
Abstract
During the SARS-CoV2 pandemic vaccines were made available at a rapid pace in the United States (US) with support from the government. In Mississippi, vaccine hesitancy was marked. Across the country many areas of the US demonstrated reduced uptake regarding this specific vaccine due to a variety of reasons. Even with the efficacy of the vaccine indicative of a significant level of protection from mortality and serious morbidity, vaccine uptake and hesitancy were a significant concern. This study surveyed Mississippians on their willingness to take the vaccine or not, and in particular, investigated political ideology as a reason for vaccine hesitancy. Data was collected via an online survey and 589 adults (>18 years) responded. Those self-identifying as “Republican” were more than twice as likely to disagree that not getting the vaccine was a risk to their health and others (OR = 2.07, 95% CI 1.70, 2.54) as those who identified as “Democrat or independent” voters. Future health promotion efforts should specifically attempt to address this group in a more effective manner.
Introduction
Vaccine hesitancy has been reported since the invention of vaccines themselves. 1 Many scourges of the last century are no longer as prevalent in the United States (US). Diseases such as smallpox have been eradicated through a robust vaccine program that eliminated the disease world-wide. 2 Polio is rarely seen in the US today, whereas in the past century people typically knew someone permanently afflicted by the virus. During the recent corona virus pandemic (COVID-19), the US ramped up vaccine research and an effective 2-dose vaccine was developed as well as a single-dose. 3 Even with the rapid development of a vaccine providing significant risk reductions in both hospitalization and mortality, many Americans would not take it. In Mississippi, the uptake was among the lowest in the country, not reaching 40% of the total state population at any time during the first or second wave. 4 In September of 2022, over 2 years after the first wave in the US, Mississippi had only 52% of residents fully vaccinated. 5
Vaccine hesitancy is defined by the SAGE Working Group for Vaccine Hesitancy as, “the delay in acceptance or refusal of vaccines despite availability of vaccine services.” 6 In 2016, Thomson et al 7 examined 43 prior studies on vaccine acceptance based on numerous variables. They assessed studies related to adult use of the influenza vaccine as well as parental choices related to childhood vaccines. Lack of trust in the government, health professionals opinions, personal views on social responsibility, and feelings of personal susceptibility to the disease were predictors of acceptance and hesitancy. Recent studies have shown that during the COVID-19 pandemic various factors likely influenced people to either accept the vaccine or remain hesitant. 8 Factors such as social media, race, gender, age, education, income, family influences, religious beliefs, politics, and other personal beliefs played a part, as did healthcare system trust and experience. 8 Specific mention was made regarding intentional disinformation spread on social media during the pandemic. Use of social media for vaccine information without a trusted source, for example, health department, physician, or the Centers for Disease Control (CDC), was associated with two-fold odds of vaccine hesitancy. Lasher et al surveyed college students in 2021 and found those being more politically conservative, and consuming right-wing news had increased vaccine hesitancy. 9 Further, Sarathchandra et al in the US developed a pre-pandemic survey instrument regarding general vaccine acceptance and noted that scientific reasoning regarding vaccines increased vaccine acceptance among liberals but decreased it among conservatives. 10 In the most recent COVID-19 pandemic, having a US president promote unproven medical cures for the virus also likely further confused the populous. 11 In addition, a specific study on COVID-19 vaccines noted that those who self-identified as Democrats politically, were less likely to reject the vaccine than those holding other political views. 12 However, Khubchandani et al in a US sample of 1878 found by late 2020, those most hesitant identified as Black or Hispanic, and those reporting children at home. 13 Political affiliations did affect the outcomes, however, with those leaning Republican being more hesitant. The current study aimed to assess vaccine hesitancy in Mississippi including whether political ideation would have an influence on vaccine acceptance or rejection. In particular, how those self-identifying as Republican would compare to Democrats and independents.
