
Abstract
Objectives:
Twenty-four-hour ambulatory blood pressure monitoring (ABPM) is recommended in patients with white coat hypertension (HTN) by national guideline, but was poorly utilized, and is available only in very limited subspecialty clinics. We aim to examine the feasibility and utility of ABPM in a primary care setting in the diagnosis and management of white coat HTN including the implementation and modification of antihypertensive therapy.
Methods:
Patients who have elevated blood pressure in clinic office but normal blood pressure readings at home are eligible for 24-h ambulatory BP monitoring. We analyzed data from patients who were suspected to have white coat HTN in the last 2 years underwent ABPM in our practice.
Results:
Among 68 patients, 54 patients met the selection criteria. ABPM showed that 13 patients had normal BP (24%), while 41 patients (76%) had persistent HTN. Among these patients with persistent HTN, 28 patients had intervention including 24 patients prescribed with new anti-hypertensive medication or medication increase, 3 patients prescribed with additional lifestyle modification and one started CPAP.13 patients with slightly elevated BP (133/77 for average daytime BP) didn’t have medication adjustment.
Conclusion:
ABPM has substantial utility in the diagnosis and management of white coat HTN in a primary care setting.
Keywords
Introduction
Hypertension (HTN) remains a leading cause of disability and death worldwide, and is one of the most important modifiable risk factors associated with target end-organ damage, cardiovascular disease event, and disability-adjusted life-year lost in the United States (US department of health and Human Services. Office of the surgeon general 2020). Accurate blood pressure measurement is critical in the diagnosis and management of hypertension. There is an important difference between white-coat HTN (isolated office HTN) and uncontrolled HTN. White-coat hypertension occurs in 15% to 30% of subjects with an elevated office blood pressure and is associated with minimally increased risk of CVD complications or all-cause mortality.1,2 However, uncontrolled HTN poses significant cardiovascular risk. 3 Out-of-office BP monitoring is recommended for the diagnosis of HTN according to 2021 USPSTF and 2017 ACC/AHA guideline. Ambulatory Blood Pressure Monitoring (ABPM) assessing daytime and nighttime blood pressure on a continuous basis for one 24-h period (every 30 min during daytime and every 1 h during nighttime) is generally accepted as the best out-of-office measurement method for measuring blood pressure, while Home Blood Pressure Monitoring (HBPM) assessing blood pressure at specific times during the day and night is an acceptable alternative, with only about 60% to 70% overlap with ABPM.
Twenty-four-hour ABPM consultation service can provide useful information for determining which patient has isolated office HTN and in guiding drug regimen modification for the patient. 4 A systemic review conducted by the US Preventive Services Task Force reported that ABPM provided a better method to predict long-term CVD outcome than did office BPs. 5 ABPM is approved by Medicare to verify white-coat hypertension with the diagnosis code of R30.0. Accurate assessment of white-coat hypertension is very important to avoid over medication or under treatment. ABPM led to significant number of patients with reclassification of hypertension control in older people in Spain. 6
Despite the importance of ABPM in differentiating white-coat HTN and persistent HTN, ABPM is vastly underutilized. In Unites States, Medicare claims for ABPM between 2007 and 2010 were submitted for only <1% of beneficiaries. One of the major reasons for the poor utilization is that ABPM is only available in very limited outpatient care setting within subspecialty clinic such as HTN clinic in nephrology or cardiology, while most of hypertension patients are managed in primary care setting. In order to increase its utilization, we have examined its utility in our primary care clinic. We intended to use ABPM to differentiate true white-coat HTN versus uncontrolled HTN among our patients with suspected white-coat HTN. We have collected blood pressure data from all the ABPMs performed since Jan 2020 to Jan 2022 to determine the impact of 24-h ABPM in the diagnosis and management of HTN.
Method
IRB protocol was submitted as QI project under the title “Improve blood pressure management by provide 24-h Ambulatory blood pressure monitor in patients with high risk for white coat hypertension-Quality Improvement Initiative.” Stony Brook University Human Subject Committee IRB number (No.1349978-1) was generated and deemed exempt on 9/21/2021.
