
Abstract
Utilization of telehealth modalities to provide cognitive and behavioral therapies is rapidly increasing. Limitations to access to care can prohibit individuals from getting the care they need, especially evidence-based treatments. In the U.S., Veterans are a population in great need of accessible and high-quality evidence-based psychotherapy for insomnia, as it often co-occurs with other common syndromes such as depression and PTSD. Cognitive Behavioral Therapy for Insomnia (CBT-I) offers effective treatment for insomnia and can be delivered via telehealth and in a group format to greatly increase availability and accessibility. To date, however, few programs exist offering telehealth-to-home CBT-I, fewer still are offered in a primary care setting, and none to our knowledge are offered in group format. We examine the feasibility and efficacy of a fully telehealth-to-home (TTH) group CBT-I pilot program in primary care and compare primary outcomes to those seen in a face-to-face (F2F) format as well as meta-analytic studies of group CBT-I. Primary endpoints, as typically defined such as sleep efficiency (SE) and scores on the insomnia severity index (ISI) appear comparable to those seen in F2F groups in our clinic, and to outcomes seen in the literature. We discuss challenges and strategies for successful implementation of such a program in integrated primary care to increase access and availability of this evidence-based treatment.
Introduction
Access to evidence-based mental health care has become more restricted with the onset of the COVID-19 pandemic. Psychological distress related to COVID-19 has increased common mental health syndromes (eg, depression, anxiety) 1 and related behavioral health issues, such as insomnia. 2 Recent data suggest COVID-19 worry is significantly associated with increased insomnia and suicidal ideation. 3
The devastating effects of COVID-19-related distress are likely exacerbated in veterans, 4 who have over 6 times higher rates of insomnia than the general population. 5 Recent research estimated that new or exacerbated insomnia symptoms occurred in 20% of Veterans during the first year of the pandemic. 6 By extension, mental health symptom severity is likely increasing in this population, as insomnia is associated with increased depressive 7 and trauma 6 symptomatology.
Behavioral sleep medicine is a front-line treatment for insomnia. CBT for insomnia (CBT-I), a multi-component intervention targeting psychological, behavioral, and physiological factors associated with the perpetuation of insomnia, has the strongest evidence base. CBT-I has demonstrated short- and long-term efficacy across modalities and settings, including individual 8 and group formats, 9 via telehealth,10,11 and in primary care settings. 12 Scoping reviews of CBT-I support its effectiveness in treating insomnia in individuals with co-morbid psychiatric 13 and medical conditions. 14
Since 2011, CBT-I has been a part of the VA National Telemental Health Program (NTMHC)—a scalable program designed to increase access to evidence-based mental health treatment across facilities in remote/rural communities, and in urban environments with limited resources. Veterans can attend treatment sessions hosted by experts elsewhere by visiting their nearest VA community-based outpatient clinic. CBT-I via telehealth has evidence of clinically and statistically significant effectiveness.15,16 However, existing clinic-based telehealth programs still require Veterans to locate, access, and attend telehealth sessions in an outpatient clinic office.
Since the onset of the COVID-19 pandemic, patients are increasingly being offered the option to attend telehealth appointments from their home. This shift has both challenges and advantages, prompting innovation to meet the needs of patients. Offering CBT-I using telehealth-to-home (TTH) format requires attention to common telehealth barriers (eg, appointment coordination, overcoming the digital divide), and unique challenges, such as the coordinated and secure transmission of sleep logs and insomnia measures. To date, a TTH format for CBT-I has only been implemented on a small scale, using a one-on-one therapy format. 17
We conducted a feasibility pilot of a fully TTH CBT-I group program within a large outpatient primary care clinic through integrated behavioral health in primary care at the VHA. This paper highlights the importance of offering TTH group-based CBT-I in primary care and describes its unique benefits and challenges. We then present preliminary data from a small trial comparing TTH to in-person CBT-I groups offered at the same Community-Based Outpatient Clinic (CBOC) before the pandemic.
Methods
Participants and Setting
This study was conducted within the primary care mental health integration (PCMHI) model at a large VA primary care clinic in the southwest United States, which serves approximately 22,000 Veterans per year. With the onset of the pandemic, groups previously held in-person were adapted to a fully telehealth-to-home format, where patients participated from home and the group facilitators participated either from their designated telehealth locations (typically their home) or from the clinic. Groups were conducted via the VA encrypted videoconferencing platform “Virtual Care Manager” (VCA), which allows for synchronous group audio/video communication and reminder notifications. See Tables 1 and 2 for participant demographic data.
