
Abstract
Although the importance of control in reducing the morbidity and mortality from diabetes is well established, it is often not achieved.1,2 Factors contributing to poor control include inadequacies in patient self-care behaviors, medical management, or both. 3 In urban areas with well-insured patients, these factors are often managed by a multidisciplinary team of clinicians specializing in diabetes. However, these teams are often not available in rural areas, particularly to patients with limited English skills. We developed a technology-based intervention designed to help patients with diabetes lacking access to multidisciplinary diabetes specialty care.
The diabetes management program (DMP) was implemented for patients with diabetes in a rural primary care office who did not choose to consult a multidisciplinary specialty care. The DMP performs the following functions: (1) administers extensive questions to the patient regarding multiple dimensions of patient self-care behaviors and barriers to these behaviors (Self-care Behaviors Survey for Patients With Diabetes), (2) generates a report summarizing the key results from the patient questionnaire serving as a reminder for the health care provider concerning possible interventions appropriate for patients who respond to specific questions (see Appendix A for a sample summary of the patient questionnaire), and (3) creates a 1-page summary of the most important clinical information needed to manage a patient with diabetes from the medical record data (see Appendix B for sample clinical summary). The products from the DMP are helpful for diabetes management to the extent the patient and health care provider refer to them and implement change based on problems identified.
The purposes of this study were to (1) describe the current practices and health care provider management of patients with diabetes in a rural primary care office and (2) determine if there are differences between Hispanic and non-Hispanic persons concerning diabetes self-care behaviors and barriers to self-care and discover which of the behaviors and barriers are associated with diabetes control as measured by the glycosylated hemoglobin (HbA1c) level. The second purpose evolved as the office had substantially different ethnic groups.
Methods
The DMP was implemented at the University of Iowa Health Care-River Crossing office in Riverside, IA. Many of the office’s patients come from rural areas around the city with a catchment area of 3182 persons. The office treats 4300 patients per year. Around 2% of the patients have documented diabetes, and 60% are Latino. Approximately 55% of the office visits are covered by private insurance, 10% by Medicare, 25% by Medicaid, and 10% have no insurance. Two board-certified family physicians and a physician’s assistant see patients in the office.
In March 2009, 86 persons attending this office were identified as having diabetes using the International Classification of Diseases–9 diagnostic diabetes code. Seven of those persons were excluded from a mailing, as they were residents of a nursing home or had gestational diabetes. Seventy-nine patients with diabetes were sent a cover letter describing the DMP, a questionnaire, and a postage-paid return envelope. For nonresponders, a reminder letter was sent 3 weeks later, and a month later a second full packet with cover letter, duplicate questionnaire, and postage-paid return envelope was sent. Nonresponders were attempted to be reached twice by research assistants (bilingual when appropriate) to ask if they had any questions or concerns about the questionnaire and were encouraged to return it. As new patients with diabetes enrolled at the office, the same mailing process was conducted. Four additional patients were sent the mailings during the study. Of the total of 83 patients identified with diabetes, 61 (74%) returned the patient questionnaire. Twenty-seven (33%) of the patients with diabetes were Latino, as identified by office staff. Those individuals received materials in Spanish.
After the questionnaires were returned, they were double-entered in Web Surveyor (http://www.vovici.com) and verified for accuracy. A summary for problem behaviors was generated for each patient. The summary was then scanned and placed in the patient’s electronic medical record. A paper copy was also given to the primary care provider.
Diabetes Questionnaire Instrument
The 127-item questionnaire, “Self-care Behaviors Survey for Patients With Diabetes,” was developed by a research team at the University of Iowa over a period of 7 years. 3 It has been pilot tested in many offices and reviewed by dieticians, nurses, physical therapists, and physician experts managing persons with diabetes. It is composed of the following domains: sociodemographic, family support, health risks, mental/physical health, physician-patient communication, self-care behaviors, and potential barriers to diabetes management. The questionnaire has a Flesch-Kincaid readability scale of 5.0 grade level.
The Spanish version of the questionnaire has been through numerous translations. A final review of the Spanish version of the questionnaire was completed by a Spanish-speaking medical student who also aligned the English and Spanish questionnaires to be the same for each page. The medical student also translated all cover letters that went out with the questionnaires, which were then approved by the primary care Spanish-speaking physician.
Institutional Review Board
The lead physician (DB) in the blinded study wanted to improve diabetes care in the office. Thus, he directed the mailings of the questionnaire to patients in his practice. Once this was done, the institutional review board approved a retrospective medical record review of diabetes-related medical information.