Methods
This study included adult (≥18 years of age) residents of Mississippi who were able to access the survey through electronic means and excluded those were not Mississippi residents and <18 years of age. Participants were recruited via social media, e-mail and limited community outreach opportunities facilitated by the social networks of the Mississippi INBRE Community Engagement and Training Core, 14 including the Idea Network of Biomedical Research Excellence (INBRE) Outreach Scholars program, and community-based health and outreach organizations. Upon completion of the survey, participants were offered the opportunity to receive a superstore e-gift card valued at $25. Data represented in this manuscript was collected from May to June 2021. Protocol was reviewed and approved by the University of Southern Mississippi Institutional Review Board (Protocol #IRB-21-111).
Participants completed a 98-item survey that included information regarding COVID-19 symptoms, testing and vaccination history, contextual influences, individual/group influences, and vaccine/vaccination-specific issues of vaccination uptake. Survey design constructs modeled recommendations and included items from the SAGE Working Group Report for Vaccine Hesitancy 15 as well as items from the RAND American Life Panel Impacts of COVID-19 survey 16 selected from the PhenX Toolkit version November 11, 2021 (Ver 40.4). 17 Survey items were reviewed by multiple behavioral and public health researchers, as well as healthcare organization leaders familiar with the population. IBM SPSS Statistics 27.0 (New York) was utilized to analyze preliminary descriptive data and report descriptive and frequencies of quantitative data. Odds-ratios were calculated for variables related to political ideology as well as a logistic regression model including possible affect modifiers when odds-ratios indicated associations. It should be noted that for the purpose of chi-square comparisons the investigators compared those reporting to be Republicans to both Democrats and independents due to the literature suggesting that Republicans/conservatives are more likely than others to be vaccine hesitant.
Results
Demographics
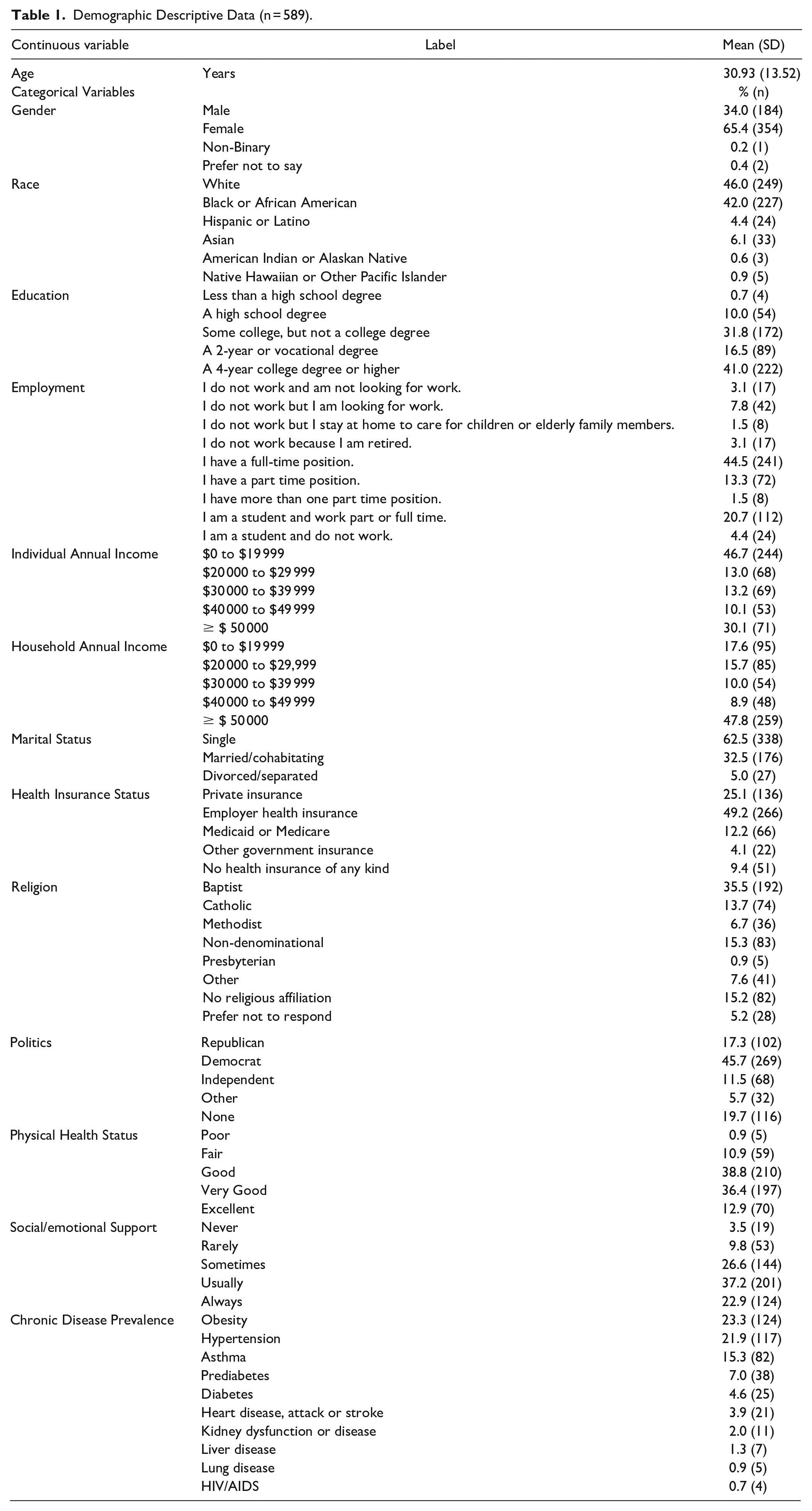
The survey sampled 589 Mississippians with an age range of 18 to 81 years. Of the respondents, more than half were female (65.4%) and identified as single (62.5%), and many reported having a full-time employed position (44.5%) and some degree of higher education. Near half of respondents reported an individual annual income of $0 to $19 999 and a household income greater than or equal to $50 000. Respondents mostly identified as either white (46.0%) or Black/African American (42.0%). Many respondents reported receiving health insurance benefits from their employer (49.2%) or private insurance (25.1%). More than two-thirds identified with a Christian-based faith. Most of the respondents (75.2%) perceived their health status as “good” or “very good.” When asked “How often do you get social/emotional support you need,” 60.1% of respondents reported always or usually. Of the conditions that participants self-reported being diagnosed with by a healthcare provider, obesity was the most common condition, followed by hypertension and asthma. It should be noted that not all respondents answered all questions. Table 1 provides further detail with regards to descriptive data.
