
Abstract
Black women living in Prince George’s (PG) County, Maryland, have high rates of overweight and obesity. Obesity significantly impacts Black women, leading to poor physical and mental health, decreased social well-being, and a financial strain on the healthcare system. Despite living in an affluent area and having middle to high incomes and high education levels, Black women living in PG County have difficulty managing their weight. This study explores how social and cultural factors and social networks impact the weight of Black women living in PG County, Maryland. A qualitative case study design guided by social cognitive theory was employed to conduct semi-structured interviews and focus groups with 15 women. Key social and cultural factors (income, family network, peer network, and living in PG County) influenced participants’ attitudes and behaviors toward their weight and strategies to manage their weight. Additionally, participants expressed that Black culture is more accepting of larger and curvier body types, and this reinforces a positive body image and less desire to achieve an ideal BMI. Participants also expressed that COVID-19 impacted their weight management strategies. This study adds to the literature by better explaining some of the underlying factors that influence decision-making around weight management among Black women who live in PG County, Maryland.
Introduction
Overweight and obesity (OVO) is a major public health concern, especially among Black women. Obesity is caused by factors that are modifiable (engaging in physical activity and eating a healthy diet) and non-modifiable (genetics, developmental conditions, or metabolism). Social determinants of health (SDOHs), the health, economic, and social conditions where people live, work, play, and worship, influence one’s ability to make healthy decisions. About 80% of poor health outcomes are due to SDOHs and psychosocial factors, therefore medical care alone cannot improve health outcomes. Prevention and treatment efforts need to be focused on solving the underlying issues leading to overweight and obesity (OVO). Left unchecked, OVO can lead to a myriad of chronic health conditions, such as hypertension, diabetes, high cholesterol, and the worsening of mental health issues, leading to poorer quality of life and put an undue financial strain on the healthcare system.1 -5 People living with OVO also often experience stigma, social isolation, and discrimination.
Achieving and/or maintaining a healthy weight is complicated by external social and cultural factors like social networks and family upbringing. Social and cultural factors like stigma, bias, racism, body perception, cultural food practices, social influencers, stress, and religion are key factors in weight-based decision making. One theory to help explain this is the Social Cognitive Theory which describes how individual experiences, external environment, and other’s actions can influence one’s decision making ability with regards to their health. To effectively elicit positive changes in health behavior, one must receive social support, build their self-efficacy to manage their disease/condition, and use observational learning. The Social Cognitive Theory is one of most widely used theoretical frameworks to address chronic disease management, including obesity.
One’s culture can be influential in forming personal viewpoints on health and wellness and different cultures have varying views and approaches to eating and physical activity habits, 6 which are influenced by their traditions and history. For example, the spirit of collectiveness and the central role of family and friends are prevalent core values in Black culture. People within similar social networks model their eating and activity habits after each other. These external factors can help explain how Black women make health decisions and how they perceive and handle external triggers. Some research suggests that obesity may be contagious, suggesting that if a close relative or friend (eg, sibling or spouse) is living with OVO, then their partner will be too. 7
Another issue is the historical abuse leading to generational oppression. Black people have been historically disenfranchised and negatively impacted by economic policies and health disparities. For example, Black people are less likely to have the ability to walk to the grocery store and have longer commute times to get groceries because of lack of access to stores in their neighborhood. For Black people, safety and access to public transportation are key in choosing a grocery store, whereas this is not as much of an issue for their white counterparts, for example. 8
One area of interest is Prince George’s (PG) County, Maryland (located outside of the nation’s capital). PG County is one of the most affluent Black suburbs in America; 60% of residents are Black, and over half of those are Black women, with the median age being 36.7 years. Of the Black women living in PG County, 46.3% earn more than $75 000 per year (median $79 184), which is higher than the national average (2018 data), 67.6% own their own home, 38.8% have a bachelor’s degree or higher, and 28.1% have at least some college or trade school.9,10 Despite the county’s affluence, residents report a lack of access to nutritious and quality foods, culturally appropriate foods, and grocery stores, with many living in designated food deserts. Over 25% of the restaurants are “carry-outs” 11 which serve low-nutritional value and high calorie foods but are easily accessible. Despite having higher incomes and being well educated, one county level report noted that many lack the knowledge and skills to prepare healthy foods, do not know how to cook healthy foods, or lack the time needed to get groceries to cook at home, leading to higher OVO rates. 11
Black women living in PG County, Maryland, have disproportionately higher rates of obesity compared to their White counterparts (75.5% and 61.8%, respectively). This data also aligns with state and national trends.9,12 -17 Higher rates of OVO are also observed across income and education levels, suggesting that there are other determinants of health that may impact weight status among Black women.