Medical Record Reviews
The medical record reviews were conducted using both the paper medical records and the electronic medical record. Information about gender, race, height, weight, medications, medical diagnoses, initial year seen in the practice, date and reason for visits over the past 3 years (acute care, diabetes follow-up, or physical examination), laboratory values (HbA1c, lipids, serum creatinine, urine protein, microalbumin), blood pressure at each visit, visual foot examination and/or comprehensive foot examination, referral for dilated eye examination and podiatry, whether patient brought blood glucose values to the visit, whether health care provider reviewed the blood glucose values and made recommendations for glucose monitoring, and immunizations. Medical record documentation of diabetes education was also recorded.
Data Analysis
The main outcome variable, HbA1c, was tested for an association with each potential predictor variable. Spearman correlation coefficients were used to assess the relationship between outcome and predictor variables. Univariate analyses using t tests or a 1-way analysis of variance were used to assess significant differences in mean HbA1c.
Barriers to self-care of following the recommended meal plan, taking medications as prescribed, testing blood glucose, and exercising regularly were measured using a scale of 1 (no extent) to 5 (a very great extent). Dichotomous variables were created for each barrier such that the barrier was considered a significant problem if the patient rated it a 4 or a 5. Satisfaction with performance of each behavior was measured on a rating scale of 1 (not satisfied) to 5 (very satisfied). Dichotomous variables were created for each satisfaction question as satisfied if the subject rated it a 4 or 5. Chi-square tests were used to determine if there were associations between 2 categorical variables. Fisher’s exact test was used when there was a small value (less than 5) in 1 of the cells.
Results
Sixty-one (74%) of the 83 patients with diabetes completed the questionnaire and had the DMP implemented (problem summary and clinical summary generated). Medical record review was completed for 83 (100%) subjects. Forty-five (54%) of the subjects were men, with a mean age of 63 years (range, 18-94 years). Fifty (60%) of the subjects were married, and most (88%) had insurance.
Non-Hispanic subjects were significantly older, with a mean age of 67 years compared to the mean of the Hispanic groups of 53 years (P > .001). No significant differences were found between the 2 ethnic groups regarding gender, marital status, education, years since diagnosed with diabetes, and body mass index.
The Hispanic group had a significantly lower income, with 79% in the less than $30 000 group and 21% in the $30 000 to $75 000 group, compared with 23% of non-Hispanic in the less than $30 000 group, 27% between $30 000 and $75 000, and 7% above $75 000 (P = .015). Non-Hispanic persons had significantly more insurance coverage than did the Hispanic persons, which had 7 persons not covered (see Table 1).
Univariate Association of Glycosylated Hemoglobin (HbA1c) With Demographic Characteristics, Health Risks, Self-care Behaviors, and Barriers by Ethnicity: Medical Record Review

P < .05.
P < .001.
P < .01.
All subjects had diabetes for a mean of 9 years, with a mean HbA1c of 7.5% (range, 5.5%-14.0%). There was no significant difference in length of time diagnosed with diabetes by ethnicity. Overall, HbA1c was significantly higher for the younger group and the women (see Table 1). Comparing Hispanic and non-Hispanic persons, Hispanic women and married persons had significantly higher HbA1c than did non-Hispanic and unmarried persons. Hispanic persons had a significantly higher HbA1c when insured compared to the non-Hispanics. Overall, those insured had a lower HbA1c than did those not insured. No uninsured person had diabetes education or nutrition classes. Hispanic persons who were obese had significantly higher HbA1c (see Table 1). There were no significant differences by ethnicity for smoking and education.
On a 1 (not satisfied) to 5 (very satisfied) scale, all subjects reported being neutrally satisfied (2.89) with following their meal plan, highly satisfied (4.51) with taking their medication, satisfied (3.67) with testing their blood glucose, and neutrally satisfied (2.73) with their amount of exercise. Non-Hispanic subjects were very satisfied (4.79) with taking their medications, and Hispanic subjects were satisfied (3.73), a significant difference (P = .002).
All subjects reported following their recommended meal plans 63% of the time, taking their medications for diabetes 93% of the time, and testing their blood glucose 69% of the time. No significant differences were noted by ethnicity for following a meal plan and testing blood glucose. Non-Hispanic subjects reported taking their diabetes medications 99% of the time and Hispanic subjects 50% of the time (P = .057). Subject satisfaction with self-care behaviors and percentage time doing the behavior were significantly correlated for following a meal plan (rS [Spearman correlation] = 0.85, P < .001), taking medications (rS = 0.43, P = .005), and testing blood glucose (rS = 0.53, P < .001).
