
Abstract
Since the release of Healthy People 2020, there has been extensive research understanding factors associated with health-related quality of life (HRQoL) among specific populations. Despite this growing body of research, little has been conducted to understand the factors associated with HRQoL among uninsured/underinsured Americans. The purposes of the present study were to assess clinic staff to determine: (1) whether there is a need to examine HRQoL among uninsured/underinsured individuals, (2) whether there is a need for tailored HRQoL-promoting interventions among uninsured/underinsured individuals, and (3) the factors associated with HRQoL among uninsured/underinsured individuals. A survey was sent to an association of 41 clinics that provides free medical services to uninsured/underinsured individuals. The majority of participants indicated that uninsured/underinsured individuals experience unique factors associated with HRQoL and that there was a need to implement tailored HRQoL-improving interventions among uninsured/underinsured individuals. The results also present the personal/contextual factors associated with HRQoL of uninsured/underinsured individuals.
A growing number of individuals in the United States (U.S.) are at risk for poor health and are in need of adequate and affordable healthcare. The implementation of the Affordable Care Act (ACA) in 2014 reduced the number of uninsured nonelderly Americans from 44 million in 2013 to below 27 million in 2016. 1 Despite this initial victory, 2017 saw the first increase in uninsured nonelderly adults since the implementation of the ACA. This increase was followed by another increase the following year. 2 Along with these increases in the number of uninsured nonelderly adults, recent national conversations have also focused on individuals who are underinsured. These individuals have health insurance, though are at a significant financial risk when paying for health-related expenditures. Although it was initially thought that the ACA would reduce the number of underinsured adults in the U.S., 3 the number of Americans who are at serious financial risk when paying for health-related expenditures has increased from 29 million in 2010 to 44 million in 2018. 4
While healthcare reform continues to be debated in the U.S., the reality is that a growing number of Americans are finding it harder to afford adequate healthcare and those that cannot afford adequate healthcare are at risk for poor health and health disparities. In 2017, the Agency for Healthcare Research and Quality (AHRQ) released a report which concluded that many health disparities in the U.S. have worsened over time. 5 In addition to these worsening health disparities, indicators of overall public health continue to raise alarms—life expectancy in the U.S. has declined for 3 years in a row and the rates of obesity and suicide are climbing.6-8 These worsening indicators of public health highlight an urgent need to promote health among uninsured and underinsured individuals—a group disproportionately at risk for adverse health.
Health-related Quality of Life
Healthy People 2020 identified health-related quality of life (HRQoL) as an important indicator of overall public health. 9 HRQoL is a holistic and multidimensional conceptualization of health that is composed of an individual’s physical, psychological, and social functioning.10,11 It recognizes health as a product of various personal and contextual factors. This holistic understanding of health may play a role in explaining why multidimensional measures of health (e.g., HRQoL) can be more powerful predictors of adverse health outcomes than unidimensional measures of health (e.g., the presence of a chronic illness).12,13 Moreover, research also indicates that multidimensional measures of health can predict adverse health outcomes while controlling for unidimensional measures of health. 14 It is therefore alarming that surveillance data from the Centers for Disease Control and Prevention have suggested that HRQoL has decreased in recent years and not surprising that Healthy People 2020 set a national objective to improve HRQoL for all Americans.11,15
The emphasis on HRQoL, and the national goal to improve it, has been followed by an increasing amount of research assessing population-specific HRQoL. This research has been conducted among cancer survivors, 16 individuals with Parkinson’s disease, 17 caregivers of children with autism spectrum disorders (ASDs), 18 and individuals experiencing obesity. 19 Although this increase in research is much needed, there is a noticeable gap in the literature assessing the unique factors associated with HRQoL among uninsured and underinsured individuals in the U.S. This gap is alarming because health insurance status has been shown to be positively associated with HRQoL and like cancer survivors, individuals with Parkinson’s disease, caregivers of children with ASDs, and individuals experiencing obesity—20,21 uninsured and underinsured individuals likely experience unique, population-specific factors associated with their HRQoL. Although insurance status has been positively associated with HRQoL, no known research has explored the unique factors associated with HRQoL among uninsured and underinsured individuals.