Participant Characteristics (Total Recruited).

Participant Characteristics (Group Participants).

Procedure
Prior to the start of the group, each Veteran received intervention materials and relevant handouts via secure messaging or encrypted email. After orientation, each group member completed a sleep log, which was reviewed in the subsequent session and served as the basis for recommendation to sleep adjustments. Data were collected via chart review.
Intervention
The CBT-I group protocol in this clinic is an adaptation of the VA protocol published by the Veteran’s Health Administration18,19 and used in previous studies (eg, Gehrman et al 2016). See Table 3 for a brief session-by-session description. We found that group members needed more education and assistance to use telehealth technology and added a “session 0” digital health literacy session to the group TTH protocol.
Description of CBT-I Group by Session.
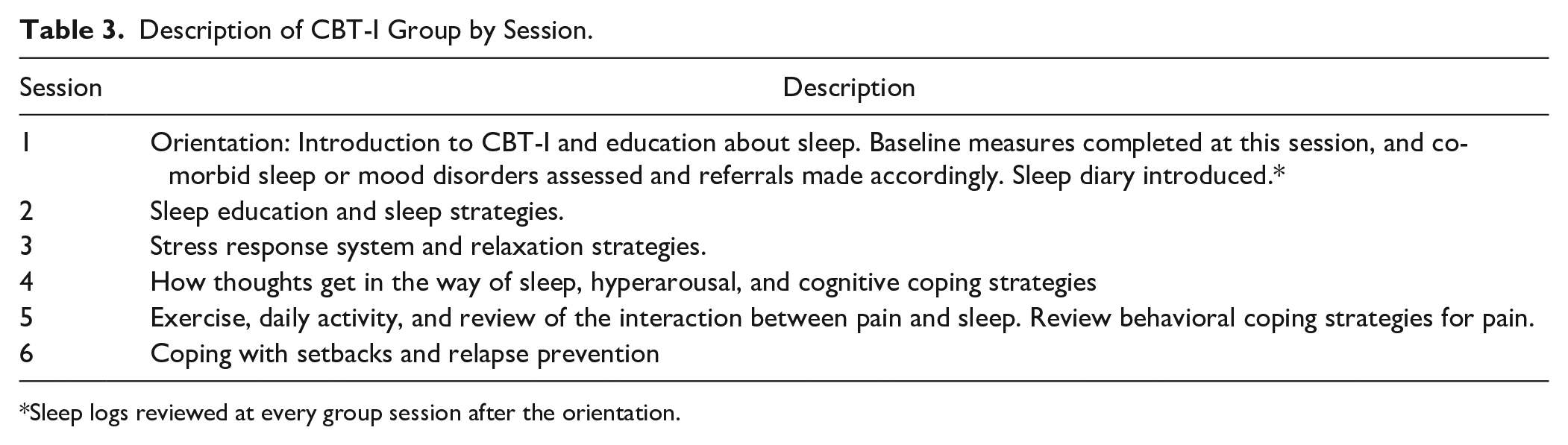
Sleep logs reviewed at every group session after the orientation.
Quantitative Outcomes
We collected data on enrollment, retention, completion, and subjective acceptability of the TTH format. Enrollment was the number of individuals who enrolled and intended to participate in first group session (eg, did not cancel before first meeting). Retention was the number of individuals who participated in the first or second session. Completion was the number of individuals who completed at least 4 sessions. The 4-session threshold was determined as number of sessions needed for adequate data (eg, at least 2 ISI measures, at least 2 completed sleep diaries) for that patient. Subjective acceptability was measured via a structured exit interview form containing Likert-type questions about the group format and modality.
Patients completed the Insomnia Severity Index (ISI), a 7-item inventory assessing insomnia symptoms, at the initial and final sessions. 20 Sleep diaries documented time to bed, estimated time in attempting to go to sleep, estimated time taken to fall asleep, total time spent awake in the middle of the night, final wake time, final time out of bed for the day, total sleep time, and sleep efficiency.
Qualitative Outcomes
Participants provided open-ended feedback to the group leader regarding their satisfaction with the group content and technological process at the end of each session.
Results
Feasibility
N = 27 Veterans completed at least 4 sessions of the 6-session CBT-I group either through TTH (n = 15) or F2F (n = 12). Enrollment was 66% in TTH and 71.4% in F2F. Retention was 57% in TTH and 56% in F2F. Completion in TTH and F2F was 75% and 70% respectively. On average, 3.77 TTH participants attended at least 1 session, compared to 3.07 in F2F. In both groups, modal number of group sessions attended was one.