Participants
After IRB approval, all patients that had ABPM in our office from Jan 2020 to Jan 2022 were identified according to the record in our office with a billing code of R30.0 that meets Medicare criteria for white-coat hypertension. Since 2001, Reimbursement of ABPM by Medicare has been limited to patients meeting the following criteria: (a) suspected white-coat hypertension defined as office blood pressure >140/90 mmHg on, at least, 3 separate clinic/office visits with 2 separate measurements made at each visit; (b) at least 2 documented blood pressure measurements taken outside the office which are <140/90 mmHg; and (c) no evidence of end-organ damage. Due to the definition change of hypertension from 2017 ACC/AHA guideline, we included patients with office BP>130/80 to reflect this update.
Data Collection
There is a total of 68 patients underwent ABPM during this period. The number was less than we initially expected due to temporary suspension of ABPM for about 6 months due to COVID-19 pandemic. We collected the following information: age, gender, office BP reading prior to ABPM, the numbers of total readings collected, the number of daytime and nighttime readings collected, white coat HTN confirmed or reclassified as persistent HTN, the decision to change medication after ABPM. Data collected was confirmed by an independent second reviewer.
In this study, we were only evaluating patients who had suspected diagnosis of white-coat HTN. This is the main diagnosis that is approved for ABPM for Medicare and most of the private insurance. If BPs were <130/80 in office prior to ABPM, then these patients did not meet criteria for suspected white coat HTN, thus would be excluded. Selected patients need to meet the following criteria: (1). The office BP reading prior to ABPM needs to be >130/80. (2). Patients selected need to have minimum of 70% of successful programed measurements, corresponding to a minimum of 20 daytime readings and 7 nighttime readings. 7 If the number of measurements obtained is slightly fewer than this, it may still be reasonable to accept the ABPM study as valid, understanding that the results are not optimal; thus, we included patients with nighttime reading of 6. The ABPM result is reviewed by the ordering physician who documents the result of ABPM and decision for medication adjustment.
Data Analysis
HTN is defined as following with ABPM with the diagnostic criteria suggested by the 2017 ACC/AHA guidelines; meeting one or more of these criteria using ABPM qualifies as confirmation of hypertension: (1). A 24-h mean of ≥125 mmHg systolic or ≥75 mmHg diastolic; (2). daytime (awake) means of BP ≥ 130 mmHg systolic or ≥80 mmHg diastolic; (3). nighttime (asleep) means of BP ≥ 110 mmHg systolic or ≥65 mmHg diastolic
We used ABPM 7100 monitor manufactured by Welch Allyn. Software CardioPerfect Workstation version 1.6.6 (or higher) was provided with the monitor and installed on a designated computer by IT personnel from Stony Brook university hospital to ensure proper installation and security that meets standard for medical record storage. Access was same as accessing medical records in Stony Brook University hospital. For any technical questions, we would call technical support from WelchAllyn for software problems.
For ABPM, nighttime or daytime readings and 24-h readings were used successfully.8-10 We chose daytime readings and 24-h readings instead of nighttime readings for the diagnosis of HTN. For practical reasons, home readings correlate more closely with the results of daytime ambulatory measurements than with blood pressures that are typically obtained in the clinician’s office. Daytimes readings are collected from 8:00 am to 10:00 pm. Nighttime readings are collected from 10:00 pm to 8:00 am. We set specific time instead of individualized schedule for the sake of simplicity.
Results
Patient Characteristics and the Overall Result of ABPM
Of the 68 patients underwent ABPM, 3 patients didn’t have complete data, 6 didn’t meet criteria for data collection, 5 patients didn’t meet criteria for white-coat hypertension since office BP prior to ABPM was normal. Fifty-four patients that met all the criteria mentioned in the method were selected (Figure 1).
