
Abstract
Introduction
There is a growing body of literature that conceptualizes health stigma and discrimination in relation to the production of harmful consequences for those who face social and structural inequities.1-3 One such inequity linked to poor health is having low socioeconomic status, such as the estimated 235 000 Canadians who experience homelessness each year. 4 Homelessness is associated with poor health outcomes,5-7 including higher incidence of traumatic brain injury, 8 bodily injury, 9 and increased mortality. 10 Canadian studies with homeless populations indicate 75% have untreated dental conditions, 11 85% have at least 1 chronic health condition, and over 50% report a diagnosed mental illness. 12 Chronic pain is a significant health issue for this population as well. 13 Canadian research has found homeless persons report experiencing chronic pain for 10.3 years, with an average onset age of 35.8 years; this pain is most commonly located in the back (52%), knees (29%), and shoulders (21%). 14 For this population multiple morbidities are common, 7 including the reporting of substance abuse co-occurring with mental illness 15 and pain. 16
Health Care Access
Lacking access to primary care services is a recognized gap in the care of homeless populations, 17 with Canadian and American studies finding that only 43%, 18 51%, 19 and 56% 14 of homeless participants have a primary care provider. Homeless individuals are significantly more likely to be connected to a primary care provider if they over the age of 50 years, 20 and/or have a chronic health condition, 18 regular contact with a community health nurse, 19 or a concurrent disorder. 15 The chances of having a primary care physician have been found to decrease significantly with each additional year spent homeless. 18
As a population, homeless individuals are frequent users of emergency care services. A review of the 2005-2006 National Hospital Ambulatory Medical Care Survey found that those who were homeless made 72 visits per 100 persons in the United States annually. 21 The reasons for these emergency department (ED) visits include medical as well as social needs, such as hunger and seeking safety.22,23 Suffering injuries, whether unintentional or self-inflicted, accounted for 55% of ED visits in 1 study of homeless patients. 24 Chronic pain is another reason these individuals commonly seek acute care. In 1 Canadian study, 34% of participants reported seeking care for pain from a physician other than their primary care practitioner in the preceding 3 months, and 27% reported they needed health care for pain during this time but were unable to get it. 14 Homeless individuals have been found to have significantly greater psychiatric needs than housed patients who access ED services,25,26 and the diagnoses of concurrent mental health and substance-related disorders are higher for ED users who are homeless than those who are not.15,21
Barriers and Facilitators to Access
There are many barriers homeless people experience while navigating the health care system. Within Canada, researchers have found that these barriers to access commonly include social, structural, financial, emotional, and geographical considerations.27,28 Discrimination is common when homeless patients seek health care 29 and patients may worry disclosing their housing status will result in stigmatization from care providers. 30 In 1 study, homeless patients described unwelcoming health care encounters as being dehumanizing and they characterized their experience as being rushed or subjected to rude treatment. 31 When homeless individuals feel marginalized or that their concerns are not adequately addressed, it can have a negative impact on their overall health-seeking behavior and engagement. 32
Treatment for chronic pain is one area where perceived discrimination may lead to negative patient outcomes for the homeless. A survey of primary care providers found that an estimated 38% of weekly adult appointments involved patients with chronic pain complaints. 33 Patients in general have reported suboptimal primary care interactions when seeking care for chronic pain due to suspicions of drug-seeking, having their symptoms dismissed as trivial, or feeling that they have been disrespected. 34 Within emergency care settings, providers and patients also agree that chronic pain is considered a low-priority concern. 35 Those who are homeless may fare even worse than the general population. Primary care physicians can be reluctant to prescribe narcotics to patients with a known history of substance misuse and treatment can be complicated by psychiatric comorbidities, missed appointments, and a lack of coverage for alternative or complementary therapies. 14 Persons who are homeless face significant barriers to medication adherence23,36 and may not be well-served by withdrawal management policies in hospital settings. 37
The literature clearly identifies that homeless populations have poor health, limited access to primary and emergency care, and may face discrimination in these settings. What is lacking is a deeper understanding of how persons experiencing homelessness feel their care is affected by clinician perception of their housing status. Thus, the research question is, where do vulnerably housed or homeless individuals receive health care and what needs do they feel are not adequately addressed in these settings due to clinician bias?
