
Abstract
Background:
Non-communicable diseases and psychiatric pathologies are the health problems that most affect the population in the United States.
Objective:
This study aimed to examine the mediating role of patient-centered communication (PCC) in the relationship between satisfaction with medical care, physical health, and emotional well-being in American men.
Methods:
A cross-sectional - predictive study was carried out. The variables analyzed were satisfaction with medical care, physical health, and emotional well-being. Information from the Health Information National Trends Survey Data (HINTS) was used; HINTS 5, cycle 3 (collected between January and June 2019) and 4 (2020). Data from 3338 men were considered (mean age: M = 55.40, SD = 19.53). Data analyses were carried out using structural equation modeling (SEM) to represent the statistical mediation model with latent and observable variables.
Results:
Analyses showed that the variables were significantly related (P < .01). In the mediation model, there is evidence that satisfaction predicts communication (β = .764, P < .001) and this, in turn, is related to physical health (β = .079, P = .007) and emotional well-being (β = .145, P < .001). In addition, the standardized estimates of the structural multiple mediation model presented acceptable goodness-of-fit indices: χ2/gl = 2.24, CFI = 0.999, TLI = 0.999, RMSEA = 0.019 [90% CI: 0.013-0.022], SRMR = 0.018.
Conclusion:
Patient-centered communication plays a significant dual mediating role in the relationship between satisfaction with medical care, physical health, and emotional well-being, respectively. Therefore, PCC is essential in healthcare for American men.
Introduction
In the United States, noncommunicable diseases are among the main public health problems, causing 89% of all deaths annually. 1 Noncommunicable conditions, such as heart disease, different types of cancer, stroke, diabetes, and chronic obstructive pulmonary disease, are responsible for more than two-thirds of all deaths. 2 On the other hand, mental illness is also one of the main causes of mortality in the world, causing a total of approximately 8 million deaths each year.3,4 They are considered one of the main causes of disability and one of the most important risk factors for non-communicable diseases. 5 In fact, people with mental illnesses such as anxiety and depression are more likely to have obesity and other chronic physical conditions such as diabetes and cardiovascular disease with a risk 1.4 to 2.0 times higher than in the general population. 6
Some studies report that men have a higher prevalence of these pathologies, which drastically impacts their life expectancy in the United States. 7 In fact, they live fewer healthy years than their female counterparts.8,9 In addition, men have a higher probability of mortality from noncommunicable diseases at younger ages than women. 10 This could be explained by men’s reluctance to use health care services 8 and, secondly, the fact that men tend to adopt unhealthy behaviors that affect the prevention and treatment of diseases. 11 This is reflected in poor eating habits, including low consumption of fruits and vegetables and increased consumption of saturated fats12,13; in addition to other modifiable risk factors, such as sedentary lifestyle, tobacco, and alcohol consumption.5,13,14 Public awareness of the essential role of a gender perspective in men’s physical health and emotional well-being is needed as physical and emotional illnesses continue to increase. 15
On the other hand, male patient-centered communication can have a positive impact on physical health and emotional well-being. 16 The quality of patient-centered communication is a key determinant of patient satisfaction with medical care. In turn, satisfaction with health care service can positively impact emotional health, which also improves physical health. 17 In fact, studies have explored the role of communication in improving treatment efficiency from the perspective of patient satisfaction with medical care. 18 There is evidence of the positive effects of communication in patients with chronic physical conditions, such as hypertension, obesity, and diabetes, and mental illnesses, such as depression and schizophrenia. 19 There are several factors that influence people’s physical and mental health5,13,14; however, there is a growing body of scientific evidence suggesting that satisfaction with quality of care derived from effective patient-provider communication may positively influence these conditions.20 -22 Effective doctor-patient communication can promote effective information exchange, which is beneficial for patients to obtain health information, make appropriate decisions, and ultimately achieve positive health recovery outcomes. 22
However, it is important to mention that communication between physicians and male patients represents a challenge for the medical community. 23 In medical encounters, male patients ask fewer questions, obtain less information, receive less counseling and preventive services, and their visits are less participatory than female patients.23,24 In addition, men, in general, tend not to inform their physicians about the presence of any disease. 25 Untreated health problems in male patients can become a concern because they are much less likely to seek physical and mental health treatment. 26 One study showed that patients who did not show a greater tendency to discuss lifestyle and psychosocial concerns with their physicians were those who did not experience early recovery from their physical pain. 20 Therefore, it is important for physicians to seek effective communications strategies with male patients to improve the physician-patient relationship, their satisfaction with the quality of medical care, and avoid negative impacts on physical and mental health outcomes.