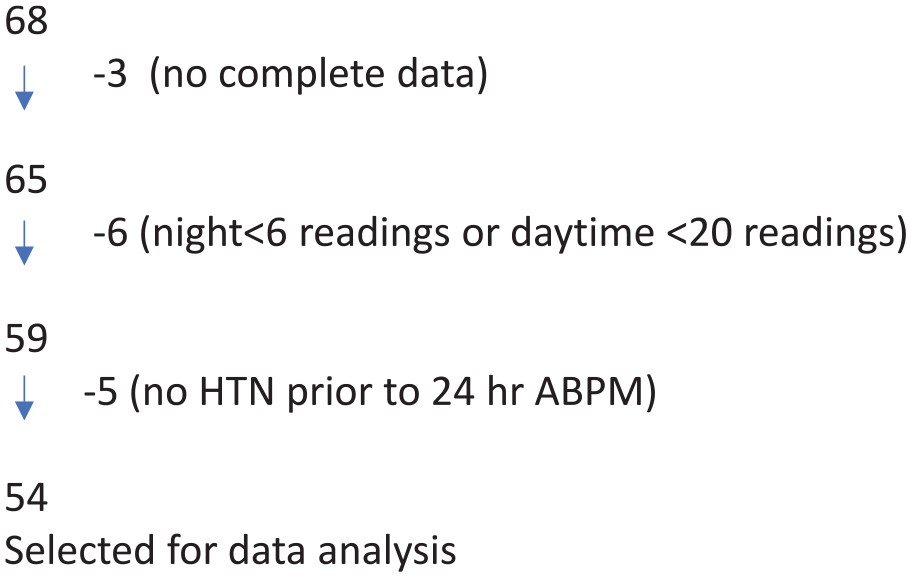
Patient selection.
Baseline patient information is summarized in Table 1. It was a group of patients with mean age of 65 years, and the majority were females 38/54 (70%) and less than a third were males 16/54 (30%). Mean office BP readings prior to 24-h ABPM was 153/81. Twenty-four-hour ABPM average BP is 133/79 mmHg, daytime BP average is 135/80 and nighttime BP average of 119/63.
Baseline Patient Information.

As shown in Figure 2, out of 54 patients, 13 of them (24%) was confirmed as white-coat HTN (or white coat effect). Forty-one of the 54 patients (76%) was reclassified as persistent HTN. Among 41 patients that were confirmed as persistent hypertension, 13 patients with slight elevation of BP didn’t have documented intervention. Twenty-eight patients with significant BP elevation had documented intervention either with lifestyle modification or medication increase.

Reclassification of diagnosis after ABPM.
Confirmed White-coat Hypertension
Among the 13 Patients with confirmed white coat HTN, 4 patients were male and 9 patients were female. This was relatively proportional to male: female patient ratio in the selected population (16:38). Patients with white-coat HTN had an average age of 68.
BP in this group has average 24-h BP of 118/68, daytime BP of 119/67 and nighttime of BP of 115/66 (see Table 1). Thus, white coat hypertension is confirmed and continue existing management. No new intervention was applied. This reclassification prevented unnecessary medication in 13 out of 54 patients (24%), and avoided potential antihypertensive medication side effects.
Confirmed Persistent HTN
The group of patients with persistent HTN had average age of 64. Among the 41 reclassified patients, 13 of them didn’t have any documented intervention (Figure 2). As shown in Table 1, the average daytime BP of the group diagnosed with persistent HTN without intervention was about 133/77 and 24-h BP reading of 131/77. Lifestyle modification was discussed with these patients. The remaining 28 patients had documented intervention. The group of patients had average daytime BP for patients who had intervention was 144/87, 24-h BP was 141/85 and nighttime reading of 133/78. New medication prescribed or existing medication dose increased in 24 out of 28 patients. One patient started CPAP machine for obstructive sleep apnea, and 3 had implementation of lifestyle modification.
Discussion
Very few studies described the role of ABPM in the diagnosis and management of white-coat HTN in primary care setting. A MEDLINE search using the keywords “ambulatory blood pressure monitoring” and “white-coat hypertension” until January 2022 did not yield any significant published studies. Our result using ABPM intended to diagnose white-coat HTN in an academic primary care setting has demonstrated for the first time that the majority of patients actually had persistent HTN and needed additional intervention to control blood pressure for the prevention of cardiovascular events.
Our result is consistent with a study for the use of ABPM for hypertension management in community pharmacy described by Gardner and Schneider. 4 In that project, pharmacists helped to educate patients that were referred by their PMD with HTN medication education and performed 24-h ABPM. Based on ABPM result, pharmacists made a recommendation of BP medication changes to referring doctor. Unnecessary therapy was avoided in 40% of patients with suspected isolated office HTN. This is consistent with the data we have in primary care setting ordered and interpreted by patients’ own PMD without referral, with 24% avoid unnecessary medication treatment and another 24% can be monitored closely without immediate medication addition. In addition to avoid unnecessary medication, the ABPM likely prevented overmedication induced adverse effect such as injuries related to relative hypotension, such as falls which is the leading cause of injury death for people over 65 from CDC record.
