
Abstract
Objective
This study aimed to assess whether a second course of digital cognitive behavioral therapy for insomnia (dCBT-I) could benefit patients with chronic insomnia who had suboptimal responses to the initial fully self-guided dCBT-I.
Methods
Building on a previous randomized controlled trial (RCT), participants with an Insomnia Severity Index (ISI) score ≥8 at 6 months after completing the initial digital CBT-I therapy were invited to enroll in the second phase of the study. Among the 20 eligible participants, 9 received a second round of digital dCBT-I therapy, 6 participated in follow-up only. Primary outcomes included changes in ISI scores and ISI remission rates (defined as ISI <8). Secondary outcomes included sleep attitudes and beliefs, as well as mental health questionnaire scores.
Results
Among patients who did not achieve full remission after the first course of digital CBT-I, 44.4% and 62.5% of participants experienced a reduction in their ISI scores to <8 following the second course of treatment and at the 3-month follow-up, respectively. Following the second treatment, ISI scores showed a trend of continued decrease, but no statistically significant difference was observed compared to the baseline before the second treatment (p > 0.05). Sleep-related attitudes and beliefs, as measured by the DBAS-16 scale, also significantly improved after the second round of treatment (p < 0.05). At the 3-month follow-up, the second treatment group showed a greater improvement in ISI scores (3.00(1.25, 5.00)) compared to the follow-up only group (−1.50(−3.25, 0.50)) (p < 0.05).
Conclusion
The present study suggests that a second course of digital CBT-I may benefit chronic insomnia patients who initially fail to achieve ISI remission after the first round of self-guided digital CBT-I. However, larger randomized controlled trials are needed to definitively assess its effectiveness.
Keywords
Public interest summary
This study explored whether a second course of digital cognitive behavioral therapy for insomnia (CBT-I) could help individuals who did not fully benefit from the first round of treatment. The findings showed that for some participants, repeating the digital CBT-I led to improvements in sleep quality and a reduction in insomnia symptoms, with continued benefits 3 months later. While the results are promising, the study suggests that larger trials are needed to confirm if this approach could be effective for a broader group of people with chronic insomnia.
Background
Cognitive behavioral therapy for insomnia (CBT-I) is the first-line treatment for chronic insomnia. 1 With the advancement of internet and digital technologies, digital CBT-I has gained increasing popularity which can provide standardized professional services without being constrained by geography, time, or the availability of a therapist.2–5 Many studies have shown that digital CBT-I is effective in improving insomnia.2,3,5 In contrast to traditional face-to-face CBT-I, digital CBT-I is delivered online through websites, mini-programs, or apps in a fully automated manner.6–8
Traditionally, CBT-I requires only one intervention course, which aligns with the CBT-I design. This design aims to provide a systematic intervention that alters cognitive and behavioral patterns, teaching patients how to manage their sleep and maintain healthy, long-term, sleep habits.9,10 CBT-I demonstrates durable treatment effects, with research evidence indicating it can persist for up to 24 months post-treatment.11,12 Typically, a second round of CBT-I is unnecessary.
However, for digital CBT-I, especially fully self-guided digital CBT-I, the situation may be different. In fully self-guided digital CBT-I, due to varying levels of understanding of the CBT-I content and unfamiliarity with the software, ensuring that all patients fully understand the content and follow the instructions as required during their first use is challenging. Although continuous improvements are being made to make digital CBT-I easier to understand, such as simulating a doctor–patient conversation, as in our randomized control trial (RCT), 3 it is still not possible for patients to discuss their understanding of certain content or address treatment-related doubts with a therapist as they would in face-to-face sessions. The combination of these factors may have led to suboptimal results in some patients after the first round of digital CBT-I. Currently, it remains unclear whether a second round of digital CBT-I could benefit patients who did not achieve clinical remission for the first time. Therefore, we conducted this study to evaluate the efficacy of repeated self-guided digital CBT-I treatments, based on the hypothesis that increased familiarity with the process and content may further enhance the treatment outcomes of a second round of digital CBT-I.