Contextual Model of HRQoL
The Contextual Model (CM) of HRQoL was proposed as a model that was intentionally inclusive of cultural (e.g., acculturation) and socioecological (e.g., socioeconomic status) dimensions implicated with HRQoL—dimensions often omitted from other HRQoL models. 22 Other dimensions of the CM of HRQoL include the demographic context and the healthcare system context (e.g., access to care). 22 Each dimension directly, and through interactions with the other dimensions, impacts HRQoL. This model has been useful when working with underserved populations including uninsured and underinsured individuals,23-25 as these populations experience unique contextual factors that are often not included in traditional models and measures of HRQoL. More information on the CM of HRQoL can be found in Ashing-Giwa (2005). 22
Assessing whether there is a need (i.e., a health needs assessment) to improve HRQoL among uninsured and underinsured individuals and, if so, understanding the unique personal and contextual factors that influence HRQoL among these individuals may serve as important first steps to improving healthcare services and designing interventions to reduce HRQoL disparities. Health needs assessments are an important public health tool given the rising costs of health care services and the limited resources available to promote health. 26 These assessments can guide the allocation of limited health resources and inform intervention development and implementation strategies. 27 For example, once it is established that there is a need to promote HRQoL among uninsured and underinsured individuals, personal and contextual risk factors can be understood in order to develop and implement a tailored intervention. Tailored health promotion interventions are often preferred by both patients and providers and are effective in producing desired outcomes.28-30 Additionally, a recent review of randomized controlled trials found that tailored interventions were more likely to produce desired outcomes compared to no intervention and compared to interventions based on general guidelines.31,32 Thus, the purposes of the present study are to determine the:
Degree to which there is a need to examine HRQoL among uninsured and underinsured individuals.
Degree to which there is a need for tailored HRQoL-promoting intervention for uninsured and underinsured individuals.
And understand the personal and contextual factors associated with the:
3. Physical functioning domain of HRQoL among uninsured and underinsured patients.
4. Psychological functioning domain of HRQoL among uninsured and underinsured patients.
5. Social functioning domain of HRQoL among uninsured and underinsured patients.
Methods
The present study received institutional review board (IRB) approval at a large university located in the Southeastern United States. Participants were recruited via an email sent to the listserv of the South Carolina Free Clinic Association (SCFCA)—an association of 41 free medical clinics across 25 counties in South Carolina. Additional emails were sent to the directors of each clinic. The IRB-approved email contained a description of the project, the inclusion criteria, a description of the survey, and an assurance that all responses will be anonymous. The inclusion criteria indicated that the present study was limited to individuals who (1) self-identified as working at a medical clinic that provides services to uninsured and underinsured individuals and (2) have regular contact with uninsured and underinsured individuals.
Participants
A total of 40 participants completed the online survey. One participant was removed because they indicated that they did not have regular contact with uninsured and underinsured individuals. Of the remaining 39 participants, 29 identified as female, 9 identified as male, and 1 indicated that they would “prefer not to say.” The average age of participants was 56.86 (SD = 13.80, range = 27-72). The average number of years that the participants have worked with uninsured and underinsured was 12.2 years (SD = 11.04, range = 1-42). The majority of participants were medical providers (e.g., physicians, physicians assistants, nurse practitioners, nurses, dental hygienists; n = 19) followed by administrative and front desk staff (n = 16). The remaining participants included a medical interpreter (n = 1), grant writer (n = 1) and 2 individuals who did not specify their roles. Most participants indicated that they work at a clinic that provides services to a mix of urban and rural patients (n = 30), followed by participants who work at a clinic that provides services to only rural patients (n = 8). One respondent indicated that they work at a clinic that provides services to only urban patients. On average, the respondents indicated that the clinics see 158.51 patients per week (SD = 166.54, range = 12-600).
Procedure
The principal investigator (PI) of the present study met with the Executive Director of the SCFCA, in addition to the directors of 2 separate clinics (the 4th and 5th authors of this manuscript) that are member-clinics of the SCFCA. These individuals indicated that there was a need to examine the HRQoL among the patients at their clinics. Although focus groups were proposed, the two clinic directors indicated that they expected a better response rate if a brief survey was sent via email. They highlighted the time constraints experienced by those working at the free medical clinics as being a barrier to participation in focus groups. Based on their input, a survey consisting of open-ended and close-ended questions was created by the PI. The PI then sent the survey to the two clinic directors for their input. Both clinic directors indicated that they found the survey satisfactory.