Subjects reported doing both vigorous and moderate activities a mean of 4 days per week: a mean 41 minutes each time for vigorous activities and 39 minutes for moderate activities. Non-Hispanic subjects spent significantly more time on vigorous activities compared to the Hispanic subjects (see Table 2).
American Diabetes Association 2010 Standards of Medical Care in Diabetes
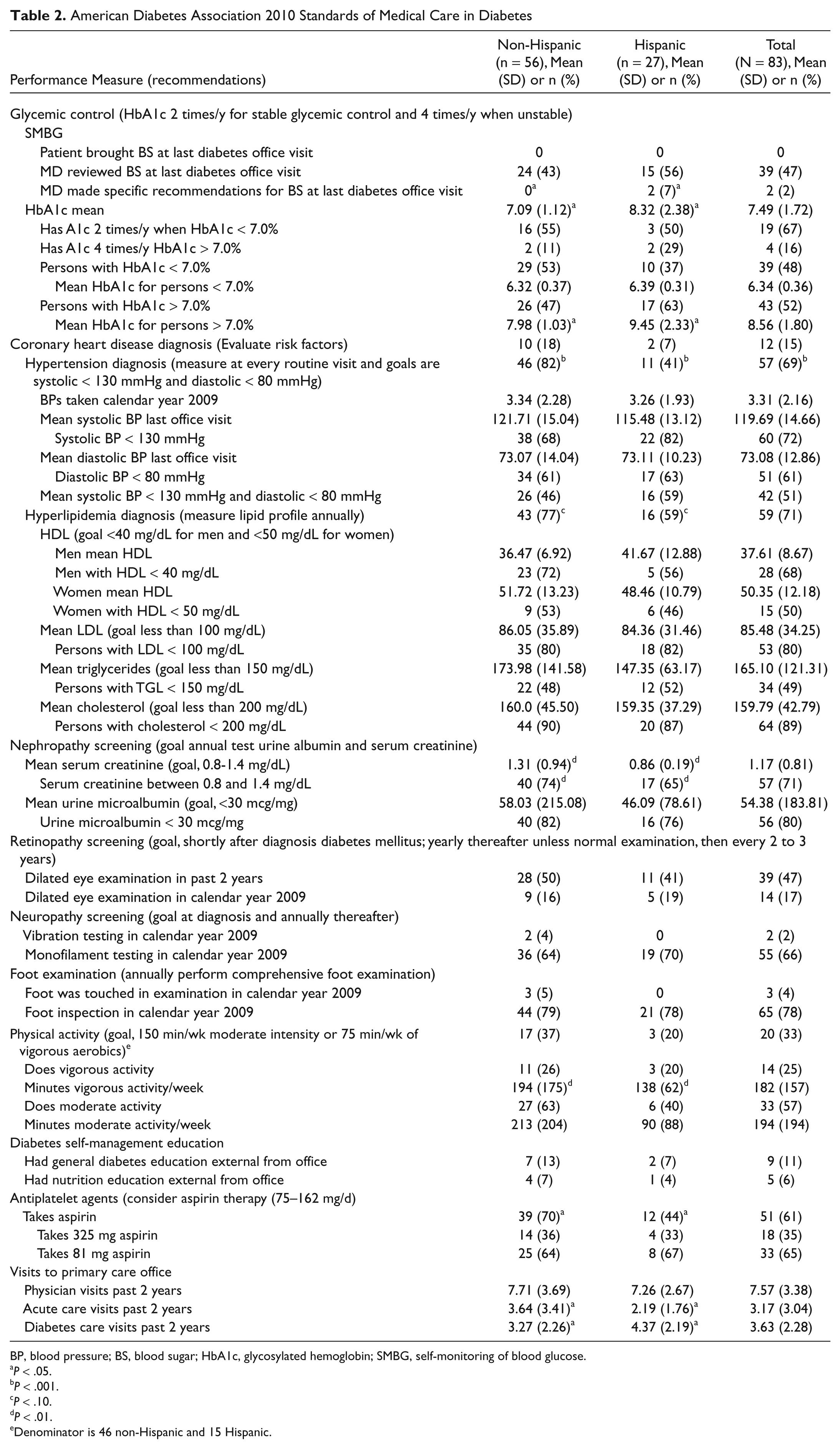
BP, blood pressure; BS, blood sugar; HbA1c, glycosylated hemoglobin; SMBG, self-monitoring of blood glucose.
P < .05.
P < .001.
P < .10.
P < .01.
Denominator is 46 non-Hispanic and 15 Hispanic.