The participants in this study were drawn from our previous RCT. 3 We selected participants who still had an Insomnia Severity Index (ISI) score of ≥8 points 6 months after completing the first round of digital CBT-I. (Participants achieving remission on the ISI are defined by a total score below the clinical cutoff of 8 points).13,14 Participation in the second round of digital CBT-I treatment or only in the follow-up was based on the participants’ willingness. The primary outcome measure was the ISI, and other outcome measures included scores from related mental health scales. The aim of this study is to provide evidence for the efficacy of a second round of self-guided digital CBT-I treatment.
Materials and methods
Study design
This study selected participants who had received digital CBT-I but still had an ISI score of ≥8 points at the end of a RCT study (6 months post-intervention). Participation in the second round of digital CBT-I treatment or only in the follow-up was based on participant willingness. The primary outcome measure was the ISI; other outcome measures included related scales including DBAS-16, FSS, GAD-7, and PHQ-9. This study was approved by the Human Ethics Committee of Peking University First Hospital. Written informed consent was obtained from all the participants.
Participants
The participants in this study were drawn from a previous RCT (ClinicalTrials.NCT04779372). 3 The previous trial aimed to investigate the efficacy of digital cognitive behavioral therapy (digital CBT-I) delivered through a smartphone application for insomnia. Participants for the current study were selected from the original RCT participants who had an ISI score ≥8 at the end of the study.
Those participants with a residual ISI≥8 could choose whether to undergo a second round of digital CBT-I, participate in follow-up without intervention, or not participate.
Participants in the second digital CBT-I group underwent a second round of digital CBT-I treatment, followed by a 3-month follow-up. Participants in the follow-up-only group did not receive the second treatment, but attended a 3-month follow-up.
Interventions
The self-guided digital CBT-I was delivered through a smartphone-based app.
Outcomes
The primary outcome was the total ISI score. The ISI is commonly used questionnaire to evaluate insomnia severity. Severity was classified into four categories: No clinically significant insomnia (0–7 points), subthreshold insomnia (8–14 points), moderate clinical insomnia (15–21 points), and severe clinical insomnia (22–28 points).
Secondary outcomes included: sleep-related attitudes and beliefs were assessed using the Dysfunctional Beliefs and Attitudes about Sleep (DBAS)-16 questionnaire. Fatigue and its effects on daily activities were assessed using the Fatigue Severity Scale (FSS). Anxiety was measured using the GAD-7 anxiety scale and depression was assessed using the PHQ-9 patient depression questionnaire.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows, version 29 (IBM), GraphPad Prism 10.4.0, JASP version 0.19.3.0. For continuous variables, normality tests were performed first. Data with a non-normal distribution (ISI) were analyzed using non-parametric tests: paired comparisons were conducted using the Wilcoxon Signed-Rank test, with data presented as median (25%, 75%). For normally distributed data (DBAS-16, FSS, GAD-7, PHQ-9), paired t-tests were used, and data are presented as mean ± standard deviation. Effect sizes were calculated following the paired comparisons, using Cohen's d or Rank-Biserial r. Fisher's exact test was used to compare proportions. A linear mixed-effects model was employed to analyze the changes in ISI over time, with assessment time point as a fixed effect and participant as a random effect. Post-hoc pairwise comparisons were conducted using Tukey's test. A p-value < 0.05 was considered statistically significant.
Results
In our previous RCT, 37 participants with an ISI >14 at baseline completed the entire study (digital CBT-I treatment and 6-month follow-up). Of these, nine participants had an ISI <8, while 28 participants had an ISI ≥8 at the end of the study. Among the 28 participants with an ISI ≥8, 11 agreed to a second round of digital CBT-I, and 9 completed it. Nine participants refused a second digital CBT-I but agreed to follow-up, and six completed it. The remaining eight participants withdrew from the study. The recruitment flowchart is shown in Figure 1.