A common technological barrier was access to a device with a camera. We leveraged the VA digital divide program to send tablet computers to Veterans for clinical use. However, even with a tablet, some struggled to access the conference room, set up secure messaging, or complete and return the online forms. On occasion, Veterans had participation complications otherwise not seen in other modalities of CBT-I, such as not having adequate privacy, or multi-tasking (eg, smoking, eating, or even driving while logged in).
Acceptability
Veterans in TTH were asked to complete exit interview surveys regarding their experience of the program. Results from 4 exit interviews indicate high satisfaction with the TTH CBT-I program. On average, participants strongly agreed that the program helped them sleep better or reduced their reliance on sleep medication. They also indicated they found meeting in a group was valuable and enjoyed having group over telehealth versus in-person. One Veteran noted an added benefit was “being able to attend from home and avoid traffic.” Another stated that it was “more casual and pleasant to learn from home without commuting” but also noted that the group experience was largely lost as the group had reduced to only 2 participants.
Symptom Change
Mean ISI score in TTH at baseline was 19.0, indicative of moderate severity insomnia. Mean ISI score decreased to 13.29 (M = 5.71, SD = 6.9, P < .01, d = 0.827), representing mild or subthreshold insomnia. In F2F (N = 12), mean ISI score at baseline was 21.4 (moderate-severe insomnia and decreased to 15.6 (moderate insomnia) (M = 5.8, SD = 6.2, P < .01, d = 0.939). Comprehensive outcome measures for the TTH and F2F groups are displayed in Tables 4 and 5 respectively.
Outcome Measures for TTH Group (n = 15).

Outcome Measures for F2F Group (n = 12).

We also compared the outcomes of TTH and F2F against comparable studies of CBT-I outcome in the literature. Effect sizes of the TTH group, the F2F group in our clinic, and a comprehensive meta-analysis of group CBT-I 9 are shown in Figure 1. Effect size for the reduction of subjective insomnia symptom severity was highly comparable across these 3 groups (TTH, F2F, and the Koffel study). Of note, the meta-analysis uses the Pittsburgh Sleep Quality Index (PSQI) rather than the ISI; however, they measure similar sleep constructs and both show good sensitivity to change (for review see Omachi 21 ). Reduction in insomnia symptom effect sizes here, as measured by the ISI (TTH: d = 0.83, F2F: d = 0.94) were comparable to sleep quality, as measured by the PSQI by Koffel et al (d = 0.85). Sleep onset latency (SOL) and wake after sleep onset (WASO) showed moderate to strong effect sizes across groups, with SOL being highest in the TTH group and WASO being highest in the Koffel et al study. In sleep efficiency (SE), the F2F and Koffel et al study showed large effect size changes, while the TTH study showed medium effect size. Finally, for TST, there was a small to moderate effect size for increased TST in the Koffel group, and a medium effect size for reduction in TST for the F2F and TTH group.

Comparison of CBT-I treatment effect sizes to meta-analysis of CBT-I groups.
Discussion
The purpose of the current feasibility pilot study was to determine whether there is sufficient preliminary evidence to support the ongoing use of group TTH CBT-I in integrated primary care behavioral health. Thirty percent of initially enrolled individuals completed most or all sessions in the TTH groups, similar to the F2F group. Outcome behavioral sleep data in patients completing at least 4 TTH sessions are comparable to in-person outcomes, and comparable in effect size to group CBT-I observed in a meta-analysis of controlled trials of F2F CBT-I groups. 9 Although this informal comparison of effect sizes is not as informative as direct statistical comparison of outcomes, it does appear that the TTH group retains many of the robust clinical effects widely demonstrated in CBT-I treatment.
The VA has been investigating engagement and outcomes of evidence-based psychotherapy delivered via telehealth for many years, and rapidly expanded its outreach during the COVID-19 pandemic. Multiple studies document positive treatment outcomes for PTSD depression, anxiety, and show corresponding positive qualitative feedback.22–24
This has also been extended to CBT-I in a group format with a Veteran sample; however, as mentioned previously, this was conducted in a clinic where patients were in a group room together and the clinician utilized telehealth from another clinical site (Gehrman et al. 15 ). To our knowledge, this is the first study examining telehealth delivery to the home, thereby eliminating all transportation, distance, and logistical barriers.