Methods
Interviews were conducted and analyzed following Fraser’s narrative inquiry approach. 38 Narrative inquiry is a well-founded method in research with health care patients39,40 and individuals experiencing homelessness41,42 because it captures individual experiences through the participants’ own words. Phase 1 was to hear the stories and associated emotions directly from participants. 38 Interviews lasted approximately 30 to 60 minutes and were conducted by the authors or a trained senior research assistant. Prior to the commencement of data collection, all research assistants participated in a 1-day training session led by the authors, which included seminars on research with vulnerable populations, ethical considerations, and mock interviews. In the field each interview was conducted with 2 members of the research team present, 1 to serve as the interviewer and 1 to take handwritten notes. Interviews were also audio-recorded. The research assistants were required to spend a minimum of 1 day as a note-taker before becoming an interviewer. The research assistants who did become interviewers also had additional qualifications, such as graduate level training and/or prior experience working with homeless populations.
While obtaining informed consent at the beginning, participants were told that the researchers’ interest pertained to their health care access. The interviews began with the general prompt, “tell me about yourself” to allow the participant to direct the conversation more broadly. Throughout the interview researchers would raise topics for discussion, although not in any specific order. These topics included what the participant liked or did not like about their life, which agencies they accessed in town, how they described their physical and mental health, what they do when they are sick or hurt, what their last experience was like at the hospital, and what they would say to policy makers or “the people who make the rules.”
Supplementary data were also collected through chart reviews at 2 local hospitals, to obtain figures on how often acute care services were used by participants in 2018. All participants were asked for their permission, 52 gave consent and 1 declined. The lead author worked with trained research assistants to review the hospital charts.
Sample
Fifty-three individuals who self-identified as homeless or vulnerably housed were included in this study. Snowball sampling was used in 2 rural and semirural towns in Ontario in October and November 2018 to identify and recruit participants from a local emergency shelter, employment center, and government assistance location. All participants who were recruited chose to participate with no attrition. One participant declined to participate in the hospital chart audit that followed the interview. The sample consisted of 32 men and 21 women. The ages ranged from 17 to 66 years, with a mean age of 40 years (SD = 13.20). All participants were Canadian-born, with 24% identifying as having Indigenous ancestry.
The sample size was determined through consideration of Malterud et al’s proposed concept of information power, which requires that researchers pay attention to the dynamic interaction between 5 factors; these include the (a) aim of the study, (b) sample specificity, (c) use of established theory, (d) quality of dialogue, and (e) analysis strategy. 43 In general, fewer participants are needed when the study aim is narrow, the combination of participants is highly specific for the study aim, there exists established theory, the interview dialogue is strong, and the analysis includes narrative details.
We argue that the present sample of 53 is an appropriate mid-range size needed to obtain information power. The aim of the study was narrow—to understand how individuals who were homeless or vulnerably housed navigate the health care system. The sample specificity was dense, in that the participants were highly specific and met the criteria of self-identifying as being homeless or vulnerably housed. The project was informed by a body of theoretical literature on health, stigma, and discrimination1,29-31 and used a narrative interview method. Finally, the data underwent individual and cross-case analysis as detailed below.
Data Analysis
Analysis of the interviews followed Fraser’s narrative inquiry; in phase 2, the material was transcribed by the authors and in phase 3 the individual transcripts were interpreted. 38 The 2 authors and a qualified consultant independently listened to the audio while reading the transcripts and handwritten notes that were produced during the interviews. For each person interviewed, the coders created a document that detailed the key themes that emerged in their narratives. The coders conducted 3 at the beginning and confirmed they were using the same process. The coders worked independently and did not share their interpretations of key themes during this phase.
To complete phase 4, scanning across different domains of experience, 38 each of the coders independently created a spreadsheet that identified the key themes they found and noted in which interviews they were present. These documents served to highlight how interpersonal experiences had shared or different meanings across participant narratives. In phase 5, linking the personal with the political, and phase 6, looking for commonalities and differences among participants, 38 the coders met in person to review their interpretations of the individual interviews and the overall themes that emerged across them. The coders held a 2-day meeting that began by listing all themes that emerged on a large whiteboard and then discussing and sorting them into major themes and sub-themes until consensus was reached. It should be noted that interrater reliability was not assessed, such as through calculation of the Cohen kappa statistic, because narrative inquiry is intended to produce a nuanced meaning and interpretation of the data. Fraser notes that rather than producing “the right” knowledge, narrative research is done with an understanding there are multiple possibilities for representing stories. 38 To this end, the authors held a subsequent workshop with interview participants following the 2-day coding meeting to review the key themes that emerged and receive confirmation that the material presented was an accurate representation.