Communication problems between male physicians and male patients have received little attention. There is a need to explore physician-patient communication and male patients’ satisfaction with quality of care to improve the efficiency of treatment of physical and mental conditions. Therefore, we hypothesized that male patient-centered communication may play a mediating role in the relationship between quality of medical care, mental health, and physical health in Americans.
Materials and Methods
Data Sources and Participants
A cross-sectional-predictive study was carried out. 25 This is a secondary analysis of the Health Information National Trends Survey Data (HINTS). The data were collected by the National Cancer Institute (NCI) and are part of HINTS 5, cycle 3 (collected between January and June 2019) and 4 (2020). It is a nationwide survey of the noninstitutionalized US adult population for collecting information on health-related behaviors, knowledge, and attitudes. 26 The sampling design for HINTS has been previously and extensively described.14,26 Participants who provided information on physical health problems and emotional well-being were included.
We considered those adult male respondents who answered the questions on the study variables (N = 3338, mean age = 55.40, SD = 19.53). The data exceeded the minimum required sample size (518) for SEM statistical mediation models 27 considering the number of observable and latent variables, statistical power, and the minimum anticipated effect, which have been used in previous research. 28
Variable Measurements
Patient-centered communication (PCC): A latent variable was developed considering respondents’ communication with doctors, nurses, or other health professionals in the last 12 months. Seven questions were asked, which are as follows: “How often did they help you deal with feelings of uncertainty about your health or healthcare?” (PC1); “How often did they spend enough time with you?” (PC2); “How often did they explain things in a way you could understand?” (PC3); “How often did they make sure you understood the things you needed to do to take care of your health?” (PC4); “How often did they involve you in decisions about your healthcare as much as you wanted?” (PC5); “How often did they give the attention you needed to your feelings and emotions?” (PC6); and “How often did they give you the chance to ask all the health-related questions you had?” (PC7). 29 These indicators make up the main dimensions of PCC: meeting informational needs (PC3 and PC4), meeting emotional needs (PC1 and PC6), and involving enough twoway interaction and shared decision-making (PC2, PC5, and PC7).29,30 The response options to the 7 questions were categorized considering a 4-point scale: 4 = always, 3 = usually, 2 = sometimes, and 1 = never). 29 The items were reverse-scored prior to analysis and summed to create a continuous overall score for PCC, where higher scores indicate higher levels of PCC (see Supplemental Table S1).29,31
Satisfaction with medical care: This variable was assessed by an item measuring perceived quality of care, which was used as an indicator of patient satisfaction. Respondents were asked: Overall, how would you rate the quality of health care you received in the past 12 months? Responses were rated on a 5-point Likert scale (1 = poor and 5 = excellent). This measure has been used in previous articles evaluating HINTS data (see Supplemental Table S1). 32
Physical health: Respondents provided information on their physical health, including perceived health status, body mass index (BMI), calculated using weight and height, and number of chronic conditions, which together were included for the creation of this latent variable in the structural equation model. 33 The Quetelet formula was used to calculate BMI by dividing weight (measured in kilograms) by the square of height (measured in meters) (see Supplemental Table S1).