Demographic Descriptive Data (n = 589).
COVID-19 Related Symptoms, Experiences, and Medical Care Sought Between January 2020 and September 2021
Of the participants, 60.6% reported having had COVID-19 related symptoms (including fever/chills, dry cough, sore throat, runny/stuffy nose, shortness of breath/difficulty breathing, headache/muscle/body aches, nausea/vomiting/diarrhea, loss of taste/smell, and/or fatigue). For those that reported symptoms, 68.4% of respondents went to see a healthcare professional. Of those who saw a healthcare professional for at least one of the COVID-19 related symptoms, 40.9% visited a doctor’s office, 24.0% visited an urgent care center, and 16.9% visited a drive thru clinic or testing center. About 24% of respondents reported a positive COVID-19 test and the majority of those (90.2%) tested positive with symptoms. When participants were asked about receiving the COVID-19 vaccine, 65.8% reported they had received a first dose. About 39% received COVID-19 vaccinations at the department of health drive-through site, and 58.7% received the Pfizer vaccine. Of those who were not vaccinated at the time of the survey (34.2%, n = 176), 40.0% said they were extremely unlikely to get the COVID-19 vaccine in the next 3 months. Regarding those having had the first dose of the vaccine, 81% (n = 274) of those self-identifying as Democrats had at least 1 dose at the time of the survey as compared to 38% (n = 39) of Republicans (Pearson χ2, 0.000).
Contextual Influences of Vaccine Hesitancy
The most reported primary source of information used for COVID-19 information was social media (20.5%, n = 111) followed by broadcast television (16.1%, n = 87), CDC media sites (15.7%, n = 85), and online news websites (15.3%, n = 83); 10.5% (n = 57) did not consume news about COVID-19. The most commonly reported secondary source was social media (19.8%, n = 96) followed by online news websites (15.3%, n = 74), friends, family or personal networks (13.6%, n = 66), and CDC media sites (13.0%, n = 63). When respondents were asked to rate their agreement with groups or individuals who did not agree with COVID-19 vaccinations, 59.9% of participants somewhat disagreed-to-strongly disagreed with those individuals. For those who could recall an event that discouraged them from vaccination in general in the past (not COVID-19 specific) whether they ended up receiving the vaccine or not, 42.7% recalled fear of having adverse reactions. Most of the respondents (71.9%) did not know anyone who would not get the vaccine due to religious or cultural reasons.