There is a gap in the literature that examines the health behaviors of middle- to high income Black women and how social and cultural factors impact OVO. 18 This study examined the impact that social networks have on middle- to high-income Black women’s decision-making around diet and physical activity to manage their weight. It is critical to understand the decision-making pathway that influences health decisions among Black women in order to develop culturally tailored health education programs to improve the weight status and overall health and wellness of Black women living in PG County, Maryland.
Methods
Recognizing that Black women can be influenced by their social environment and culture, this study was guided by the Social Cognitive Theory (SCT); a theory that helps to conceptualize why people adopt, initiate, and maintain health behaviors. 19 The 6 constructs of the SCT are (1) reciprocal determinism, (2) behavioral capability, (3) observational learning, (4) reinforcements, (5) expectations, and (6) self-efficacy. These constructs help frame why social and cultural factors can have an impact on one’s ability to maintain and/or control their weight, the factors that contribute to decision making around healthy behavior adoption, and also the positive or negative affect one’s environment can have on them. The SCT has shown to be effective in addressing disease prevention and management of conditions like obesity.20,21
A case study design was adopted using information gathered from 2 sources (1) semi-structured interviews and (2) focus groups.
A triad approach was used to recruit 15 women by word of mouth and from existing social networks. Five women were recruited and then asked to recruit 2 additional women within their social network (eg, friends, family, church members, sorority groups). Each participant received a $25 gift card for the interview and focus group, totaling $50.00.
Each woman participated in a 1-hour virtual interview using the AnyMeeting software. Once the interviews were completed, 4 focus groups were held to further delve into the content. During the interviews and focus groups, participants were asked questions about social and cultural factors that impact their weight management decision-making. All interviews were audio- and video-recorded and transcribed verbatim. Findings were analyzed using NViVo software to identify salient major and minor themes.
Participants were screened using Google Forms to ensure they met the inclusion criteria; self-identified as Black (African, African American, or Caribbean descent), were 35 to 50 years old, lived in PG County Maryland, and had a BMI at or above 25 kg/m2 and individually earned at least $79 184 (median income for PG County). This geographic location was chosen because it is the most affluent Black suburb in Maryland22,23 making it ideal to recruit middle to high income Black women. Participants were excluded if they did not have access to the internet.
The researcher developed a semi-structured interview guide for the interviews and focus groups. This guide included a series of open-ended questions with probes to help facilitate dialog. The questions were focused on 3 themes: (1) body perception and weight status, (2) social and cultural factors impacting physical activity, and (3) social and cultural factors impacting nutrition and food decisions. Participants were allowed to submit any additional information not covered in the interview or focus group related to the topic.
Before data collection, the interview guide was field-tested with 3 women to improve the reliability of the instrument. A convenience sample was used to recruit these women who met the study’s inclusion criteria. The purpose was to assess the feasibility, duration, and comprehensibility of the survey instrument and protocol. The interview guide was modified to reword some questions, add additional questions that aligned with the research question, and the questions were reordered for better flow. Morgan State University’s Institutional Review Board (IRB) approved the study. Prior to the study, all participants gave informed consent, which was also reviewed before the start of the interviews and focus groups.
Interviews and focus groups lasted between 45 and 60-min. All 15 women participated in the individual interviews. Thirteen out of 15 women participated in 1 of 4 focus groups; 2 were lost to attrition and unable to partake in the focus groups due to COVID-19 and natural disaster. The focus groups included a mix of women from each of the social networks and lasted between 45 and 60-min.