The survey began with an easy-to-understand written definition of HRQoL, in addition to a depiction of HRQoL that also served to explain the present study. The depiction of HRQoL consisted of 3 circles identified as representing each of the 3 domains of HRQoL (i.e., physical functioning, psychological functioning, and social functioning) with arrows pointing from each circle towards a central circle identified as HRQoL. Additionally, the 3 circles identified as representing each of the 3 domains of HRQoL had 3 separate circles pointing towards each of them containing a question mark. The question marks indicated that the present study was interested in the personal and contextual factors associated with each of the domains of HRQoL.
The survey consisted of 16 questions, 4 open-ended questions and 12 close-ended questions. Three of the 4 open-ended questions asked the participant to identify specific factors associated with each domain of HRQoL (i.e., physical functioning, psychological functioning, and social functioning). The 4th open-ended question was an optional question that asked participants if they had any other comments about HRQoL among uninsured and underinsured patients. The 12 close-ended questions assessed: (1) whether or not the participant has regular contact with uninsured and/or underinsured individuals; (2) participant role at the clinic; (3) type of patients seeking services at the clinic (eg, urban, rural, mix); (4) estimate of patients who are urban and rural; (5) average number of uninsured and underinsured patients seen at the clinic per week; (6) degree to which there is a need to examine HRQoL among uninsured/underinsured individuals (Likert-type responses ranging from Strongly disagree to Strongly agree); (7) degree to which uninsured and underinsured individuals experience unique factors that influence their HRQoL (Likert-type responses ranging from Strongly disagree to Strongly agree); (8) degree to which there is a need for tailored HRQoL-promoting interventions among uninsured and underinsured individuals (Likert-type responses ranging from Strongly disagree to Strongly agree); (9) participant gender; (10) participant age; (11) number of years that the participant has been working with uninsured/underinsured individuals; and (12) zip code of the clinic.
Results
The Degree to Which There is a Need to Examine HRQoL among Uninsured and Underinsured Individuals
The majority of participants (n = 24; 61.54%) responded that they strongly agreed with the following statement: “Please rate the degree to which you agree or disagree with this statement: There is a need to examine health-related quality of life among uninsured and underinsured individuals.” Of the remaining participants, 11 (28.21%) indicated that they agreed with the statement and 4 (10.26%) indicated that they strongly disagreed with the statement.
The Degree to Which There is a Need for Tailored HRQoL-promoting Intervention for Uninsured and Underinsured Individuals
The majority of participants (n = 26; 66.67%) responded that they strongly agreed with the following statement: “Please rate the degree to which you agree or disagree with this statement: There is a need for interventions to improve health-related quality of life that are tailored to the specific needs of uninsured and underinsured individuals.” Of the remaining participants, 10 (25.64%) indicated that they agreed with the statement, 1 (2.56%) indicated that they were unsure about the statement, and 2 (5.13%) indicated that they strongly disagreed with the statement.
Qualitative analytic methods
The qualitative analysis for the present study relied upon a grounded theory approach in that the results were determined from an inductive method of analysis that allowed individual data points to inform the creation of larger constructs. Specifically, the qualitative analysis for the present study utilized the constant comparative method. The constant comparative method is a grounded theory approach wherein individual participant responses are used to generate themes by determining patterns of responses and categorizing the responses into themes by constantly comparing the individual responses to the themes, and generating new themes as needed, in order to sort all of the responses into themes. 33
The PI for the present study first organized the qualitative responses from the participants into a spreadsheet in order to facilitate the analyses. Specifically, the responses were categorized according to the research question to which they were responsive (i.e., factors impacting physical functioning, factors impacting psychological functioning, and factors impacting social functioning). Each individual response is called an “instance.” Next, 2 research team members independently reviewed the list of instances for each research question and assigned themes using the constant comparative method of analysis as described above. The 2 research team members then compared their themes with one another to determine a list of final themes (i.e., an agreed-upon list of the themes that both research team members would then use to code the instances in the final stage of analysis).
Finally, the 2 research team members independently applied the list of final themes to the list of instances once again. They then compared their list of themes with one another to determine the final results of the study. A third team member resolved any discrepancies in the themes assigned by the 2 initial researchers (i.e., in the case where the final applied codes by each of the 2 team members did not match, the third team member decided what code applied for the final results). After this coding process was concluded, the third team member calculated the inter-rater reliability by first determining the percent agreement between the 2 raters and then calculated the kappa statistic, which takes into account the incidence of chance agreement between raters.
