
Abstract
The Comprehensive Care Initiative (CCI) utilized a quasi-experimental design to evaluate the effects of same room, multi-provider primary care visits on the management of type 2 diabetes (T2D). Patients with T2D were invited to enroll in CCI if they had T2D with glycated hemoglobin (HbA1c) >8.0% or T2D with BMI >30. CCI intervention included delivery of comprehensive same room multi-provider visits with a primary care physician, community health worker, pharmacist, dietitian, medical assistant, and licensed social worker at the same appointment. CCI patients were compared with a propensity score matched control group receiving usual care (n = 56, 50 ± 11 years old, 77% female, 41% African American, 95% uninsured). After 6 months, the adjusted average reduction in HbA1c in the CCI group was 0.97% (SE = 0.45) in comparison to 0.05% (SE = 0.20) in the control group (P = .04). This pilot study showed promising results in lowering HbA1c in an uninsured, ethnic minority population of T2D patients through delivery of comprehensive multi-provider primary care visits.
Keywords
Introduction
Effective T2D management requires integrated primary care that combines input from the primary care physician along with that from other care providers such as dietitians, pharmacists, and social workers. Fragmentation of care, when appointments are scattered across days and times, and limited opportunities to share clinical information between care providers, are challenges commonly highlighted in the Chronic Care Model. 1 This is particularly important for patients in low resourced communities. Patients in low-income communities commonly report transportation, anticipated costs, and lack of information about discounted medical care as perceived barriers to access health care services. 2 Furthermore, the most reported barrier is lack of health insurance coverage, with minority groups being more likely to be uninsured. 3 The CCI study evaluated an innovative, comprehensive care model for patients with uncontrolled T2D in a low income, ethnic minority community. This study utilized same day, same room visits with a primary care physician, pharmacist, dietitian, community health worker, medical assistant, and licensed social worker who all shared clinical information to coordinate care.
Research Design and Methods
Patients were recruited from the Baylor Scott & White Health and Wellness Center (BSW HWC) primary care medical home. BSW HWC is in a low resourced, urban community and serves more than 2000 patients annually regardless of ability to pay. The CCI study enrolled patients who were diagnosed with T2D and had either elevated glycated hemoglobin level (HbA1c) >8.0% or BMI >30. Patients who attended 3 or more CCI appointments within 6 months were included in the analyses. CCI appointments used a comprehensive, multidisciplinary primary care approach in which 4 of 6 available healthcare and wellness providers were involved with the CCI patient visit in 20-min intervals during a single office visit. The CCI clinical team consisted of the primary care physician (PCP), pharmacist, dietitians, community health workers (CHWs), licensed social worker, and medical assistant. CCI patients received personalized goals based on patient needs. Shared treatment plans were developed for each patient through coordinated weekly and monthly pre-visit planning meetings amongst the CCI clinical care team members. Revisions to the shared treatment plans were also based upon quarterly data reports of patient progress and attendance of appointments. At each follow-up visit, members of the CCI clinical team monitored and evaluated the patients’ progress in managing diabetes based upon changes in diabetes-related clinical study measures, prescribed medication use, along with self-reported changes in self blood glucose monitoring and physical activity measured in minutes. Clinical care was led by the PCP with the support of a medical assistant. Medication management was provided by the pharmacist while nutritional guidance was delivered by dietitians. The licensed social worker contributed continuous support in addressing social needs. CHWs enrolled patients in membership at BSW HWC to provide access to additional community-based support services including group exercise classes, chronic disease education, and the BSW HWC farm stand. All participant appointments were scheduled by clinic staff and appointment reminder calls were completed per usual care. In the case of a no-show appointment, patients were contacted the same day to reschedule for next available appointment within 1-week. The program did not provide transportation for participants.
The primary outcome measure of HbA1c was extracted from the patients’ electronic health record (EHR) at baseline (enrolled on a “rolling” basis) and 6 months after initial enrollment date. Secondary outcome measures included body mass index (BMI), weight in pounds (lbs.), and systolic blood pressure (SBP). Propensity score matching was used to select a control group. To account for geographical variation, the potential control group was selected from the same zip code as CCI patients. The variables used for matching were patients’ baseline HbA1c, age, sex, race, and health insurance status. 4 The control group patients attended the same community clinic and had access to the same clinical team via referrals and warm handoffs. Demographic variables and baseline HbA1c were compared between intervention and control groups using 2-sample t-tests for continuous variables and chi-square tests for categorical variables. Within group changes from baseline to post-intervention were evaluated for HbA1c, body weight, BMI, and systolic blood pressure for both groups using paired t-tests. A general linear model was used to estimate the adjusted effect of the intervention as compared to control on HbA1c at 6-months adjusting for baseline HbA1c, age, race, and sex.