NViVO was used to analyze the data, and the results were aggregated and arranged based on key themes. After 12 interviews, saturation was reached, with the primary themes becoming repetitious and no new information gathered. The same was observed after 3 focus groups. Data was analyzed by a single coder. The interview guide was used as a framework to guide the discussion and a code book was developed to cull out the themes. A three-step process was used to analyze the data-decontextualization, recontextualization, and categorization—to uncover behavior patterns. Researcher biases were managed by setting aside preconceived notions about individuals’ experiences, feelings, and responses to certain situations. A thorough research plan was developed that included creating interview guides that asked broad questions before delving deeper into a topic (to avoid leading the participant to a particular response) and grouping topics into specific topics. Throughout the process, the researcher kept a journal to reflect on the process to document what the researcher did, how they felt and what they thought during the research to facilitate reflexivity to examine personal beliefs, assumptions, and goals.
The ontology and epistemological tenets outlined in Creswell 24 were used to guide the researcher’s thought process and approach to conducting research. Ontology is defined as the possibility that the researcher and participant may interpret the data or information differently. Epistemological means that the researcher builds a partnership with each participant/interviewee to learn from the network of participants. 24 Having these perspectives helped to strengthen the outcomes because the researcher was able to have and support open conversations with participant during the interviews and focus groups.
Study Validity
Maxwell outlined 7 strategies to achieve validity: long-term involvement, collecting rich data, respondent validation, search for discrepancies and negative cases, triangulation, quasi statistics, and comparison to maintain quality control. Based on feasibility, some of the strategies were used to strengthen the study validity, such as collecting rich data and respondent validation, and search for discrepancies. In addition, steps to address confirmability, transferability, and auditability were used. To obtain an in depth understanding of the research question, multiple sources of data were collected from individual interviews and focus groups. Having 2 data sources gave participants multiple opportunities to express their views on the topic; leading to a richer and deeper conversation. Examples of how confirmability, transferability, and auditability were addressed include:
Confirmability: researcher asked each participant to review their transcripts and results to check for discrepancies; in addition to listening to the audio files several times to ensure the transcript was accurate.
Transferability: researcher has provided the context and boundaries of the study so that the users can apply the findings to other similar groups.
Auditability: researcher created a detailed code book, data analysis plan, and interview guide to illustrate the approach to analyzing the data and reporting the results.
The audio files and video files were reviewed, and cross referenced with the transcripts and researcher notes to ensure accuracy as well as the participants reviewed the transcripts. The researcher created an interview guide with a step by step process to ensure the research study could be replicated.
Results
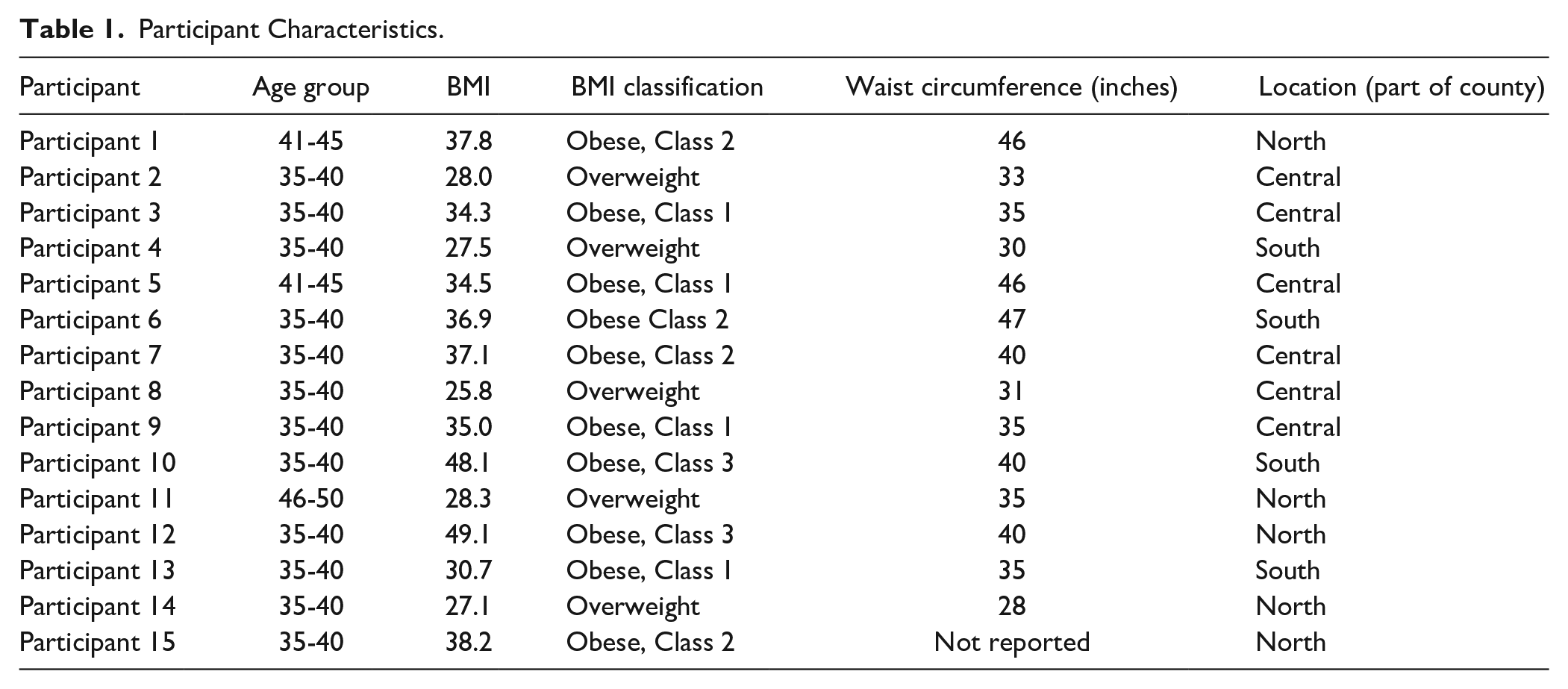
All 15 women (Table 1) were living with OVO and reported living in a state of weight imbalance most of their adult lives and impacted by major life events (eg, COVID-19, pregnancy, or college). They were highly educated, mid- to upper income group of women who valued their friendships and family. Nearly every woman in the group recognized that they were OVO, but most had a positive body image and wanted to focus on being healthy, not reaching a certain number on the scale or having the “right” BMI. Most people in their social networks were OVO, and they indicated that their peer groups influenced their decisions about how they managed their weight through nutrition and physical activity and how they interacted and engaged over food during social settings. Additionally, these women experienced common barriers to eating healthy and engaging in physical activity, some of which were influenced by their social network, such as having an accountability partner or lack of access to healthy foods or adequate spaces to work out due to where they live.
Participant Characteristics.
Three key themes emerged from the data collection: (1) body perception in the Black community, (2) culture of PG County, and (3) social and cultural impact on weight (Table 2).
Key Themes.
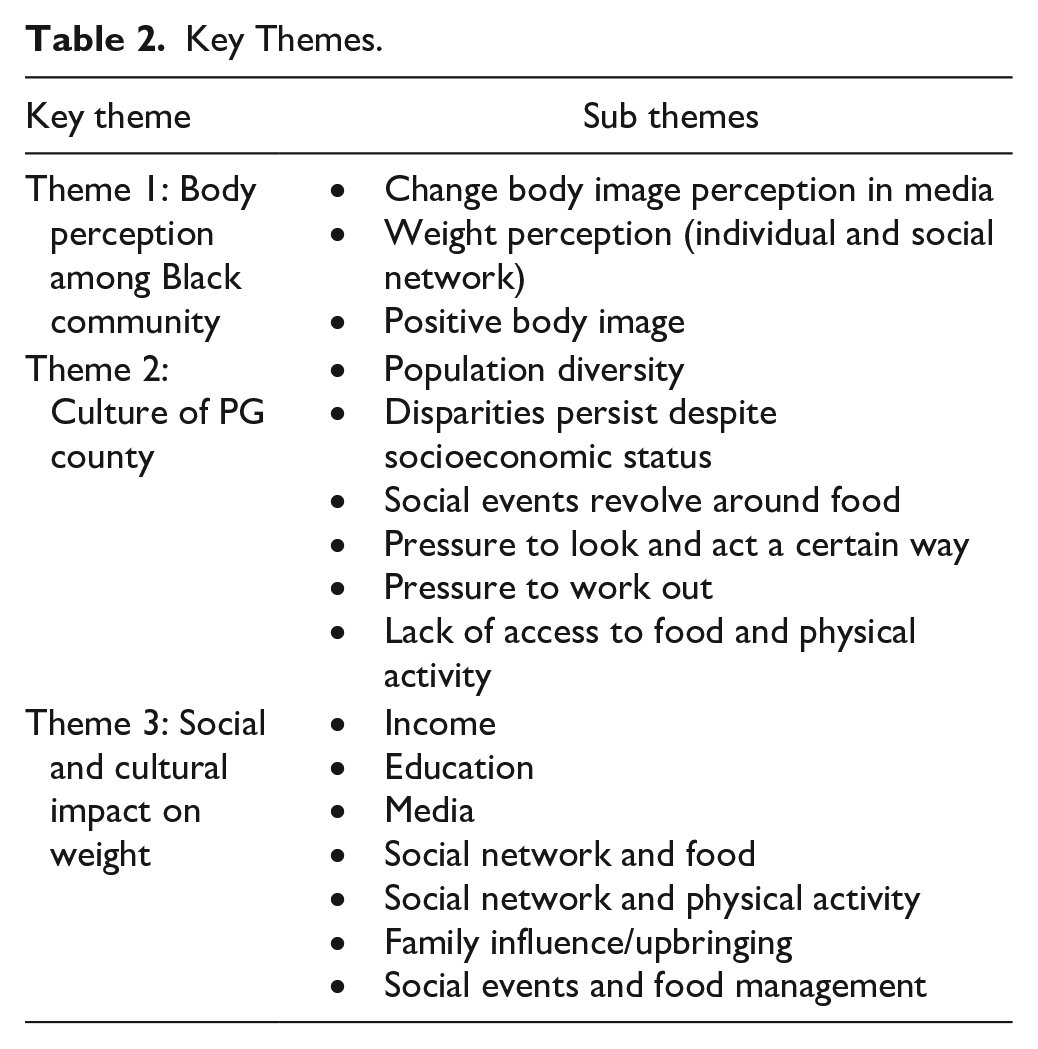
Theme 1: Body Perception in the Black Community