Personal and Contextual Factors Associated with the Physical Functioning Domain of HRQoL among Uninsured and Underinsured Patients
The most prevalent themes as identified by the participants in response to this research question were Physical Environment, Low Socioeconomic Status, and Poor Access to Healthcare. The inter-rater reliability for the analysis of this research question (percent agreement = 76, kappa = 0.74) was considered acceptable according to most standards.34,35 A full list of results for the third research question is available in Table 1. Example instances of the most prevalent themes and the “other” theme are available in Table 2.
Physical Functioning Themes.

n indicates the total number of instances that were coded under the theme.
Physical Functioning Example Instances.

Personal and Contextual Factors Associated with the Psychological Functioning Domain of HRQoL among Uninsured and Underinsured Patients
The most prevalent themes as identified by the participants in response to this research question were Low Socioeconomic Status, Affective Disorders, and Other. The inter-rater reliability for the analysis of this research question was considered acceptable (percent agreement = 75, kappa = 0.72). A full list of results for the 4th research question is available in Table 3. Example instances of the most prevalent themes and the “other” theme are available in Table 4.
Psychological Functioning Themes.

n indicates the total number of instances that were coded under the theme.
Psychological Functioning Example Instances.

Personal and Contextual Factors Associated with the Social Functioning Domain of HRQoL among Uninsured and Underinsured Patients
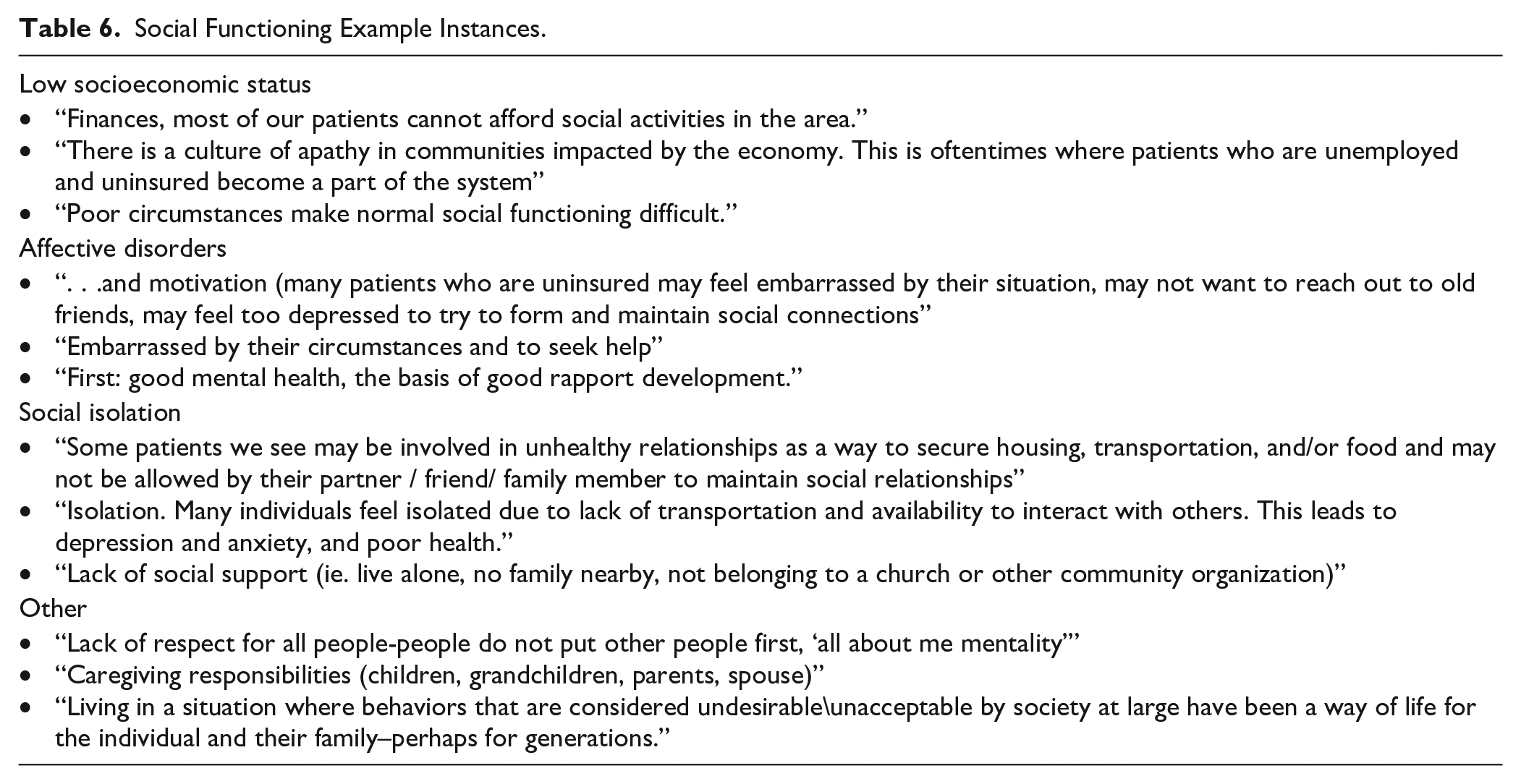
The most prevalent themes as identified by the participants in response to this research question were Low Socioeconomic Status, Affective Disorders, and Social Isolation. The inter-rater reliability for the analysis of this research question was considered moderate (percent agreement = 64, kappa = 0.59). A full list of results for the 5th research question is available in Table 5. Example instances of the most prevalent themes and the “other” theme are available in Table 6.