Finding it difficult to follow a meal plan was a barrier to self-care behaviors. Those who reported this as a great problem had significantly higher HbA1c; in the ethnicity group, Hispanics who had a greater problem had a higher HbA1c. Three Hispanic persons stated having no medications at times was a problem (see Table 3). Where there was less involvement of family in providing help and support with the diabetes, the HbA1c was higher in the Hispanic group (see Table 1).
Comparison of Sociodemographics, Barriers to Self-care, and Family Support by Ethnicity: Survey Results a

Fisher’s exact test.
Satisfaction scale of 1 = not satisfied to 5 = very satisfied.
Hispanic persons had significantly more barriers to self-care of diabetes management, such as being too tired to exercise and fear of falling and injury while exercising, than did non-Hispanic persons (see Table 3). Cost was also a barrier for Hispanic persons in purchasing medication and making physician office visits (see Table 3). In many aspects of diabetes management, significantly more Hispanic persons wanted their family support in exercise, blood glucose testing, visiting their doctors, checking their feet, following a meal plan, and taking their medication (see Table 3).
Fifteen (18%) of the subjects had never heard of the HbA1c, and 10 (19%) had heard of the HbA1c but did not know what their level should be. Eleven (21%) subjects felt the HbA1c should be 7% or higher, and 17 (32%) felt the HbA1c should be 5% or 6%.
Nine (17%) subjects did not know what their blood glucose should be before meals, whereas 30 (58%) thought it should be between 90 and 130 mg/dL, and the remaining 13 (25%) thought it should be 90 to 150 mg/dL or greater. Those subjects who answered that their blood glucose level had ever been higher than 300 mg/dL or did not know if their blood glucose levels had ever been higher than 300 mg/dL had higher HbA1c levels (P < .05).
Standards of Medical Care in Diabetes in a Rural Primary Care Office
The standards of medical care in diabetes provide (1) components of diabetes care, (2) general treatment goals, and (3) tools to evaluate the quality of care. 4 A summary of these components is provided for this study in 1 rural primary care office according to Hispanic and non-Hispanic status (see Table 2).
From the medical record review, documentation of patients bringing blood glucose records to the office visit was noted for 3 persons. However, review of blood sugar was completed for about half of the subjects, and only 2 patients received recommendations for blood sugar self-monitoring at their last office visit. About half of the subjects had HbA1c below 7%; not all subjects were receiving HbA1c testing according to the frequency recommended by the American Diabetes Association guidelines.
Significantly more non-Hispanic persons had hypertension and hyperlipidemia diagnoses than did the Hispanic persons. Blood pressures were taken at every office visit with the mean systolic and diastolic pressure in this group within the range recommended by the guidelines. Seventy-two percent of all subjects were in the recommended systolic blood pressure range, 71% in the recommended diastolic blood pressure range, and 51% both systolic and diastolic blood pressure in the recommended range.
No significant differences in the 2 groups were noted for HDL, LDL, triglycerides, and cholesterol. Most persons were in the appropriate range for their cholesterol and LDL levels. About half of the subjects were in the appropriate range for their HDL and triglycerides.
Significantly more non-Hispanic persons had serum creatinine in the recommended range, whereas the mean value of 1.31 was higher than that of the Hispanic group. Urine microalbumin was similar across the 2 groups. Overall, about two thirds of the subjects had a serum creatinine and urine microalbumin completed within the past 3 years.
Retinopathy and neuropathy screenings were documented in the medical records, with about 50% having a dilated eye examination in the past 2 years and 66% having a monofilament testing in 2009. Foot inspection was documented for 78% of the participants.
Depression diagnosis was similar across groups, with 28% having the diagnosis. According to the Patient Health Questionnaire (PHQ-9) responses, moderate/major depression trended higher for Hispanic persons with a mean score of 7.7. The non-Hispanics had a mean score of 4.3, which was significantly different (P = .025).
Only 14 persons reported doing vigorous activity, and 33 reported moderate activity, with an overlap of 13 persons reporting both. Twenty subjects (33%) met the guideline of reporting either 75 minutes of vigorous activity or 150 minutes of moderate activity. A mean of 194 minutes of vigorous activity was significantly higher for the non-Hispanic group. Subjects who responded that they would be willing to exercise more than 30 minutes a day had lower HbA1c levels than those who did not (P = .001).
Very few subjects went to diabetes management or nutrition classes external to the office setting. Only one-on-one instruction is provided at the office by the health care providers.
Sixty-one percent of the subjects take aspirin, with the majority taking 81 mg compared to 325 mg. Both groups had a similar number of physician visits in the past 2 years, with a mean of 8 visits. Hispanic persons had significantly more diabetes visits than did the non-Hispanics and with fewer acute care visits.