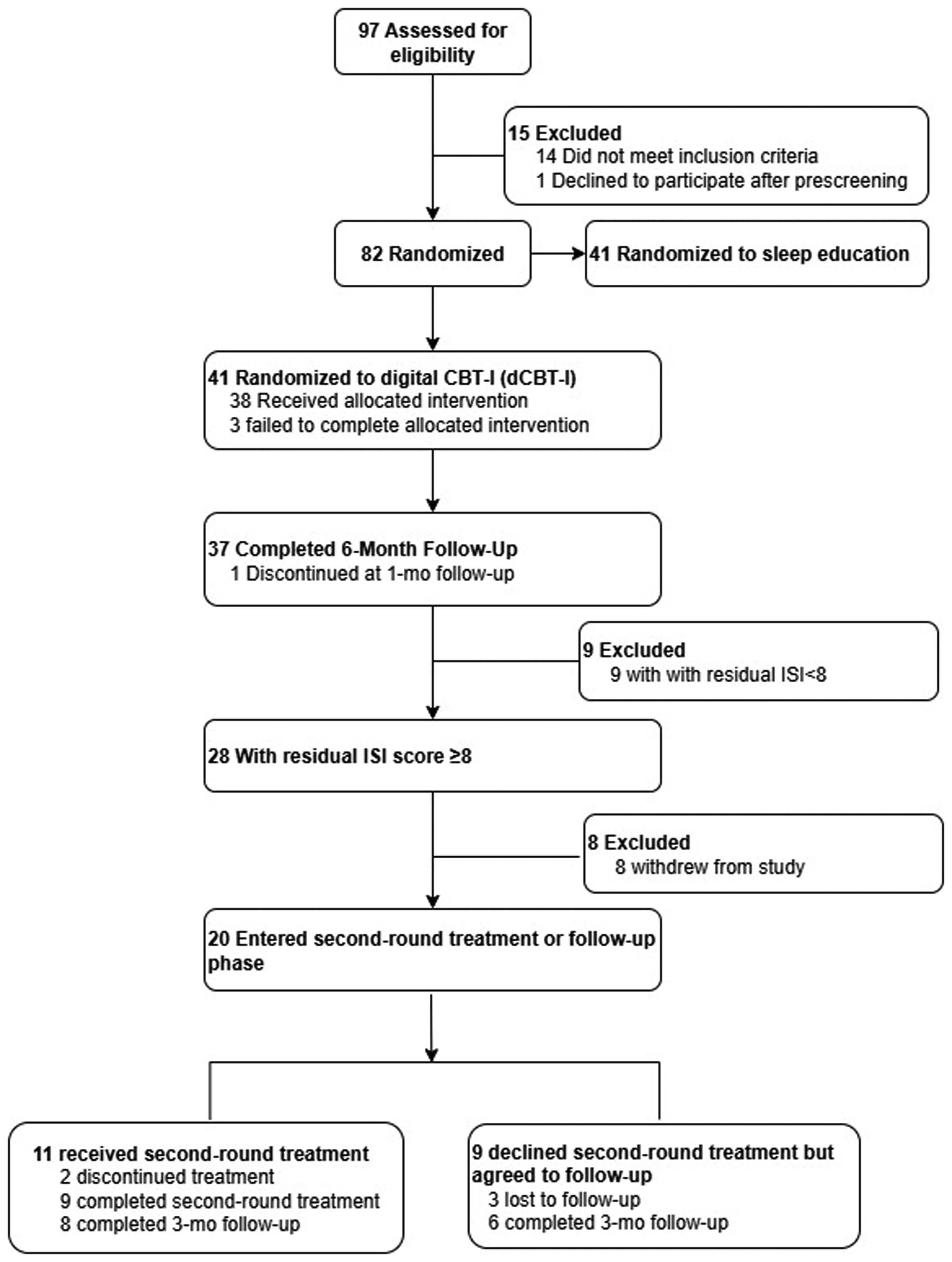
Participant recruitment flowchart.
Nine participants (5 males, 4 females, age 52.4 ± 15.5 years), all of whom had an ISI≥8, received a second round of digital CBT-I treatment.
After the second 6-week digital CBT-I intervention and at the 3-month follow-up, 44.4% and 62.5% of participants achieved ISI scores <8 (ISI remission), respectively. Fisher's exact test showed a significant difference (p = 0.0172) (Figure 2).