Social Functioning Themes.

n indicates the total number of instances that were coded under the theme.
Social Functioning Example Instances.
Discussion
Uninsured and underinsured individuals are at an increased risk for poor health outcomes and consequently diminished HRQoL.4,20,21 Despite the current body of research seeking to understand the factors associated with HRQoL among diverse individuals, relatively little research has been conducted to understand the factors associated with HRQoL of uninsured and underinsured individuals. This paucity of research has resulted in a dearth of information regarding the unique personal and contextual factors that may influence the HRQoL of this group. The present study addressed this gap in the research and explored the beliefs of providers and office staff employed at clinics who serve uninsured and underinsured individuals regarding (1) the need to examine HRQoL among uninsured and underinsured individuals, (2) the need for tailored HRQoL-promoting interventions for uninsured and underinsured individuals, and (3) the personal and contextual factors associated with the specific domains of HRQoL functioning (i.e., physical, psychological, and social functioning) that impact uninsured and underinsured patients.
Overall, nearly 90% of the participants agreed with the statement that there is a need to examine HRQoL among uninsured and underinsured individuals. Similarly, the vast majority of participants agreed that there is a need to develop tailored HRQoL-promoting interventions for uninsured and underinsured individuals. The results suggest that the providers and staff at the clinics surveyed likely believe that the development and implementation of a HRQoL-promoting intervention for uninsured and underinsured individual is an appropriate allocation of resources—though the type and amount of resources are unknown and warrant a future study. Such a study will fill a growing gap in care of this population—a population that is increasing and that experiences low HRQoL.4,36,37 Although to the authors’ knowledge there is little research exploring the development, implementation, and efficacy of HRQoL interventions tailored for uninsured and underinsured individuals, the evidence examining the efficacy of tailored health promotion interventions for specific populations (e.g., racial/ethnic minorities) is promising.27-29
The present study also examined the personal and contextual factors associated with the specific domains of HRQoL (i.e., physical, psychological, and social functioning) among uninsured and underinsured individuals. The results of the qualitative analysis highlighted the prevalent factors with respect to each domain—factors that have been unexplored in the literature. Although the participants identified several factors impacting the HRQoL among uninsured and underinsured individuals with regard to their physical functioning, the most prevalent factors within this category include: physical environment, low socioeconomic status (SES), and poor access to healthcare. Likewise, numerous factors associated with psychological functioning emerged. The 3 main factors included: low SES, affective disorders, and “other.” The “other” factor included diverse themes such as the negative impact of poor sleep on health, personal conceptualizations of when insurance may be needed, and limitations in the ability to engage in health-promoting behaviors such as physical activity. Finally, participants expressed the belief that low SES, affective disorders, and social isolation were prominent factors associated with social functioning among uninsured and underinsured individuals.
Interestingly low SES was the only factor that participants identified as impacting all 3 domains of HRQoL. SES is a known social determinant of health and low SES has been related to poor health outcomes and diminished HRQoL.38,39 Low SES is a pervasive risk factor for poor health outcomes influencing several domains of HRQoL including physical, psychological, and social functioning.39,40 The results of the present study highlight the overarching nature of low SES and its potential impact on the HRQoL of uninsured and underinsured adults, as it was the most frequently cited factor (52 instances). Despite the complexity and intractability of SES in the U.S., health care providers and public health experts can design interventions and advocate for resources in their communities to target components of SES (e.g., income, education, employment) in order to mitigate the impact of these components and improve the HRQoL of uninsured and underinsured individuals.
