
Abstract
Cervical cancer disparities persist in the United States despite the availability of the well-established screening test, the cervical cytology, and resultant prevention and early treatment of precancerous lesions. Women of racial and ethnic minorities suffer the highest incidence rates in the United States, and therefore bear a disproportionate burden of the disease. 1 Indeed, mortality from cervical cancer among African American women is almost twice that among White women. 1 Persistent infection with oncogenic strains of human papillomavirus (HPV) plays a major role in the development of cervical cancer, and the prevalence of HPV infection is highest among women with minority race/ethnicity, low education, and low income.2-5 Although the recent availability of the HPV vaccine has the potential to lower the rates of HPV infection, 6 the uptake of HPV vaccination remains low. 7
There are about 55 million cervical cytology tests performed each year in the United States, mainly in primary care settings. Approximately 3.5 million (~6.4%) are abnormal and require medical follow-up,8-12 which generally entails colposcopy (ie, microscopic evaluation of the cervix) and biopsy of suspicious areas. 13 Although cervical cancer is preventable, adherence to colposcopy and follow-up recommendations is less than optimal, with the lowest adherence rates occurring among low-income, inner-city African American women,14-19 generally in the 30% to 40% range,19-24 as well as among women who are younger and less educated.25,26 These populations not only experience access barriers (eg, insurance, language, place of residence) but also psychosocial barriers (eg, low knowledge and high anxiety) that undermine adherence.18,19,27-32
Despite the fact that adherence remains a persistent problem, only a few studies have focused on psychosocial barriers to follow-up testing and management after an abnormal cytology result, particularly in the most vulnerable populations.19,30,33,34 This study builds on previous work19,30 to provide a more comprehensive and systematic assessment of barriers in an inner-city, underserved population, guided by the Cognitive-Social Health Information Processing (C-SHIP) model,19,30,35-37 which highlights 5 cognitive–affective constructs that can undermine adherence (ie, cancer-risk knowledge and perceptions, cancer-risk beliefs and expectancies, cancer-risk distress, cancer-risk goals and values, and cancer-risk coping skills).19,30,35-37 In the current study, we addressed 2 research issues among underserved women scheduled for an initial colposcopy: (a) to delineate the profile of cognitive–affective barriers of an inner-city, predominantly African American population and (b) to describe the relations between these barriers and sociodemographic factors to identify strategies to improve follow-up adherence for use in the primary care setting.
Methods
This is a cross-sectional, correlational study that assessed barriers to follow-up adherence among low-income, minority women, who were notified of an abnormal cytological test result and received a scheduled colposcopy appointment. This design was chosen in order to assess psychosocial barriers and their sociodemographic correlates prior to the actual follow-up appointment to capture women during the anticipatory phase of feedback impact. The data for this study were collected as part of a precolposcopy baseline assessment for a larger parent study, which is a randomized controlled trial that evaluated the efficacy of a tailored, telephone-delivered barriers counseling intervention program in the colposcopy clinic (National Institutes of Health Grant R01 CA104979; Suzanne M. Miller, Principal Investigator). For ease of communication, the parent study design and outcomes are reported in another article. 38 The study was approved by the institutional review boards of Fox Chase Cancer Center (FCCC) and Temple University Hospital (TUH).
Participants
Patients who were scheduled for an initial colposcopy were recruited from the Temple University School of Medicine Women’s Care Center Colposcopy Clinic in North Philadelphia, Pennsylvania, which serves a predominately low-income African-American population, from May 2006 to June 2010. The final sample size was 210.
Procedure
Patients with an initial abnormal cervical cytology test result were mailed a notification letter informing them of their result and the need to follow-up with a diagnostic colposcopy, a scheduled appointment date, and colposcopy clinic contact phone numbers. The TUH research nurse reviewed the Colposcopy Clinic schedules and identified eligible patients. Approximately 2 to 4 weeks before the initial colposcopy appointment, eligible patients (N = 343, 100%) were contacted by the TUH research nurse by telephone. On contact, the patient’s upcoming colposcopy appointment was confirmed and the research nurse informed the patient about the study opportunity and invited her to be transferred to a FCCC study staff to learn more. Patients who provided verbal HIPAA (Health Insurance Portability and Accountability Act) authorization and informed consent were then telephonically transferred to an FCCC study staff member.
For patients who were transferred, study staff provided further information about the study and confirmed verbal consent. Verbally consenting participants (N = 324, 94.5%) were administered the demographic and barriers assessments, and were sent a written informed consent document in the mail for them to sign and return in a prestamped envelope. Although the barriers assessment was administered to all verbally consented participants, only those who returned the written consent form were included in the final sample (N = 210, 61.2%).
Measures
Sociodemographic Assessment
Variables assessed included age, race/ethnicity, level of education, marital status, and employment status. The sociodemographic characteristics of the study sample (N = 210) are presented in Table 1.
Baseline Demographic Characteristics of the Total Sample (N = 210).