To determine the number of chronic conditions, respondents indicated yes or no when answering the question: “Has a doctor or other health professional ever told you that you had the following conditions: diabetes or high blood sugar, hypertension or high blood pressure, a heart condition, chronic lung disease, arthritis or rheumatism?” Responses were summed, with higher scores indicating a greater number of chronic conditions. Finally, respondents were asked to rate their perceived general health with response options (1) excellent, (2) very good, (3) good, (4) fair, and (5) poor. This proposed variable has been used in previous HINTS studies from 2014, 2017, and 2020 (see Supplemental Table S1).14,31
Emotional well-being: This variable was assessed using the Patient Health Questionnaire for Depression and Anxiety (PHQ-4), which combines 2 short 2-item questionnaires for depression and anxiety (see Supplemental Table S2). 34 Respondents were asked how often they were bothered by the following problems in the last 2 weeks: (1) little interest or pleasure in doing things (EW1); (2) feeling down, depressed, or hopeless (EW2); (3) feeling nervous, anxious, or on the edge (EW3); and (4) not being able to stop or control worry (EW4). Responses were rated on a 4-point Likert scale (1 = almost every day to 4 = not at all) and summed to calculate total emotional well-being scores, ranging from 0 to 16, as reported in previous research.32,35
Sociodemographic data: Sociodemographic variables in the study included age, education level (basic, incomplete university, complete university, and postgraduate), employment (yes or no), income range ($0-$19 999, $20 000-$49 999, $50 000-$99 999, and $100 000 or more), and race (white, black or African American, Hispanic, Asian, and other).
Statistical Analysis
Descriptive statistics of the study variables and internal consistency values were performed. Structural equation modeling was used to represent the direct and indirect effects of the proposed statistical mediation model, taking into account the non-normality of the multivariate data and the use of Likert scale items, so the ULS estimation was considered 36 recommended for SEM multiple mediation models with secondary data on a national scale. 37
Mediating models consider a third variable that intervenes in the relationship between the independent and dependent variable (direct effect). This mediating variable allows another causal route (indirect) that goes from the independent variable to the mediator and from the mediator to the dependent variable. 25
Mediation models that report significant direct and indirect effects are partial, while if the direct effect is reduced to a non-significant effect, it means that the model presents a total mediation in the relationship of the variables. The overall fit was considered based on several indices such as root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker-Lewis index (TLI), and standardized root mean square residual (SRMR), 38 which have been used to evaluate multiple mediation models, that is, simultaneous statistical mediation models represented in a structural equation model.39,40
Likewise, the chi-square test and the degrees of freedom [χ2/gl] were used, considering a good fit to estimated values below or equal to 4; these aspects were considered in previous studies that included HINTS data. 14 The respective statistical analyses were performed using the open access statistical program JAMOVI (version 1.8.4).
Results
Of the total number of respondents (N = 3338), 53.3% lived as a couple, with a mean age of 55.40 ± 19.53, and the highest proportion had a basic education (33.5%). In addition, more than half (67%) reported that they were employed, while 61.6% were white (Table 1).
Number and Percentages of Participants According to Their Socio-Demographic Characteristics.

Standardized estimates of the structural multiple mediation model presented acceptable goodness-of-fit indices for the data: χ2/gl = 2.24, CFI = 0.999, TLI = 0.999, RMSEA = 0.019 [90% CI: 0.013-0.022], SRMR = 0.018. First, we reported significant total effects (excluding the mediator variable) of satisfaction with medical care on physical health (β = .083) and emotional health (β = .114). Subsequently, when the mediator variable was included, the total effects were decomposed into direct and indirect effects. The structural model (Figure 1) shows that satisfaction with medical care significantly predicted patient-centered communication (β = .764, P < .001). The same was observed between patient-centered communication in relation to physical health (β = .079, P = .007) and emotional mental well-being (β = .145, P < .001). While the direct effects were smaller than the indirect regressions and practically non-significant, specifically in the association of satisfaction with medical care with physical health (β = .022, P = .436) and emotional well-being (β = .003, P = .939). This refers to total mediation effects, 41 where indirect effects account for a 71% proportion of the overall effect size on physical health (β = .061, P < .001) and 98% on emotional well-being (β = .111, P < .001). The values of the standardized regressions showed 1 large, 1 medium, and 1 small indirect effect size, 40 where the mediator variable had an explained variance of 0.576 considering a moderate effect size (0.25 ≥ R 2 ≥ 64) 42 which is above the minimum recommended value of practical significance in clinical research.

SEM mediation analysis.
Table 2 presents the descriptive data. As a previous step of the statistical mediation proposal, it was taken into account to determine the relationship between the study variables, which are significantly associated.