A similar pattern emerged for affective disorders (i.e., mental health disorders often characterized by a disturbance/change in mood status such as depression and mania), which was identified as a major factor contributing to the psychological and social functioning of uninsured and underinsured individuals. The results suggest that uninsured and underinsured individuals experience adverse mental health and that this adverse mental health impacts their psychological and social functioning. These results are worrisome because it is known that poor/limited access to mental health care can exacerbate psychopathology and diminish quality of life.41,42 Additionally, a significant barrier to obtaining adequate mental health care is insurance status.42,43 Despite the barriers to obtaining adequate mental health care associated with insurance status, providers attending to uninsured and underinsured individuals may promote HRQoL by focusing on mental health concerns with their patients, in addition to guiding these patients to resources available in their community.
The results of the present study highlight important factors which are likely to negatively impact the HRQoL of uninsured and underinsured individuals. Some of these factors may be viewed as individual-level and personal (e.g., affective disorders, health literacy, social support), while others may viewed as community-level and contextual (e.g., low SES, poor physical environment). This mix of personal and contextual factors suggest that novel and innovative multi-level HRQoL-promotion interventions are needed to address the unmet and growing health needs of uninsured and underinsured individuals in the U.S. In order to design such a comprehensive HRQoL intervention, input from community-based collaborations, in addition to interdisciplinary teams are needed. Another important finding of the study is that many of the factors impacting HRQoL among uninsured and uninsured individuals (e.g., SES and affective disorders) are represented across multiple domains, highlighting the interconnectedness of the HRQoL domains.
The results of the present study should be interpreted with some caution. The study solely consisted of participants who work at clinics that provide services to uninsured and underinsured individuals in South Carolina (SC), thus limiting the generalizability of the results given that the health uninsurance rate is high in SC and, as reflected by the location of the participants of the present study, is mostly rural. Moreover, it is noteworthy that despite having a high health uninsurance rate, SC has a well-established association of free medical clinics (i.e., SCFCA). Therefore, the HRQoL of the uninsured and underinsured in SC may be different than that of individuals residing in other states—states with less opportunities for charitable healthcare for the uninsured and underinsured. The results should also be viewed with some caution given that they are provider and clinic staff-identified factors associated with HRQoL among uninsured and underinsured individuals as opposed to factors identified by the uninsured and underinsured individuals themselves. Furthermore, as with all data analyses, there may be some concern with unconscious bias in the interpretation of results. Though it should be noted that responses were independently analyzed by 2 team members and results were reviewed by the 4th and 5th authors—directors of 2 SCFCA member-clinics. Despite these limitations, there is strong support for future studies to examine factors associated with HRQoL among patients who are uninsured and underinsured and from other high-risk groups, factors associated with HRQoL as identified by the patients themselves, and more robust designs (e.g., those that integrate quantitative and qualitative approaches).
The present study is important and is a valuable contribution to the limited body of research that has focused on understanding the HRQoL of an at-risk group. To the authors knowledge, this is one of the first studies seeking to understand the factors associated with HRQoL among uninsured and underinsured individuals—a growing and diverse patient population representing more than 20 million U.S. adults.1,4 Although the provision of universal health insurance will likely improve the HRQoL of uninsured and underinsured individuals, it is unreasonable to expect such a change in the U.S. in the near future. Given the worsening health disparities in the U.S., 5 it is clear that the health of at-risk groups cannot wait for such changes. Therefore, the burden lies on the shoulders of health care providers such as nurses, physicians, and psychologists and public health researchers to improve HRQoL among uninsured and underinsured individuals. The results of the present study have important implications for health service providers, public health policies, and HRQoL-promotion interventions and suggest a need for comprehensive and creative health approaches, policies, and interventions focused on addressing the unique personal and contextual needs of uninsured and underinsured individuals. Such approaches, policies, and interventions should be implemented at institutional, state, and ideally federal levels in order to mitigate the pervasive impact of poor HRQoL among at-risk groups such as those who are uninsured and underinsured.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the publication of this article from the University of South Carolina University Libraries’ Open Access Fund.