Our result strongly supported the use of 24-h ABPM in a primary care setting for suspected white-coat HTN. The use of 24-h ABPM in the setting may greatly help to improve the severe problem of underutilization. Even though ABPM is considered as the gold standard for diagnosing HTN and reimbursed by Medicare for suspected white-coat hypertension, actual reimburse claim for Medicare is less than 1% of beneficiary. In addition, favorable patient acceptance of ABPM was found in a primary care setting in the United States. 11
There are several reasons for the underutilization of ABPM in outpatient care setting, particularly in primary care clinics. Firstly, the ABPM machine with software is costly, normally runs more than $2500. The reimbursement is low, about $64.7 from Medicare with both test and interpretation. Private insurance potentially pays slightly more ranging $55.00 to 220.00. Thus, for a small practice with limited patients, not only it doesn’t provide financial incentive, but also can become a financial burden and add more stress to the already resource limited primary care. In order to provide more access for patients who need this service, ABPM from centralized service or pharmacy might be helpful to provide this service if patient has a prescription from their primary care physician. This was demonstrated to be feasible and useful. 4 Secondly, we noticed that insurance coverage varies, and patient copay is different and quite unpredictable. We needed to find a way for obtaining insurance coverage information and prior authorization to ensure smooth coverage for patients. Thirdly, there is a general need of education for ABPM use and significant number of health care providers are not familiar with the use of ABPM and interpretation. More education will help to expand the use of ABPM.
Despite the difficulty to have access of ABPM in the community, we have tried to expand the utilization of this useful tool to help better diagnosis and management of HTN and improve quality. Our practice data supported the notion that ABPM is feasible in outpatient setting. We have 2 nurses who are in charge of ABPM. Physicians will send a message to the nurses in charge of ABPM regarding the need to perform ABPM with a timeline and document in the chart regarding the rational for performing ABPM (Medicare requires this and other insurance might require that information too to get it covered). The nurse in charge will schedule the patient. Normally we schedule up to 3 ABPM a week though theoretically we can schedule more than 5 a week. However, patient might be late returning the machine. When we put the ABPM on a patient, we provided the patient with information sheet for education and quick trouble shooting. Our primary care clinic has about 26 attending physicians, 3 NPs and residents who work with 3 to 4 attending physicians at any given time. The charge nurse normally trains at least 2 nurses that knows how to operate the ABPM. We have been able to obtain the data reliably using the ABPM. It provided community with example that it is feasible to provide this service in primary care setting, especially in a large group with a lot of patients. Recently, we had more patients needing 24-h ABPM than one ABPM machine can handle, and just got approved for purchasing a second monitor.
Our study has several limitations. Firstly, it is a small study with a total of 68 patients. Secondly, we used fixed time 10:00 pm to 8:00 am as nighttime reading instead of the true nighttime. We initially tried to identify true time of sleep and wake by patient pushing on- and off-buttons. However, it caused significant problem for BP recording of some patients. This problem was minimized by using 24-h BP and daytime BP for white-coat HTN diagnosis. Finally, we were not able to assess the true impact of BP medication. We likely included patients who were already on BP medication, with well-controlled BP at home and elevated blood pressure in office. We were unable to identify reliably when it was started. However, our results showed that the BP for patients who are reclassified as persistent HTN but didn’t have specified intervention was relatively close to normal BP though elevated, and lifestyle modification was discussed with these patients. Patients who had BP management intervention clearly had higher BP (Table 2).
BP Difference Between Groups: White Coat HTN, Persistent HTN With Intervention and Persistent HTN Without Intervention.

Conclusion
The overall utility of 24-h ABPM is evident to improve the quality of BP management for patients with white-coat hypertension. This information is important in providing more accurate classification of HTN diagnosis and avoiding overtreatment and undertreatment of HTN, both have significant clinical consequence. Our ABPM data demonstrated using ABPM is clinically helpful for improving patient care, and it is feasible in a primary care setting. Further studies with a large patient population with white-coat HTN in a primary care setting are needed to expand the use of ABPM for the better diagnosis and control of hypertension.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Stony Brook University Human Subject Committee (IRB) (No. 1349978-1) deemed exempt 9/21/2021.