Results
At the time of analysis, 56 patients were enrolled in the study, 28 from the CCI group and 28 matched controls. On average, patients were 50.0 (SD = 10.82) years of age, 76.8% female, 58.9% Hispanic, 41.1% African American, and 94.6% were uninsured. Patients who attended ≤2 CCI appointments were excluded from the analyses (n = 14). There were no statistically significant differences in patient demographics between the CCI and control groups. At baseline for the CCI group, average (SD) BMI was 36.37 (7.64), average weight was 212.13 (54.51) lbs., and average systolic blood pressure was 128.29 (13.79) mmHg. For the control group at baseline, average BMI was 34.87 (9.28), average weight was 208.07 (65.13) lbs., and average SBP was 126.46 (14.15) mmHg. Patient BMI, weight and systolic blood pressure did not demonstrate a statistically significantly change at 6-months for either group.
For the CCI group, the average (SD) HbA1c at baseline was 9.76 (1.67) % and decreased to 8.80 (1.30) % at 6-months, equaling a mean reduction of 0.96 (SD = 1.98) (P = .02). The control group had an average HbA1c of 9.95 (1.69) % at baseline and 9.90 (2.18) % at 6-months with a mean reduction of 0.05 (1.89) (P = .90). After adjusting for baseline HbA1c, age, sex, and race, the average reduction in HbA1c for patients in the CCI group was 0.97 (SE = 0.45) in comparison to an average reduction in HbA1c of 0.05 (SE = 0.20) in the control group at 6-months (P = .04). The adjusted average HbA1c at 6-months was 0.88 (SE = 0.55) % lower for the female patients than the male patients (P = .12).
Figure 1 presents the average (SD) HbA1c at baseline and 6-months by sex and race in the CCI and control groups. In the CCI group, female patients had an average of 1.30 (1.94) unit reduction in HbA1c (P = .005) while the male patients had a slight increase of 0.27 (1.75) (P = .72). In the CCI group, Hispanic patients had an average of 1.05 (1.88) unit reduction in HbA1c (P = .04) in comparison to African American patients who had average of 0.83 (2.21) unit reduction in HbA1c (P = .24). There were no significant differences by sex or race from baseline to 6-months in HbA1c for the control group.
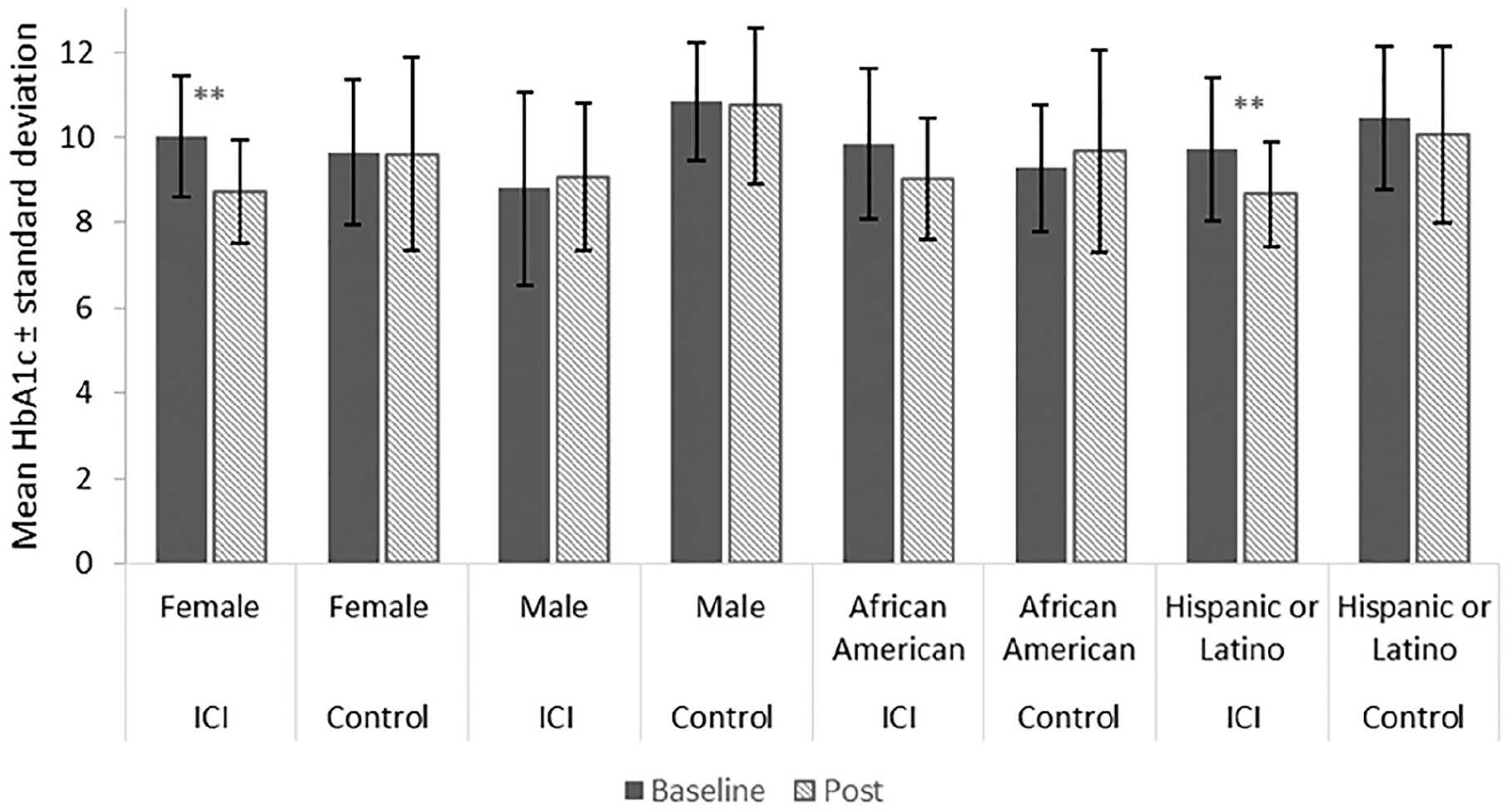
Average HbA1c at baseline and 6-months in CCI and control group by sex and race.
Discussion
This pilot study is one of the first to investigate the efficacy of comprehensive, same room, multi-provider clinical visits in the management of T2D based on the CCM. CCI utilizes an innovative approach to patient-centered primary care that has been adapted to meet the needs of a low resourced, ethnic minority community. CCI appears to have improved the management of T2D by reducing barriers from within and without the healthcare system. The collaborative approach for patient case management utilized by the CCI may decrease barriers for providers to share clinical information and contribute to positive clinical outcomes. 1 The comprehensive, same room, multi-provider clinical visit model also appears to decrease patient barriers reported in the literature. 2 These aspects should be further investigated in future research.