Discussion
It was feasible to implement a DMP in a rural primary care setting, as 74% of the persons with diabetes completed and returned the questionnaire. The implementation, though, was time consuming and costly and was facilitated outside of the usual realm of practice. From the patient’s medical record, medical students entered the questionnaire data into a software program to generate the Summary of Patient Questionnaire (see Appendix A). The students also abstracted information from the patient’s medical record to generate the clinical summary (see Appendix B). Those documents were then uploaded into the electronic medical record, and a paper copy was given to the primary care physician and mailed to each patient. From the information obtained through the questionnaire and medical record, a compilation of standard of medical care for diabetes was generated, which indicates strengths and weaknesses of office productivity and medical record recording.
Comparisons for sociodemographic characteristics and health risks were provided by ethnicity group to discern additional differences between the groups. Differences were found between the 2 ethnic groups: female Hispanic persons, married Hispanic persons, and overweight and obese Hispanic persons had higher HbA1c than did their counterparts. According to several studies on the subject, diabetes does affect the poor and members of ethnic/racial minorities at a higher rate than that of other groups. Prevalence of diagnosed persons 20 years and older with diabetes in the United States is 6.6% for non-Hispanic whites and 10.4% for Hispanics. 5 Minorities have worse adherence to self-care, worse diabetes control, and higher rates of serious diabetes-related complications.6-8 As noted in this study, persons with poor adherence satisfaction for self-care behaviors of following their meal plans, taking their medications, testing their blood glucose, and exercising had higher HbA1c, and the highest HbA1c levels were in this Hispanic group. The Hispanic group also exercised less than did the non-Hispanic group. In reviewing the lipid and kidney function tests between the 2 groups, there were no significant differences in complications noted. Subjects indicated a valuable source of support for diabetes management was their family members. Instructions and education provided during an office visit could be expanded to include family members.
Twenty-eight percent of the subjects carried a diagnosis of depression, whereas 18% had the criteria for moderate/major depression on the PHQ-9. The PHQ-9 indicated 3 persons not diagnosed had symptoms of depression. Patients with diabetes and depressive symptoms had worse adherence to self-care guidelines and glycemic control. In this study, those persons with depressed symptoms did not have lower adherence satisfaction with following their meal plans, taking their medications, testing their blood glucose, and exercising, nor did those persons with depressed symptoms have different glycemic control.7-10
Even when Latinos have health care insurance, their quality of care may be limited by the coverage of insurance, the shortage of health care professionals, and the lack of interpreters with medical background. 11 Even with insurance coverage, the Latinos have difficulty getting off work for nonemergency or acute office visits. Many nonemergency health care needs go unmet for Latino/Hispanic adults, particularly in the areas of preventive services and chronic care management. 11 Very few of the Hispanics (13) at this clinic went for external diabetes or nutrition classes, although a local tertiary care center has a diabetes self-management education program.
The implementation of this DMP highlighted the ethnic differences for Hispanics and non-Hispanics in diabetes self-care behavior, barriers to self-care, and family support for diabetes management. Knowing these differences provides health care providers additional information for providing diabetes care. The implementation also allowed the office to note their discrepancies in performance measures as listed in the recommendations by the American Diabetes Association guidelines.
In a recent report on the implementation of the standards of care for diabetes, only 57% of adults with diagnosed diabetes had achieved an HbA1c less than 7%, slightly higher than this office of 48% achieving that goal. 12 Fifty-one percent had achieved a blood pressure within the guidelines of less than 130/80 mmHg compared to 46% in the report. 12 Of the 72 who had a cholesterol test, 89% had a cholesterol level less than 200 mg/dL compared to 47% in the report. 12 Of the 69 who had a triglyceride test, 49% had a triglyceride less than 150 mg/dL, slightly higher than the 47% in the report. 12
An important finding from this study is that the validity of the questionnaire was confirmed by the fact that persons saying they had difficulty following a meal plan had a higher HbA1c. Again, the questionnaire was validated by the fact that those with less family help and support had higher HbA1c.
The ramifications of this implementation of this DMP are just beginning to be felt by the patients and staff at this practice. The family physician is reviewing the summary sheets with the patients at each office visit. Some patients have brought their summary sheets to the office to review specific items for further discussion. Diabetes management takes a team effort involving the health care providers, the patients, and their family members. It is an ongoing effort that needs continual support.
Footnotes
Appendix A
Summary of Patient Questionnaire
Appendix B
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors disclosed the following financial support for the research and/or authorship of this article: Financial support for the research was provided by the Department of Family Medicine, Carver College of Medicine, University of Iowa, Iowa City, IA.