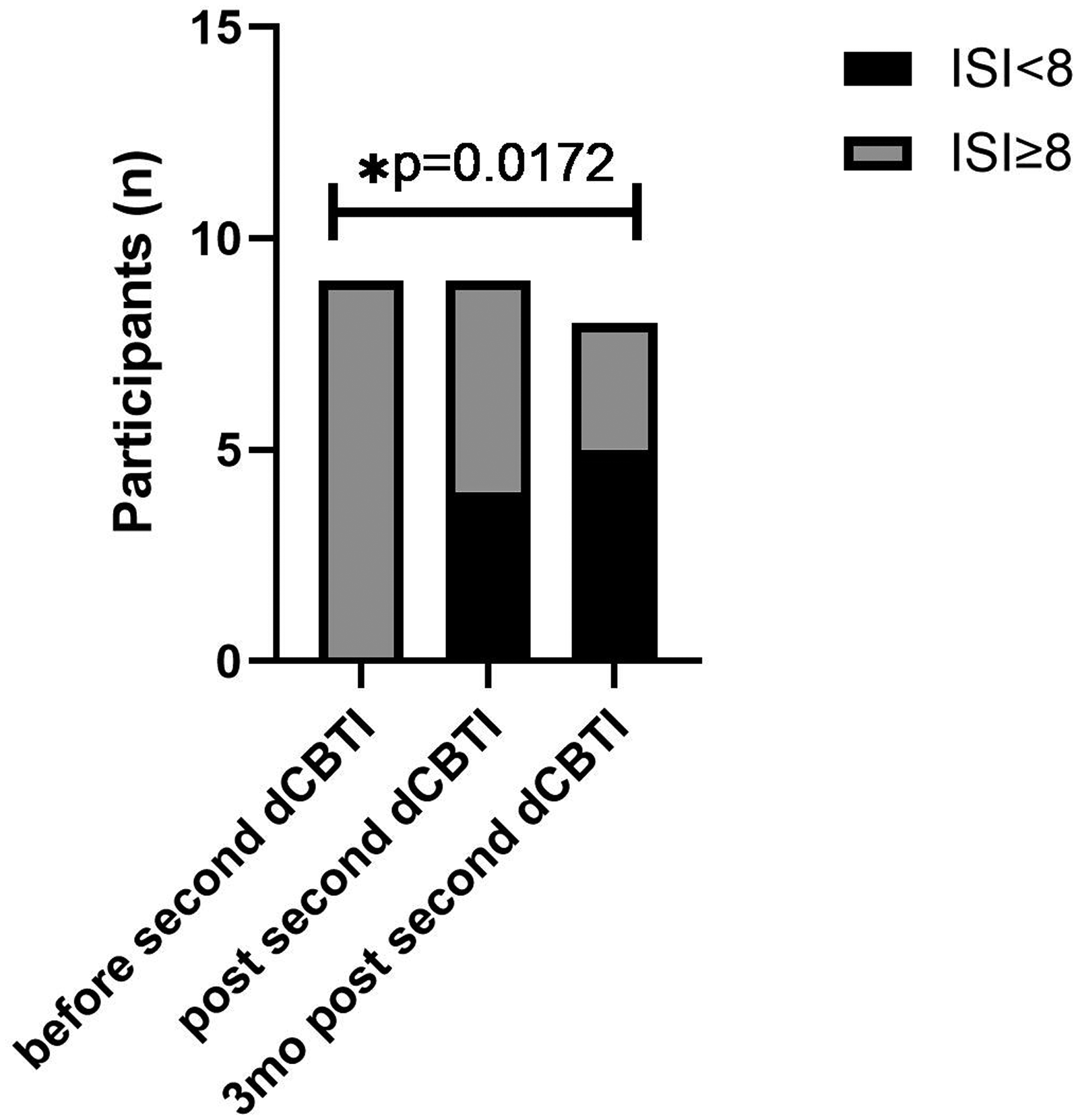
Proportion of ISI remitters from baseline to post-treatment and 3-month follow-up after the second round of dCBT-I.
A linear mixed-effects model revealed a significant main effect of treatment time point (F(3.46, 24.24) = 15.31, p < 0.0001), indicating that ISI scores changed significantly over time. Subsequent Tukey's post-hoc multiple comparisons showed that ISI scores were significantly reduced at all post-treatment time points—including after the first and second dCBT-I sessions and at follow-up—compared with baseline (all adjusted p < 0.05) (Figure 3). However, no statistically significant differences were observed between the follow-up time points themselves (all adjusted p > 0.05).