Participants had general concerns about how Black women are sometimes negatively perceived in the media and wanted to change the narrative to promote body positivity and positive self-image instead of reaching an unrealistic or undesirable BMI. They wanted to focus on being healthy rather than achieving a goal weight based on society’s standards. It was common for most of these women to refer to their bodies as being “curvy,” “slim sexy,” or “perfect,” while a few others viewed themselves as fat and overweight and not feeling good about it. Many had a desire to work on certain body parts like their arms or legs. Overall, most of the women had a positive body image, as 1 participant noted: “culturally I feel like size or having a little meat on your bones is not as frowned upon in our Black culture as I guess it would be in other cultures” (Participant 1). Their perceptions aligned with how their social circle perceived them and most people in their social networks did not think they were overweight. Some of their family and friends viewed their bodies as “just right” or even on the “small side.” Despite this positivity, 1 participant explained that Black women have “learned to appreciate our bodies and love our bodies but that does not mean that we take care of our bodies like we should” (Participant 15).
Theme 2: Culture of Prince George’s County (PGC)
One’s place of residence influences his/her social status and network. Theme 2 provides insights into the women’s views of PG County and how it impacts their weight management. In PG County, there is an overabundance of fast food restaurants compared to some of the predominantly non-Black nearby areas. PG County is recognized as one of the most affluent black counties in the US, but unfortunately, there are still issues with achieving good health and wellness among Black women.
The county is separated by 3 distinct regions (North, Central, and South) and participants lived in all 3 regions of the county. Many pointed out that experiences are dependent on place of residence in the county, which is dependent on personal resources. Most women viewed the county as mostly Black with a mixed range of incomes; some women were born and raised in the area, and others were transplants—moving here for college or careers, for example. Even though the women noted the affluence of PG County, they indicated that there are high rates of chronic diseases, especially among Blacks, and a lack of access to adequate green space and healthy food options.