The hospital records were reviewed onsite at the hospitals using patient e-records accessed through Medipatient and Saluvision. Patients were identified using first and last name and date of birth. The researchers collected visit history information on each participant for the year 2018. Records in each system were reviewed collecting information on type of visit (ED, outpatient, and inpatient), general reason for visit, identified address, time to physician in attendance (PIA), identified Canadian Triage Acuity Scale (CTAS) number, and discharge disposition/instructions/referrals. Researchers documented visit history information chronologically for each participant and data from the 2 systems were compared.
Ethics
Participants received a $20 gift card to 1 of 2 large retailers as remuneration. The study was approved by the authors’ institutional Research Ethics Review Board on August 28, 2018 (file #3315) and the hospitals where data collection occurred gave consent following written confirmation of the university’s approval.
Results
Health Care Services Accessed
Interview data indicated 28% of participants had a local primary care physician or nurse practitioner, 40% had a primary provider in another city (7.5% <30-minute drive, 9% 30- to 60-minute drive, 23% <60-minute drive). An additional 32% had no primary care physician or nurse practitioner of record.
Hospital chart reviews indicated that 28 (54%) of the 52 participants who gave consent had a visit in 2018. These 28 individuals had 76 visits collectively for medical (60 = 79%), mental health (13 = 17%), and dental (3 = 4%) reasons. Of the 28 individuals who had emergency department visits in 2018, 8 were frequent users, 2 of whom were particularly high users (with 15 and 28 visits, respectively). These 8 frequent users in 2018 represent 15% of the 52 participants who gave consent to review their records; collectively they had 34 of the total visits for medical issues (including 14 for pain), 10 visits for mental health (such as anxiety and situational crisis), 12 visits for drug-related issues (including withdrawal and cellulitis at the injection site), and 1 visit for dental reasons. Collectively this represents 57 hospital visits in 2018, which indicates these 8 individuals (15% of all participants) produced 75% of the hospital visits in 2018.
Perceptions of Clinician Bias
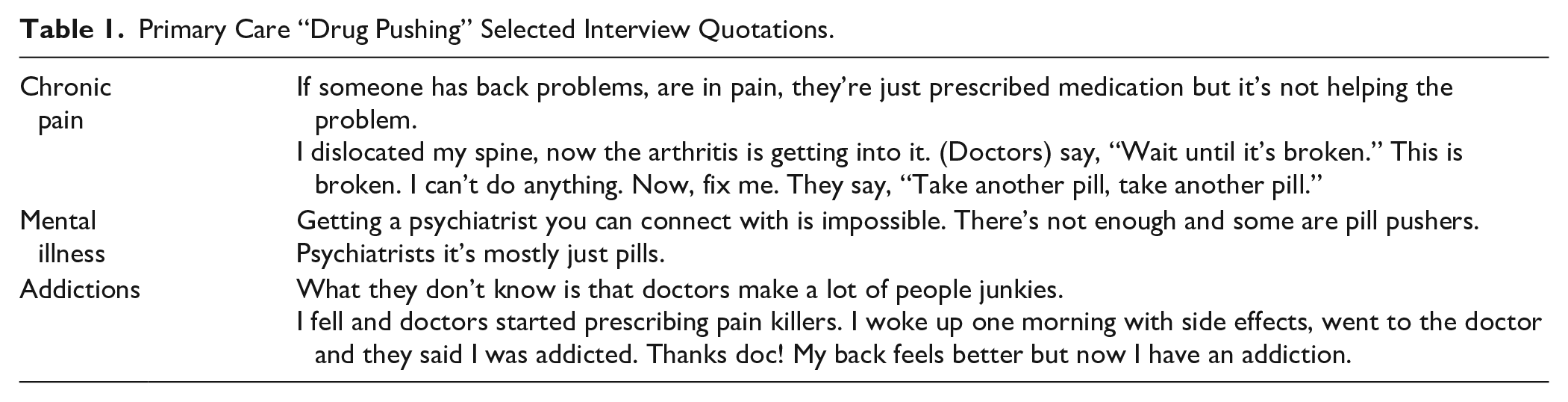
When seeking primary care treatment for chronic pain, mental illness, and/or addiction-related issues participants felt there was an overemphasis on prescribing medication over other forms of treatment (Table 1).
Primary Care “Drug Pushing” Selected Interview Quotations.