Changes in Insomnia Severity Index (ISI) scores over time.
Paired analyses using Wilcoxon rank tests confirmed that changes from baseline at each treatment and follow-up time point were associated with large effect sizes (all rank-biserial r > 0.9) (Table 1).
Changes in ISI scores following dCBT-I treatment (results of Wilcoxon rank tests).

ISI: Insomnia Severity Index; IQR: interquartile range; CI: confidence interval; r: rank-biserial correlation (JASP).
Effect size interpretation: r = 0.10 (small), 0.30 (medium), 0.50 (large). Compared to the baseline, ISI significantly decreased in both first and second dCBT-I courses with large effect size.
*p < 0.05 compared to the baseline.
Following the second treatment session, ISI scores showed a sustained further decrease, with median reductions from baseline increasing from 8 points after the first session to 12 points after the second session (Table 1). However, the difference between the two sessions did not reach statistical significance (p > 0.05).
Dysfunctional beliefs and attitudes about sleep (assessed using the DBAS-16) were significantly reduced after the second treatment compared to baseline before the second round treatment (55.78 ± 41.00 vs 80.63 ± 33.61, p = 0.0017). At the 3-month follow-up, a borderline significant reduction compared to baseline was maintained (68.13 ± 41.73 vs 80.63 ± 33.61, p = 0.050) (Table 2).
Changes in DBAS-16, FSS, GAD-7, and PHQ-9 scores following the second dCBT-I and at 3-month follow-up.
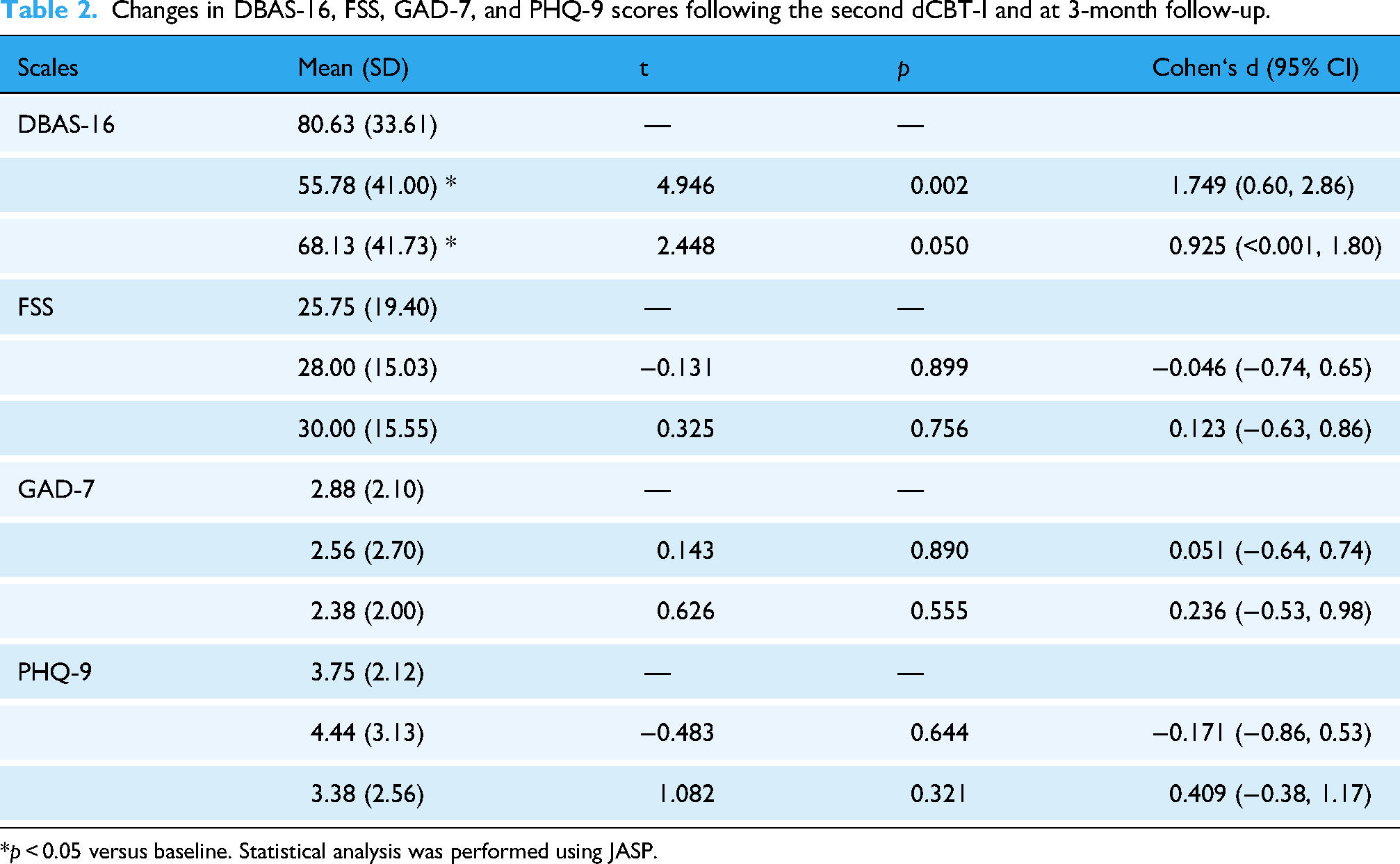
*p < 0.05 versus baseline. Statistical analysis was performed using JASP.
Compared to baseline values, no significant differences were found in other mental health scales, including the PHQ-9 for depression, GAD-7 for generalized anxiety, and FSS for fatigue severity (all p > 0.05) (Table 2).
For the follow-up without the second treatment course group, at the 3-month follow-up, all patients still had an ISI ≥8. No statistically significant difference was found compared to baseline (p > 0.05).
The decrease in ISI in the second digital CBT-I group (3.00(1.25,5.00)) was significantly greater than that in the follow-up-only group (−1.50(−3.25,0.50))(p < 0.05), using the ISI at 6 months post-first intervention as the baseline (Figure 4).

Comparison of ISI changes from baseline between the second digital CBT-I group and the follow-up-only group.
Discussion