Healthy dining options are scarce and have only recently started to pop up in some areas as noted by some participants. “There is a McDonald’s and carry-out on every corner just about and I have noticed that if you go to a more diverse area or majority White area, they have healthier options” (Participant 14). Participants stated that they feel like they do not get sufficient access to fresh produce and meats and the grocery stores options are limited with many grocery store chains leaving the area. Participant 1 said, “I don’t know if we get the end of the distribution or what. . . when I was buying vegetables and stuff that I had to prep. . .literally two days later it would be going brown.” While there are many parks and trails in the county, many participants expressed that they did not feel they had adequate access to them because they were not within walking distance and would need to drive to gain access.
This demonstrates that despite being well-off, participants still find it challenging to eat healthy and engage in regular physical activity, partly due to where they live and their lack of access to better options.
Theme 3: Social and Cultural Impact on Weight
Theme 3 highlighted the social and cultural factors that impact these women’s decisions around their weight; socializing around food played a major role.
While income and the high cost of being healthy were noted as general issues, the women could buy what they needed to be healthy, such as exercise equipment, high-end groceries, gym memberships, and personal trainers; 1 participated stated that “Fortunately, I make good money so I can buy better foods. I can shop at Whole Foods. I have all kinds of top-notch juicers and blenders” (Participant 8). Another participant said that she has “an income that allows me to try different things. If I wasn’t financially stable and made less, then I probably wouldn’t be able to afford a lot of the stuff that I have been able to do like buying an elliptical and a treadmill” (Participant 4).
All the women had college degrees. They perceived their educational attainment as a driving factor to live healthier because they were exposed to new foods and ways of preparing foods, and education afforded them higher incomes. So, it was not necessarily about learning more about nutrition and physical activity but more about the opportunities that getting higher education provides for oneself.
Media also played a role. Traditional media included television, magazines, or radio, and social media included platforms like Instagram and Facebook. Media influence was mostly positive, and women used social media mainly to get ideas for workouts and recipes (from women that looked like them) that they then shared with their network.
“I follow a lot of bigger or plus-size healthy women online. So, they may be like 220 pounds, but it’s majority muscle” (Participant 10).
Family influence, traditions, and values were major influences for this group. Participants were taught a mix of positive and negative behaviors while growing up. For example, some women grew up in families where physical activity was the norm, while others were raised in sedentary households. Learning how to cook and prepare Caribbean or Soul Food dishes at a young age was a common theme. Dishes typically consisted of fried and high-fat foods, lots of salt-based seasonings, seasoned vegetables, and processed meats. Family events were centered around food and family. Culturally, there are unspoken rules around food consumption; for example:
“I think culturally people will be offended if you don’t eat their stuff” (Participant 12).
The power of familial influence is strong. Habits that were adopted in childhood were often carried into adulthood, and most women sought to break bad habits but noted that this was hard to do.
The women’s social networks, which consisted of their friends, family members, and coworkers, influenced how they consumed food, the types of foods, how they engaged in activity, and the types of physical activity.
“A lot of my peers are very conscious of other cultures and very open to exploring other cultures and the foods of other cultures” (Participant 1).
Participant 3 stated “Black events always have food” and several other participants made similar statements. About half of participants did not want to appear disrespectful when offered food at events and felt pressured to eat even when not hungry. Nearly all of the participants said they based their outings on where they would eat and going to brunch was frequently referenced as a common outing which is centered around hours of socializing, eating and drinking, usually with alcohol. One woman noted that in her family, if multiple people were celebrating birthdays, then each person got their own table of food with their personal favorites—there was no sharing. Being successful in PG involves networking for work, which means attending cocktail parties with open bars and breakfast or coffee meetings.
Discussion
The literature is lacking any major studies that addressed management of overweight or obesity among middle-to high-income Black women. This study contributes to the literature by better explaining the underlying social and cultural factors that impact the weight of middle-to-high income Black women living in PG County. Results show that these factors are critical in the decision-making pathway for the participants and should be considered when designing weight-centric programs for these women. The programs developed could serve as a framework for additional programs tailored for women with similar characteristics in other parts of the country.