Nearly half of the participants somewhat agreed-to-strongly agreed that anyone who does not get the COVID-19 vaccine is risking their health and the health of others (56.1%) and that their government was making decisions in their best interest with respect to how to provide the COVID-19 vaccine (49.1%). Most of the respondents somewhat agreed-to-strongly agreed that the COVID-19 vaccine is easily available to their area (85.7%) and that the COVID-19 vaccine is accessible to them within a reasonable driving range (87.2%). About 55 to 61.8% of respondents somewhat agreed-to-strongly agreed with the positive statements regarding vaccine accessibility, safety, and healthcare provider/vaccine producer intentions.
Political Ideation and Vaccine Acceptance or Hesitancy
Political ideation was assessed by comparing those identifying as Republican directly to those who identified as Democrats or independents. The 2 named parties represent most of Mississippians who identify with a party but independent politicians have gained favor in local or state races. 18 Those identifying as Republican were twice as likely to disagree that, not getting the vaccine was a risk (OR = 2.07 95% CI 1.70, 2.54) when compared to Democrats combined with independents; were more likely to believe vaccine producers were not interested in their health (OR = 1.75 95% CI 1.44, 2.12); to disagree that not getting a vaccine is risking their health or others (OR = 2.07 95% CI 1.70, 2.54); and to agree that there are better ways to prevent the disease than a vaccine (OR = 2.07 95% CI 1.52, 2.82). In addition, those identifying as Republican were more likely to disagree that vaccines strengthen the immune system (OR = 1.53 95% CI 1.17, 2.00); to disagree with the statement that COVID-19 is a serious disease if someone gets it (OR = 2.72 95% CI 1.79, 4.14); and to disagree that it is important to get the vaccine for themselves and their family (OR = 3.15 95% CI 2.49, 3.99). Disagreement with a statement that the vaccine is safe for me and my community was also more likely among those self-identifying as Republicans (OR = 3.24 95% CI 2.51, 4.17).
Since differences were noted based on political ideology, a logistic regression model examined factors that might affect predictions on hesitancy. The investigators wanted to know if age, race, income levels, would affect political ideology as an outcome. In these assessments, those identifying as Republican and aged 18 to 49 years had an adjusted odds-ratio (AOR) of 3.32 (95% CI 1.11, 9.92) when it came to disagreement with the statement, “Not getting vaccine is a risk to self and others,” when compared to those ≥50 years. Those who were white and identifying as Republican were even more likely to disagree with the statement, “It is important to get the vaccine for self and family” (AOR = 4.28 95% CI 1.41, 13.06) than respondents in the general assessment. Related to this statement, those who were in the 18 to 49 age group were also 3.76 times more likely to disagree when this adjustment was made (95% CI 1.20, 11.77). Those with a net income of ≤$49 000 when compared to ≥$50 000 were also 3.10 times more likely to disagree with the statement, “COVID-19 is a serious disease” (95% CI 1.24, 7.62).
Discussion
As previously noted, vaccine hesitancy is not new. In addition, as we have also indicated, hesitancy based on political views or religious beliefs is not a new phenomenon either. Mississippi is primarily a Republican state, with strong evangelical beliefs and those 2 variables tend to go hand-in-hand. Especially when whites have been queried. 19 However, it should be noted that religious views did not have a statistically significant outcome in the primary assessment in this setting. In addition, minorities and in particular Black Mississippians faced poorer COVID-19 outcomes 20 so even if they self-identified as Republicans, they were perhaps still more concerned about negative health outcomes than their white counterparts in this study.