This study showed that a second round of digital CBT-I further improves the clinical remission rate for those who showed suboptimal responses to the initial treatment. It also helps to improve dysfunctional beliefs and attitudes toward sleep. This study was based on a previous RCT assessing digital CBT-I. 3 After 6 months of the first digital CBT-I, participants with an ISI score of ≥8 were given the option of undergoing a second round of digital CBT-I. The baseline used in this study was the ISI at the end of the RCT (i.e. the ISI at the 6-month follow-up). Since the effects of CBT-I were sustained, the ISI at 6 months remained significantly lower than the pre-treatment levels. The second round of digital CBT-I tend to further reduce the ISI in patients whose scores have already significantly decreased but have not yet reached the normal range.
A key finding of this study is that approximately half of the participants who remained symptomatic after the first treatment (ISI ≥ 8) achieved clinical remission (ISI < 8) following a second round of digital CBT-I. Given the accessibility of this digital intervention, our results suggest that offering a second treatment course is a practical and effective option for alleviating insomnia severity in patients whose symptoms persist after initial intervention.
Automatic digital CBT-I is similar to traditional in-person cognitive behavioral therapy in terms of content and theory but the processes are different. In-person communication with a professional therapist ensures that the patients fully understand each step, with the therapist supervising the completion of the various therapy modules.1,11,12 However, for fully self-administered digital CBT-I,6–8 patients may encounter issues when first using the application and content, which can result in misunderstandings or deviations from the intended process, leading to suboptimal outcomes.
Although fully automated digital CBT-I is continuously improved to make it more accessible and understandable to patients—such as through the use of chatbots and virtual electronic doctors 3 —it does not guarantee the same outcomes as in-person therapy. The principle advantage of in-person CBT-I is that if a patient has queries, the therapist can explain the material from different angles and interact with the patient until they fully understand. However, the cost of the second digital CBT-I was lower, 15 making repeat digital CBT-I more feasible. Based on these findings, fully self-guided digital CBT-I may need to be repeated, which is also convenient to do.