Limitations of this study included the use of a convenience sample, which only provides a snapshot of the Black women within this study and represents their unique perspectives at 1 point in time. Additionally, the data were self-reported and given the triad recruitment strategy, several of the participants already knew each other and were part of the same social network. This closeness could have resulted in them feeling more comfortable and increase their ability to freely share or perhaps avoid sharing more sensitive information. Both of which could induce bias. Lastly, there was a single coder to analyze the data. This could possibly lead to the coder failing to recognize emergent themes from varying perspectives or validating a specific theme that was expected. To lessen this bias, the coder revisited the data numerous times over a period of time to see if different perspectives or insights emerged to lessen any bias. Despite these limitations, the information gleaned from this study will enable researchers to culturally tailor programs that meet the needs of middle-to high income Black women living in PG County, considering the social and cultural norms that influence them.
Findings showed that key social and cultural factors, such as income, family network, peer network, and living in PG County, have an impact on participants’ attitudes and behaviors toward their weight and strategies to manage their weight. These results aligned with the Social Cognitive Theory. For example, many women stated that they modeled their health behaviors after members in their social group, which is a form of observational learning, a key SCT component. Another example of SCT alignment is behavioral capabilities which showed up when the participants talked about their knowledge of healthy behaviors and their ability to perform those behaviors. Certain social and cultural factors, including social networks, influenced the way the participants perceived their weight and the strategies they used to manage their weight (eg, diet and physical activity). The OVO epidemic is not new; however, Black women continue to bear the burden in terms of disproportionate rates of OVO and high rates of obesity-related chronic diseases, such as hypertension and diabetes.1 -5,9,17 And, while body positivity was shown to be high among this group, their responses indicated that there can be a disconnect between body positivity and poor health outcomes which also mirrors results reported in other studies focused on Black women.
This study reinforces research that has shown that “place matters”—where you live and work has an impact on your ability to make healthy decisions. In this study, the women lived in a county touted as one of the most affluent places for Blacks to live in America; however, the lack of access to healthy food choices and quality options for physical activity was an issue. Almost 25% of food retail outlets consisted of carry-outs, which commonly serve high fat and sodium foods. Many grocery stores were in the process of closing, and replacements had not been lined up.
Public health practitioners and researchers can use the results from this study to build better health education and promotion tools for Black women. Culture is important and should not be neglected when designing programs or materials. Due to the impact that social networks and cultural beliefs have on decision-making, it is imperative that these concepts be translated into actionable programming. Also, the women’s motivation to be healthy should be incorporated into programming. Most desired to break generational habits and focus on small changes to being healthier so they could set positive examples for their children and be healthy for themselves. This can take on the form of developing a weight loss curriculum that addresses how to overcome social norms (eg, eating food when offered) or overeating in social situations and how to address the societal pressure to feel the need to look or act a certain way as a Black woman. These will tackle the underlying reasons for which Black women make decisions about their weight. Most programs primarily focus on diets and physical modifications but do not adequately address the impact of the decision-making pathway.
Despite limitations of this study, this study can be adapted and implemented in other geographic locations with Black women of varying incomes. Some of the common barriers reported in this study were similar to other studies, such as access to quality food and physical activity options; lack of time, knowledge about general health and wellness (eg, how to prepare healthy foods), or willpower; and being influenced by media and other external factors, for example. Based on the results, a decision-tree matrix could be developed to visualize the incremental decision-making pathways Black women use to make decisions about their weight.
More data is needed on Black women. Nearly every data set in the public domain reports data by race or gender, rarely both. This is a missed opportunity to really understand the health of Black women, which is desperately needed to make well-informed policy and program decisions.
There are public health policy and practice implications for these findings. This research can help local and county-level officials address the health needs of Black women, for example, by ensuring urban planners and developers incorporate places for people to engage in physical activity and reviewing zoning laws to support the growth of grocery stores and farmer’s markets, thus increasing access to fresh and healthy foods. One way to accomplish this is to offer incentives. Lastly, more collaboration is needed. Black women need to be engaged in the planning process to ensure materials are culturally relevant and resonate with them so they can take action—this is when real change will start to happen.
Footnotes
Acknowledgements
I am thankful to the support provided by my Morgan State University professors who provided their guidance and expertise during my doctoral research; Dr. Sharon Barrett, Dr. Lorece Edwards, and Dr. Ian Lindong. This work would not be possible without the dynamic Black women who participated in this study and the support of my family and friends.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.