Descriptive Data and Relationship of the Study Variables.
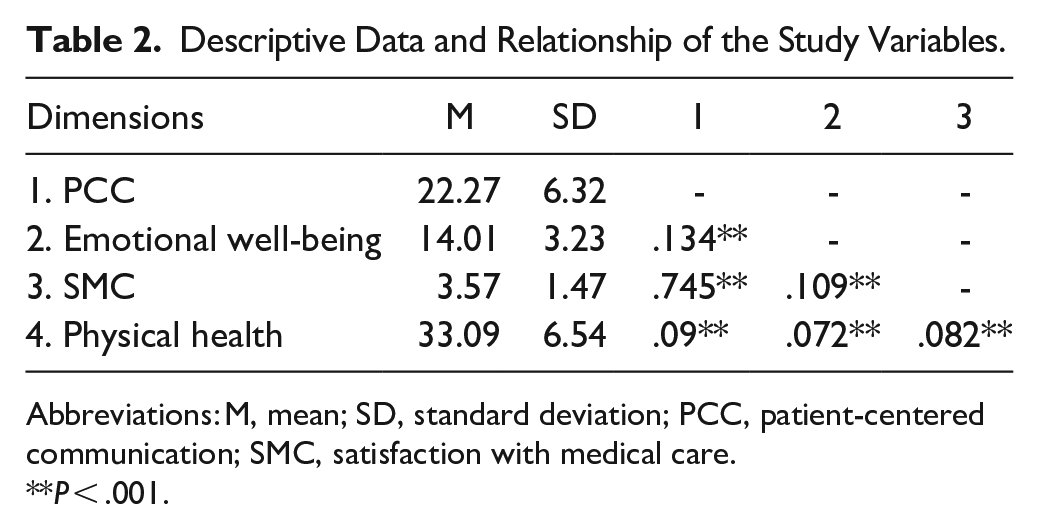
Abbreviations: M, mean; SD, standard deviation; PCC, patient-centered communication; SMC, satisfaction with medical care.
P < .001.
Discussion
Chronic noncommunicable diseases and mental illnesses are the health problems that most affect the population in the United States.1,3,4 Beyond the implications for people’s own physical and emotional well-being, 6 these pathologies increase the overall burden of disability. 43 Since understanding these diseases is essential for conducting appropriate health promotion and prevention programs, the objective of this study was to test whether patient-centered communication mediated the relationship between satisfaction with medical care, physical health, and emotional well-being in adult American men. Patient-centered communication was found to be a significant mediator in the relationship between satisfaction with medical care and physical health. Likewise, we found that communication played a significant mediating role on the relationship of satisfaction with medical care and emotional well-being.
Patient-expressed satisfaction with medical care is the state of pleasure or happiness that patients experience when using a health service. 44 Previous studies have shown associations between satisfaction with medical care and health status. 45 Satisfaction with health services is considered a determinant of health status, 46 and can impact the perceived physical condition of individuals. 45 In the current study, we found that satisfaction with medical care is associated with physical health. Several studies have examined the relationship between the care received and health outcomes and mortality. Recovery, restoration of function, and survival of patients are indicators of the quality of medical care. 47 One study reported that some factors such as hospital service, type of professional, and hospital are related to the incidence of perinatal mortality. 48 The quality of medical care is reflected in surgical case fatality rates. 49 It is worth mentioning that some processes of medical care, such as the reorganization of the outpatient clinic, 50 intensive hospital care, 51 and home care, 52 impact patients’ health status, recovery, and survival, respectively. Healthcare facilities should provide effective, efficient, and coordinated care for patients with chronic conditions. This should be done considering that gaps or poor quality of medical care can negatively impact the prevention and control of these diseases. 53
Apart from physical health status, emotional well-being is one of the factors associated with satisfaction with medical care. 54 Satisfaction with medical care, defined as an overall psychological state, includes cognitive and emotional components that impact the desired emotional well-being outcome. 55 Patient satisfaction with care can lead to better mental health outcomes through behavioral changes and improved adherence to treatment. 56 In our study, a significant relationship between satisfaction with medical care and emotional well-being was evidenced. High satisfaction with quality and timely access to appropriate medical care can minimize the impact of poor mental health. One study reported that some mental health problems, such as high psychological distress, anxiety disorders, and poorer cognitive functioning were associated with low satisfaction with medical care. 54 Another study identified that those diagnosed with schizophrenia, post-traumatic stress disorder, depression, and other psychiatric disorders had significantly lower satisfaction with primary care services compared to those without these disorders. 57 These associations could be due to ineffective interpersonal communication between providers and patients with emotional health problems. The results of these studies highlight the need for better medical care for patients with mental health problems.