The present study also showed that a second digital CBT-I session could further improve patients’ sleep-related beliefs and attitudes. Cognitive restructuring, a core component of CBT-I, aims to identify and modify maladaptive sleep-related beliefs and attitudes.The Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS-16) is the standard instrument for quantifying the severity of these treatment-targeted cognitions. 16 Cognitive restructuring is challenging, particularly when administered through a fully automated digital CBT-I format. Previous research has shown that the DBAS-16 can be improved through digital CBT-I.17–19 The present study showed that second round of digital CBT-I can further improve DBAS-16.
The main limitations of this study are its sample size and study design. This study was based on an RCT with a relatively small sample size of 41 participants in each group at the time of enrollment. The number of participants willing to undergo a second round of treatment further decreased, resulting in a smaller sample size. Additionally, this study is part of an extended RCT and is a preliminary exploration rather than a rigorously designed study. Regarding the timing of the second digital CBT-I, in this study, the second treatment was administered 6 months after the initial treatment, which coincides with the end of the RCT. This timing appears to be effective; however, the optimal timing for the second digital CBT-I must be determined in future studies.
A stepped care model could be considered in the future research. In such an approach, patients who do not reach clinical remission after an initial self-guided digital CBT-I course could be offered additional professional support or therapist guidance in a second step. This strategy may enhance patient engagement and potentially improve treatment outcomes compared with repeated fully automated interventions alone.
Recently rapid advances in artificial intelligence (AI) have created new opportunities in adapting and customizing digital CBT-I interventions. While existing dCBT-I platforms have demonstrated clinical efficacy and scalability, they are largely based on rule-driven and standardized treatment algorithms rather than individualized decision-making processes.3,20 In contrast, machine learning models and large language models offer the potential to support more personalized treatment trajectories.21,22 AI may enhance dCBT-I through adaptive content delivery, personalized psychoeducation, predictive risk identification, and multimodal data integration. Machine learning algorithms can dynamically adjust treatment modules based on user interaction data, while natural language processing may tailor psychoeducational content to individual concerns. AI systems may also identify users at risk of dropout or symptom deterioration and enable proactive intervention. In addition, integration of wearable-derived physiological data with self-reported outcomes may provide more comprehensive and objective feedback. Although fully integrating AI into clinical decision-making faces challenges, exploring AI-assisted personalized digital interventions is undoubtedly a promising direction to enhance the accessibility and effectiveness of digital CBT-I.
Conclusion
In conclusion, this exploratory study indicates that offering a second cycle of fully self-guided digital CBT-I to initial non-remitters may improve the clinical remission rate and ameliorate sleep-related dysfunctional beliefs. These findings suggest that a fully self-guided digital CBT-I program may offer additional benefit to a subset of patients through repeated intervention. However, given the exploratory nature of this study, characterized by a small sample size and a non-randomized design, these conclusions warrant verification in larger-scale, RCTs.
Footnotes
Acknowledgements
The authors would like to thank Mengqi Lv, Bin Gui, and Rui Su for their technical support throughout the study. The authors gratefully acknowledge Shenzhen Zeen Health Technology for providing access to the Chinese digital CBT-I platform (Resleep).
Ethical approval
This study was approved by the Human Ethics Committee of Peking University First Hospital. Written informed consent was obtained from all the participants.
Author contributions
Cheng Zhang: acquisition, analysis and interpretation of data, drafting of the manuscript, revision and submission. Yuxuan Liu: participant recruitment and data collection. Yane Shen: data collection, material support, contacting participants. Xiaoming Guo: participant referral and recruitment. Jing Ma: concept and design, obtained funding, supervision, critical revision of the manuscript for important intellectual content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Shenzhen Zeen Health Technology, which also provided the Resleep app.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of AI use in manuscript preparation
To enhance the clarity and readability of this manuscript, the authors employed ChatGPT for language editing and grammatical improvements. All AI-generated suggestions were carefully evaluated and modified as needed. The authors assume full responsibility for the accuracy and integrity of the scientific content.