Psychosocial Barriers Assessment
The barriers assessment instrument used in the current study was developed from our prior work,19,30 formative evaluation, and our guiding theory. Participants were asked about the 5 categories of psychosocial barriers on a Likert-type scale of 1 = not at all, 2 = slightly, 3 = somewhat, 4 = very much, and 5 = extremely. The Likert-type scale rating format was used to capture the extent to which a given barrier was operative, in order to increase the rigor of the results and their application to intervention. All items were scored in the direction that higher ratings indicated greater barriers. Reverse-scored items are indicated with an “R” below. A rating of 3 or higher was considered endorsing the item as a barrier to adherence. The 5 psychosocial barrier categories posited by the C-SHIP model were operationalized into the following:
Knowledge/risk perceptions: Three items assessed how well the participant understood (1) the meaning of an abnormal Pap smear [R]; (2) what a colposcopic examination includes [R]; and (3) what the human papilloma virus (HPV) is and its link to cervical cancer [R].
Expectancies and beliefs: Five items assessed the participant’s extent of beliefs in (1) having an abnormal Pap smear means having cancer; (2) having a colposcopy will be helpful [R]; (3) there is nothing that can be done that would change whether or not she gets cancer; (4) being able to keep her colposcopy appointment [R]; and (5) being able to follow what the doctor tells her to do after the colposcopy [R].
Distress: Five items assessed the participant’s worry about (1) the possibility of having cancer; (2) having pain or discomfort from the colposcopy or biopsy; (3) treatments that might be needed after colposcopy; (4) sexual problems after colposcopy; and (5) transmitting the virus that causes cancer to sexual partners.
Values and goals: Five items assessed the importance to the participant of (1) keeping the colposcopy appointment and following through with the doctor’s medical management recommendations [R]; (2) keeping a good body image and feeling good about herself [R]; (3) [if age appropriate] being able to become pregnant [R]; (4) being able to have a healthy sex life [R]; and (5) not being embarrassed or feeling ashamed during the colposcopy appointment.
Coping skills: Five items assessed whether the participant had ways to manage the following challenges: (1) distress associated with the appointment [R]; (2) paying the co-pay for the colposcopy appointment and getting referral letters that might be needed for insurance [R]; (3) remembering the appointment [R]; (4) managing responsibilities such as getting childcare, eldercare, and coverage at work [R]; and (5) ability to get transportation.
Results
The final study sample characteristics are presented in Table 1. More than half of the participants had completed education of high school, trade school, or GED (General Education Development) or below (n = 122, 58.65%). The majority were single, never married (n = 136, 67.33%), and a significant subset were unemployed (n = 76, 36.36%). Some participants did not provide complete demographic information; therefore, the numbers of the demographic groups are smaller than the total sample size. Women who had high school completion or below were more likely to be unemployed (P < .0001).
Regarding barriers to adherence, the frequencies and mean ratings of the barrier categories are displayed in Table 2. Overall, 81.43% of study participants reported having at least one barrier to adherence, and almost half (45.71%) endorsed 2 or more barriers.
Descriptive Statistics of Barriers Ratings by Cognitive-Social Health Information Processing (C-SHIP) Constructs (N = 210).

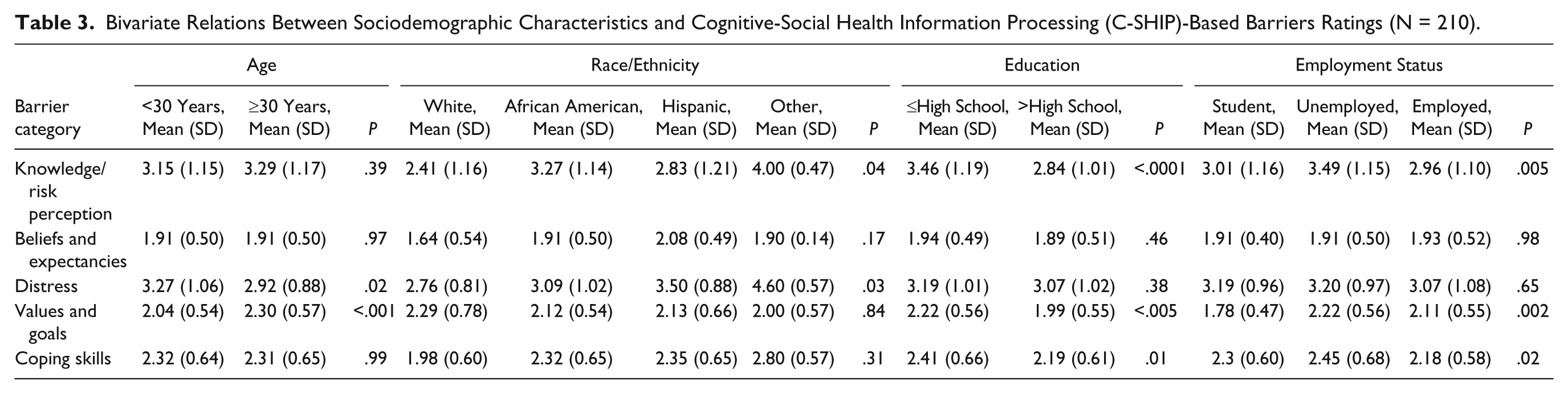
In examining the sociodemographic correlates to each C-SHIP barrier category, we focused on those correlating with the knowledge, distress, and coping skills barriers because they were the most frequently endorsed and had the highest mean ratings. Bivariate relations between sociodemographic characteristics and barrier category ratings are presented in Table 3. Women with less education (high school completion or below) reported significantly higher knowledge (P < .0001) and coping barriers (P < .05). Women who were unemployed also reported higher ratings of knowledge (P < .01) and coping (P < .05). Women who were younger than 30 years reported significantly higher distress barriers (P < .05). Please see Table 4 for a summary of major findings of this study.