Effective and efficient patient-physician communication is the art of medicine and lies at the heart of healthcare and patient satisfaction with medical care. 58 Studies have explored how appropriate communication can improve treatment efficiency from the perspective of patient satisfaction with medical care. 18 In our study, we conducted a mediation analysis and found that patient-centered communication had a greater indirect effect on the relationship between participants’ satisfaction with medical care, physical health, and emotional well-being. Patient-centered communication can improve the patient-physician relationship, 59 the quality of medical care, 60 and supports a number of clinical outcome indicators such as adherence to treatment. 61
In fact, communication is a fundamental aspect in the quality of health care delivery and patient satisfaction with medical care, and is considered an essential component in the treatment and recovery of patients.18,19,59 Good doctor-patient communication is one of the preferred attributes of patients. There is a need to strengthen the communication skills of health professionals, particularly physicians, dietitians, and nurses. This can be achieved through effective, culturally adaptable, and competent training, followed by rigorous evaluation. This is particularly important to achieve good results in the physical and emotional health of patients. Communication should be part of care to improve the overall health and well-being of patients.
Gender is an important factor in the occurrence of noncommunicable diseases and psychiatric disorders. Men have a higher probability of mortality from noncommunicable diseases at younger ages compared to women. 10 In addition, a silent crisis in men’s mental health is reported. 62 In men, mental health problems become a concern because they are not easily treated, because men are much less likely to seek mental health treatment compared to women. 63 Previous research has reported that satisfaction scores with medical care often differ with respect to gender. 64 One study identified that men tend to be more satisfied with the care they receive. 65 Satisfaction with medical care is essential for better physical health and emotional well-being; which, in turn, depends on better management of noncommunicable and psychiatric diseases through appropriate care. The existence of a male-centered health system and better attention to issues related to men’s overall well-being can positively impact the higher mortality rates observed in men compared to women. 8
Limitations and Strengths
The findings of this study should be interpreted considering certain limitations. First, the data were collected through self-report; therefore, the results are subject to recall bias, overreporting, and desirability bias. Secondly, this is a cross-sectional study, therefore direct causality cannot be inferred. Constructs such as patient-centered communication and satisfaction with medical care were not assessed using structured instruments; however, the use of national respondent data generally has these limitations. 66 Finally, confounding by unmeasured variables is a common limitation in observational research. Despite these limitations, we consider that the study presents some strengths such as the use of SEM procedures to test mediation. This statistical analysis technique, unlike a traditional regression, makes possible the simultaneous evaluation of observed and latent variables, considering a better adjustment of the measurement error, and the representation of a structural model including direct and indirect effects. 67 It is a prospective cohort study with a large, nationally representative, and ethnically diverse sample size.
Conclusions
This study demonstrates that patient-centered communication plays a significant dual mediating role in the relationship between satisfaction with medical care, physical health, and emotional well-being, respectively. Patient-centered communication can play a pivotal role in healthcare for American men. Future studies should continue to evaluate other clinical concepts that affect men’s physical health and emotional well-being over time.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221114850 – Supplemental material for Relationship Between Satisfaction With Medical Care, Physical Health, and Emotional Well-Being in Adult Men: Mediating Role of Communication
Supplemental material, sj-docx-1-jpc-10.1177_21501319221114850 for Relationship Between Satisfaction With Medical Care, Physical Health, and Emotional Well-Being in Adult Men: Mediating Role of Communication by Cristian Ramos-Vera, Jacksaint Saintila, Yaquelin E. Calizaya-Milla, María Elena Acosta Enríquez and Antonio Serpa Barrientos in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.