In acute care settings, participants felt that clinicians perceived them to be drug-seekers, particularly when seeking treatment for chronic pain, mental illness, and/or addiction-related issues (Table 2).
Acute Care Perceived “Drug Seeking” Selected Interview Quotations.

In primary emergency care settings participants felt they received selective care for physical conditions, including chronic pain, mental illness, and addiction-related issues. They reported receiving poor-quality care and sometimes were denied care entirely based on discriminatory practices (Table 3).
Primary and Acute Selective Care Provision Interview Quotes.

Discussion
Stigma and discrimination have implications for the health of those experiencing social inequities.1-3 Homeless individuals are one socially disadvantaged population who report high rates of substance addiction, mental illness, and chronic pain.5-7,14 Notably, the problems that homeless individuals commonly identify—addiction, mental illness, and chronic pain—were also the issues participants in this study felt were the most underserved in primary and emergency care settings. At the primary level when seeking care for one or more of these 3 issues, participants expressed the views that clinicians overrelied on prescribing medication without considering alternatives or the potential consequences of addiction. Conversely, when seeking care for one or more of these three issues through emergency care, participants felt judged and stigmatized, with clinicians assuming they were seeking out prescriptions for narcotics.
Research has shown that patients in general report suboptimal interactions when seeking care for chronic pain.34,35 The high incidence of multiple morbidities amongst homeless patients 7 such as addictions, chronic pain, and mental illness may result in poorer care provision for this population. While this research shows participants require on-going pain management, being labeled as “drug seekers” may lead clinicians to take a conservative approach 14 with potentially less-effective outcomes for these already vulnerable patients.
Reports of primary care access were low in this study when compared to previous Canadian estimates that suggested between 43% 18 and 56% 14 of homeless individuals have a regular primary care provider. The present study increases understanding of health care access by asking participants not only whether they had a regular primary care provider, but where they were located geographically. When location is considered, only 28% had a provider in their town. Lack of access to primary care providers is a pressing issue and may partly contribute to the high rates of ED usage among homeless persons.15,21,25 Particularly in rural and semirural towns where public transit is not available or is limited, such as in this study, travel outside of town requires access to a vehicle or a supportive friend who will drive; these types of resources may be less accessible for individuals experiencing homelessness. Within the present research, 15% were identified as frequent ED users who accounted for 75% of hospital visits in the year the study was conducted, primarily for comorbid conditions and chronic pain. The recurring visits suggest that these issues are not currently being well addressed. Increasing access to primary care providers for individuals experiencing homelessness could improve consistency of treatments for mental illness, chronic pain, and addictions while reducing ED visits.
Additional considerations are needed to tailor approaches to health care such that they are accessible to this marginalized population. Within this study participants expressed a sense that they were provided poor-quality or selective care at the primary, emergency and acute levels, based on discrimination of their housing status. At the organizational level, health care delivery systems tailored to meet the needs of the homeless have been found to be the most successful in improving primary care access for this population. 44 Some promising recent approaches focus on social determinants of health screening 45 and the colocation of services that offer medical and social care, 46 such as a homeless-tailored primary care clinic and ED 47 and nurse-led primary health clinic and men’s shelter. 7 Organizations that have reported success integrating care services share the traits of prioritizing vulnerable populations, extensive community collaboration, team approaches, diversified funding, and being data driven. 48
Limitations
This study does not represent a statistically significant sample. Interview data were collected through self-report and not externally validated. Hospital records were reviewed for visit history but did not include a review of clinical or diagnostic notations. This study focused on the views of persons experiencing homelessness and no clinician perspectives were sought.
Conclusion
Health care for homeless patients could be improved by increasing access to primary care services that are geographically accessible and nonstigmatizing. Tailored treatment is particularly needed for chronic pain, mental illness, and substance addictions, which are the most commonly identified health issues and also the areas where homeless individuals identify suboptimal care. Increasing access to primary care in the community could improve the quality of health of this population, and decrease hospital visits, but must be done in a way that respects the unique needs of this patient population.
Footnotes
Acknowledgements
The authors would like to thank Shannon Culkeen, Chloe Devlin, Lucas French, Suzanne Galloway, Carlee Giffen, Brandon Gonsalves, Rachel Loveless, Melanie Lusted, and Madeline Porter for their research assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was generously funded by the Central East Local Health Integration Network (CELHIN-TrentU_MOU_10.30.2018_03.31.2019) and the Corporation of the City of Kawartha Lakes (CKL-TrentU_MOU_09.04.2018_08.01.2019).