The strengths of the study include the involvement of a multidisciplinary team of providers to develop integrated, individualized multidisciplinary care plans at the primary care level along with the successful implementation of coordinated, patient-centered clinical visits in which providers rotate versus typical visits in which patients are mobilized through various areas of the clinic to meet with providers. This is supported by the significant reduction in the primary outcome measure, HbA1C. One potential weakness of the study is that patient-satisfaction and healthcare cost savings were not evaluated. Another potential limitation is that patients who did not meet the required dose of 3 or more sessions were excluded from the analyses.
Additional research is needed to confirm and further develop the model presented in this paper. Future research could allow further exploration of the differences in outcomes by sex and ethnicity demonstrated in this study. It is also important to evaluate feasibility of the intervention in a larger sample size. Our results support the expectation that the comprehensive, multi-provider primary care model utilized in the CCI could be beneficial in the management of T2D.
Conclusions
The CCI was found to effectively improve the primary T2D management outcome of HbA1c in a primarily uninsured, ethnic minority population. This outcome shows that delivering collaborative primary care and wrap around services could be more effective in controlling T2D when compared to patients receiving usual care. Previous studies show that utilizing elements of the Chronic Care Model (CCM) improve intermediate outcomes in diabetes care.5,6 The CCI may also reduce multiple barriers to healthcare access in lower income populations. Transportation, anticipated costs, lack of health insurance, childcare needs, limited individualized care, and time off work have been identified as perceived barriers to healthcare access in urban, low income populations in previous studies.2,3 Preliminary findings from the CCI suggest that combining elements of the CCM with integrated clinical patient visits could more effectively reduce HbA1c in uncontrolled type 2 diabetics in low-income, ethnic minority communities and reduce perceived barriers, however further study is needed. Further evaluation is also needed to measure cost-effectiveness and feasibility of the CCI intervention in larger samples as a potential value-based care approach for high-need patients.
Footnotes
Author Contributions
AHM wrote the manuscript and researched data. LB conducted the research and reviewed/edited the manuscript. HK contributed to the conclusions and reviewed/edited the manuscript. MK conducted data analysis and contributed to the results. AM conducted data analysis and reviewed/edited the manuscript. AA contributed to the research design and methods. KG contributed to the research design and methods.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agnes Cluthe Oliver Foundation.