The TTH CBT-I group offers many benefits to telemedicine more broadly (eg, Aboujaoude et al. 25 ) while producing largely equivalent effect sizes in insomnia severity outcomes (eg, ISI scores in TTH d = 0.827, F2F d = 0.939). In our experience, the TTH CBT-I group offers the benefits of synchronous therapy, while reducing barriers, and, in this case, limitations due to public health-related precautions (eg, COVID-19 safety protocols). The addition of the “session zero” may improve telehealth technology literacy among patients who might otherwise shy away from a technology-based modality, paving the way for easier access to other clinical services that may also utilize telehealth.
In addition to replicating large effect sizes and innovation of telehealth delivery, it is important to note the implications of employing CBT-I TTH group in primary care. Although insomnia is highly prevalent in community and Veteran populations (10% and 26% respectively), is a known risk factor for psychiatric disorders, and is likely exacerbated by COVID-19, it is often under- assessed nor addressed with first-line treatments such as CBT-I. 26 Within the VA, primary care mental health integration (PCMHI) is intentionally embedded within the primary care environment to increase access, decrease stigma, and address behavioral health concerns during primary care encounters. Despite this being an ideal environment and pathway to CBT-I treatment, few studies examine PCMHI telehealth service delivery in general (eg, Owen et al., 2019), 27 or sleep interventions specifically. This study highlights the importance of investigating front-line treatments for insomnia within the primary care environment. TTH services can expand the number effective and scalable options for patients, providers, and overall system access.
Practice Suggestions and Lessons Learned
The primary challenge for TTH groups was attrition (both in enrollment at session one, and retention through at least 4 sessions) due to technological barriers. CBT-I is a resource- and paperwork-intensive program (eg, daily sleep diary, weekly measure completion, weekly practice of coping skills with handouts). Group participants who were unable to complete the sleep diary or were unable to return it to the group leaders may have discontinued the group out of frustration.
To increase technology literacy and ease of use, we piloted a 60-min virtual introduction class, or “session zero.” This class: (1) allows for participants to practice and trouble shoot using the teleconferencing system on their device, (2) provides participants with a full description of CBT-I, and time commitments, and (3) allows participants to complete initial CBT-I inventories and questionnaires before session one of the intervention protocol. Anecdotally, inclusion of a session zero improved retention from approximately 35% to approximately 50%.
Limitations
As a process-oriented clinical study of archival chart data, this study has several natural limitations. Foremost, the limited sample size for this study allows for results to be interpreted as a proof-of-concept only. To reliably assess comparisons between TTH and F2F groups, a larger sample size is warranted, and is planned for future study as more data are acquired. Similarly, this was a naturalistic study without the level of methodological control seen in a pre-planned clinical trial design. Participants were not randomly assigned to each group, nor was there a mechanism to screen for possible third variables (eg, sleep medication changes). A randomized clinical trial is necessary to accurately determine the extent and reliability of the effectiveness of CBT-I in the TTH format. We examined outcomes after session 4 of CBT-I and although it is reasonable to assume that individuals who have improved at session 4 will also show improvement at session 6, this cannot be guaranteed. Finally, the archival nature of the study did not allow for us to control for comorbid psychiatric or physical health diagnoses, other concurrent treatments, or presence of any provider-driven differences in effectiveness of CBT-I delivery. The sample was also limited regarding diversity in ethnic, racial, gender, and sexual orientation and may limit generalizability of findings.
Future Directions
Future research designs should investigate TTH format of CBT-I through randomized clinical trials with controlled samples. This would substantiate the findings found here to be causally related to changes within CBT-I treatment. Further exploration of how this format may remove barriers (eg, transportation, time) and be applied to other high-need samples such as low-resourced rural and urban populations, is needed. Lastly, we recommend further investigation of digital health literacy additions as done here in “session zero,” and how they may augment the outcomes of telehealth interventions. Additional qualitative and acceptability components may also be helpful as the field expands to the patient’s home environment, which may open opportunities to involve social supports within the home.
Conclusion
The current study examined the feasibility and acceptability of a primary care-based telehealth to home CBT-I intervention and assessed change in insomnia symptoms in both TTH and F2F groups. When comparing effect sizes for TTH CBT-I to F2F CBT-I (as well as meta-analytic findings related to sleep outcomes), effect sizes were equivalently high (eg, change in ISI scores in TTH d = 0.827, F2F d = 0.939). Thus, the available evidence suggests that ongoing use of this modality is appropriate and helps deliver the well-established CBT-I treatment in a scalable format with positive insomnia reduction outcomes and patient feedback.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.