Bivariate Relations Between Sociodemographic Characteristics and Cognitive-Social Health Information Processing (C-SHIP)-Based Barriers Ratings (N = 210).
Summary of Major Findings (N = 210).

Discussion
Although cervical cancer is highly preventable, inner-city, low-income minority women continue to be at higher risk for the disease, due to disparities in adherence to follow-up regimens after an abnormal cervical cytology result.14-19,39,40 Building on existing literature and theory, this study delineated the psychosocial barriers to adherence, and their sociodemographic correlates, in an underserved population. The study sample had a large proportion of African Americans (82.2%), who are at the highest risk of cervical cancer morbidity and mortality1-5,41 and have been found to have the lowest adherence rates to follow-up care after an abnormal cervical cytology.14-19 Educational level and employment status were representative of a low socioeconomic status sample, who suffers the greatest disparities in health care access and uptake.
We found that knowledge and distress barriers were the most frequently endorsed, suggesting that these factors require attention among this vulnerable population. Of interest, coping barriers also characterized a significant proportion of the participants. Even within this underserved group, less education, being unemployed, and age younger than 30 years were associated with greater adherence barriers. Less educated and unemployed women may not have sufficient cognitive or material resources to understand their cervical cancer risk and follow through with adaptive actions. Younger women may also be emotionally less able to manage the worries and distress associated with cervical cancer risk and related diagnostic/treatment procedures.
The results show that cognitive–affective barriers vary by individual characteristics, and hence it is important to develop personalized interventions to assess and address barriers that are most relevant to the individual. Theory-based barriers assessment is a critical first step for identifying women who are at high risk for nonadherence, followed by delivering tailored counseling messages. This process can be facilitated by employing refined barriers assessment instruments, such as the one used in the current study, which offer advantages in terms of precision and sophistication of tailoring algorithms for specific individuals. As knowledge barriers are the most commonly endorsed, it would be worthwhile to explore whether a protocol for assessing and addressing barriers could be integrated within primary care services. Primary care staff who communicate with patients about the feedback of test results, and/or who prepare patients for the receipt of test results, could reinforce educational messages in a supportive fashion and provide referrals to community navigators, colposcopy clinic support services, and other resources.
In addition, based on best practice principles in health communication,42,43 the messages delivered to patients need to be carefully crafted for low health literacy levels to maximize understanding of the meaning and personal relevance of an abnormal cervical cytology result. Patients would also seem to benefit from messages that correct unrealistic fears and worries about disease and diagnostic/treatment procedures, especially since follow-up regimens require sustained adherence over time. Finally, given the importance of coping skills for enabling the patient to manage distress, distress management skills and reinforcement for adherence behaviors should be components of a comprehensive approach to barriers reduction.
While telephone-based intervention has been shown to be efficacious in the colposcopy clinic,19,30 it can be time and service provider intensive. Focusing on the most common barriers at the time of feedback in a protocolized and automated fashion should refine and streamline the process and better prepare patients. Furthermore, there is growing evidence supporting the role of patient navigators in addressing barriers and promoting adherence to abnormal follow-up in underserved patient populations, such as the Screening Adherence Follow-Up (SAFe) program for Latino women 39 and other patient navigation programs.34,44-49 Embedding state-of-the-science psychosocial barriers counseling into clinical- and community-based patient navigation programs may work synergistically to address cognitive–affective and access barriers.50,51 This integrated approach has high potential to improve adherence to follow-up among inner-city, minority women, and hence reduce cervical cancer disparities. In future research, it will be important to replicate these findings with a larger and more culturally diverse underserved sample. Furthermore, it will also be important to link reported patterns of barriers with adherence outcomes, particularly over time.
Footnotes
Acknowledgements
We also thank Mary Anne Ryan and Gem Roy for their technical assistance on this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Institutes of Health grants, R01 CA104979, RC1 CA145063, R01 CA076644, R01 HG01766, Department of Defense grant DAMD17-01-1-0238, American Cancer Society grant TURGS-02227, and the Fox Chase Cancer Center Behavioral Research Core Facility P30-CA06927 to Dr Miller.