Salient to the discussion is how health education specialists and clinical providers might reach this group of Mississippians. Typically, clinical providers are the best people to cue patients to action on a preventive health measure. “Cue to action” is a construct used in the Health Belief Model originally constructed for use in education campaigns to get people to get testing or to take a vaccine. 21 Clinical providers might help if they prioritize the message to patients with added emphasis. However, they can be vaccine hesitant as well.22,23 Annual numbers of healthcare personnel taking the influenza vaccine varies but in the 2020 to 2021 influenza season, overall, about 76% of healthcare workers took the vaccine. 24 According to this U.S. Centers for Disease Control and Prevention assessment, percentages for assistants and aides decreased by 10.8% from the previous year, and among pharmacists, a group who should know of the benefits, coverage for the year decreased by 6% from the previous year. Hospital workers, where it is often mandated, had the highest percentage of coverage at 91.6% but among long-term care workers and home healthcare, the level of coverage was only 66%. There may be various factors that influence vaccine uptake among healthcare providers, but that remains beyond the scope of this study.
Trusted sources of information are critical for dissemination of public health recommendations as ideologies can influence acceptance of information. However, it has been shown that those who identify as Republican also have a greater distrust of science in general. 25 A Pew Research Center report found that 70% of Republican leaning respondents thought scientists should stay out of public policy debates and only 24% believed that scientific experts are usually better than other people at making good policy decisions about scientific issues. Two-thirds of Democratic leaning respondents felt scientists should take an active role in policy debates and 55% thought scientists made better decisions about science policy than other people. Among the Democratic leaning, 64% actually believed scientists did not have enough sway in public policy debates. The role of general acceptance of science within policy decisions is a broader issue but general acceptance levels may be playing a role in personal decision-making regarding vaccines as well. Since the Pew study, additional survey research indicated that from 2019 to 2022 the number of parents who responded that they should have more decision-making power regarding childhood vaccines increased with 44% of Republican leaning respondents stating this compared to 11% of those leaning Democratic. 26
Related to COVID-19 vaccine political polarization, at least one group has suggested that worldwide, key politicians have caused much of the polarization and that non-partisan experts might be the key to depolorization. 27 They further suggested bipartisan coalitions, using experts but also acknowledging Republican leaning members of the public have less trust in experts. Elites within one’s “in group” may more persuasive, according to the researchers, but they also thought the bipartisan nature of a group encouraging support would have better outcomes.
While health education specialist or clinical provider engagement is needed, more research on personal biases created by political beliefs related to preventive behaviors needs to be explored. The goal should be unbiased healthcare advice, based on the best available evidence that honors patient autonomy in the process as well as any discrete cultural values that influence vaccine uptake in general. Policies that allow public and population health experts to set priorities in a pandemic may be critical moving forward and unfortunately, erosion of this infrastructure has been noted at various state levels post COVID-19. 28 This will likely have to be addressed to maintain effective public health management of infectious disease. In addition, considering specific health behavioral models such as Transtheoretical Stages of Change, 29 the Health Belief Model, 21 and Theory of Reasoned Action/Planned Behavior 30 might help frame messaging in a way that does not leave out necessary interactions among people, environment, significant others, and behavior. Some models account for peer influences, social norms, and normative beliefs.
There are some limitations inherent to this study. First, those that are common to all survey research and secondary data analysis including response biases, oversampling of various groups when compared to others and questions established outside the control of the investigator. More than half of this sample was female, single, and had some college. In addition, in this sample, respondents were solicited from a community-based health and research network and word of the survey spread from there in many cases. This demographic is more likely located in university towns or towns with community-based groups involved in health or health disparities work. Those facts have impacts on the sample frame as a whole and therefore, on the outcomes. For example, the Black/African-American subset is slightly higher than what is representative of Mississippi by 4 percentage points. This could account for higher numbers of Democrats in the sample than the state average since in general, Blacks are represented in larger numbers in this party. It is also a small, Mississippi subset and should not be generalized to the entire US population.
Conclusion
Political ideology in Mississippi can have an impact on vaccine hesitancy or uptake. It is somewhat affected by age and income levels as well as race. Further studies must look at how to reach this sub-set of Mississippians in a manner that disarms previously held beliefs on science, medicine, and preventive measures such as vaccines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mississippi INBRE, funded by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes for Health under grant number P20GM103476.