
Abstract
Objectives:
This article describes the learnings from the pilot phase of the Healthy Life Trajectories Initiative, a preconception health trial for 18- to 25-year-old women in Soweto, South Africa.
Methods:
The study compares two arms focussed on either physical and mental health (intervention; delivered by community health workers – ‘Health Helpers’) or standard of care plus (control; standard access to healthcare plus additional telephonic input on ‘life skills’; delivered by call centre assistants). These are collectively referred to as Bukhali. Data on the pilot implementation of the Bukhali trial (n = 1655) were collected from (1) weekly team meetings, (2) two focus groups (one with the intervention team Health Helpers, n = 7; one with intervention participants, n = 8) and one paired interview with control call centre assistants (n = 2), (3) notes from eight debrief sessions with Health Helpers and (4) quantitative trial monitoring data. Qualitative data were thematically analysed.
Results:
The findings clustered within three themes: (1) challenges for young women in Soweto, (2) priorities for young women in Soweto and (3) implementation challenges and perceptions of the intervention. Challenges were mostly related to tough socioeconomic circumstances and less prioritisation of living a healthier life. The priorities of employment and educational opportunities reflected the socioeconomic challenges, where health was not recognised as priority. The main challenge to participation and compliance with the trial was that young women in Soweto generally wanted a tangible and preferably financial and immediate benefit. Community peer sessions, despite being recommended by young women as part of the intervention development, were not successful. Many women also moved between multiple households within Soweto, which flagged concerns for a cluster trial and risk of contamination.
Conclusion:
Preconception health trials should consider socioeconomic challenges present in urban poor contexts. Learnings from the pilot phase significantly affected the design and implementation of the main Bukhali trial.
Keywords
Introduction
The importance of the preconception period is receiving greater recognition in global health.1–3 However, the promotion of preconception health in low- and middle-income countries (LMICs) is lagging. 4 Obesity is a particular concern for preconception health, since children of mothers who are obese before they become pregnant have a 26 times greater risk of becoming obese. 5 In South Africa (SA), an LMIC, the Birth to Twenty Plus cohort showed that by early adulthood, 47.5% of girls were either overweight or obese, 6 and that if a girl was obese by age 5 years, she had a 42 times greater risk of being an obese adult. 7 Findings from the Soweto First 1000 Days cohort reported that 67% of women presenting at their first antenatal clinic visit were either overweight or obese. 8 Concerns about obesity also extend to childhood in SA whereby one in four girls age 2 to 14 years, and one in six boys in the same age group, were either overweight or obese. 9
Given the public health distress around childhood obesity, the SA Medical Research Council, partnering with World Health Organization and the Canadian Institutes of Health Research, launched the Healthy Life Trajectories Initiative (HeLTI) in SA. This initiative aims to establish a programme of research to generate evidence that will inform national policy and decision making around preconception health as an intervention opportunity. This evidence focusses on optimising young women’s physical and mental health in order to establish healthier trajectories for themselves and future offspring, and to offset health risks, such as obesity. This programme is also being implemented in Canada, China and India. In SA, the trial is called Bukhali, which means smart/powerful in isiZulu (commonly spoken language in Soweto), with the catchphrase of ‘Living your best life’. The aim of this article is to describe the findings and learnings from the pilot implementation of the HeLTI trial in SA, including a description of intervention strategies and adaptations to the trial design.
Methods
Study setting
The HeLTI site in SA is Soweto, a predominantly low-income, peri-urban setting in Johannesburg with a population density of 6357 people per km2 according to SA’s most recent national census. 10 Although there is economic diversity in Soweto, poverty-related challenges are a reality, including unemployment and food insecurity, 11 and poor access to appropriate health services, especially for young people. 12 Preconception health promotion with young women in Soweto is imperative, since a third of them will have their first child by the time they are 19 years old. 13 Furthermore, there are multiple non-communicable disease risks for young women in Soweto – these include overweight and obesity, 7 poor diet,14–16 high sedentary behaviour17,18 and physical inactivity in late adolescence. 19 In addition, young women in Soweto face mental health challenges, such as anxiety and depression, 20 and HIV remains a complex issue for young people in Soweto, 12 with young women being particularly at risk of HIV infection.21,22 Given the evidence for the relationship between insufficient sleep and the risk of obesity, sleep is a health behaviour that was included in Bukhali trial.23,24
Qualitative formative research for HeLTI in Soweto highlighted a number of challenges for young women. These include difficulties around making healthy choices due to an unsupportive environment, 25 the need for mental health support and various social constraints such as challenges relating to social pressure and socioeconomic circumstances. An example of this is the pressure to succeed in school, particularly if the young woman is the first in her family to finish school and enrol in tertiary education. Socioeconomic challenges include food insecurity, unemployment and difficulty finding working. 26 Young women’s preferences for intervention were found to be mixed, but there was consistency in the preference for community health workers (CHWs) as the delivery agent. 26
Following expert consultations and formative work, the design of the Bukhali trial was conceptualised as a cluster randomised trial within 30 randomly defined geographical areas in Soweto. The primary aim of the trial is to evaluate the effect of a four-phase intervention, starting preconception, on the index child’s adiposity status at age 5 years as determined by fat mass index (fat mass/height) 2 derived from dual-energy X-ray absorptiometry. The two-arm randomised controlled trial (RCT) included a health component (intervention arm) and a standard of care plus component (control arm, standard access to healthcare plus additional input on ‘life skills’).
Trial protocol
Ethical approval for the trial was provided by the Human Research Ethics Committee (Medical) at the University of the Witwatersrand (Ref.: M1811111). Written informed consent is obtained from all participants. The trial is registered with the Pan African Clinical Trials Registry (https://pactr.samrc.ac.za; identifier: PACTR201903750173871). The trial is recruiting women age 18 to 25 years (n = 6800) from the Soweto Young Women’s Survey.
The intervention arm was designed to be delivered by CHWs (26–40 years old) who would (1) dispense multiple-micronutrient supplements and resource material, (2) provide health feedback (body mass index (BMI), blood pressure, anaemia and lifestyle) and free services (HIV and pregnancy testing) through monthly individual sessions and (3) facilitate monthly peer sessions on Saturdays. The stakeholder group of young women from Soweto asked that CHWs be termed ‘Health Helpers’ for the intervention. Health Helpers were required to have completed secondary school and have some tertiary training but were not required to have had any formal training as a CHW. Health Helpers received training in Healthy Conversation Skills (HCS) 27 as part of the recruitment process. HCS refresher sessions are held approximately every 12 to 16 weeks, and Health Helper HCS are reviewed by trainers. Once employed, Health Helpers received training to deliver the intervention.
The format of the individual sessions for the intervention clusters is provided in Table 1. The intention of these sessions was to provide additional support for behaviour change using HCS. Intervention content and training materials were designed with input from content experts, a specialised health curriculum developer and a graphic designer. Social learning theory concepts of knowing, doing and becoming were used in the materials. 28 Materials included a facilitators’ manual for Health Helpers and resource books for participants. The materials were designed for use in monthly peer sessions with approximately 15 women, facilitated by a Health Helper, over 18 months. Each peer session was intended to take place at a central community venue in each cluster. The details of these sessions are outlined in Table 2. Peer sessions were structured to encourage group discussion and also had take-home activities. Health Helpers follow up on the take-home activities. Since these are self-monitoring tools for the participants’ use as prompts for behaviour change (rather than research measures), the follow-up of these activities is not specifically monitored. The facilitator manual contained information about each of the health topics, and essential information was included in the participant resource book.
Individual session format for main intervention.
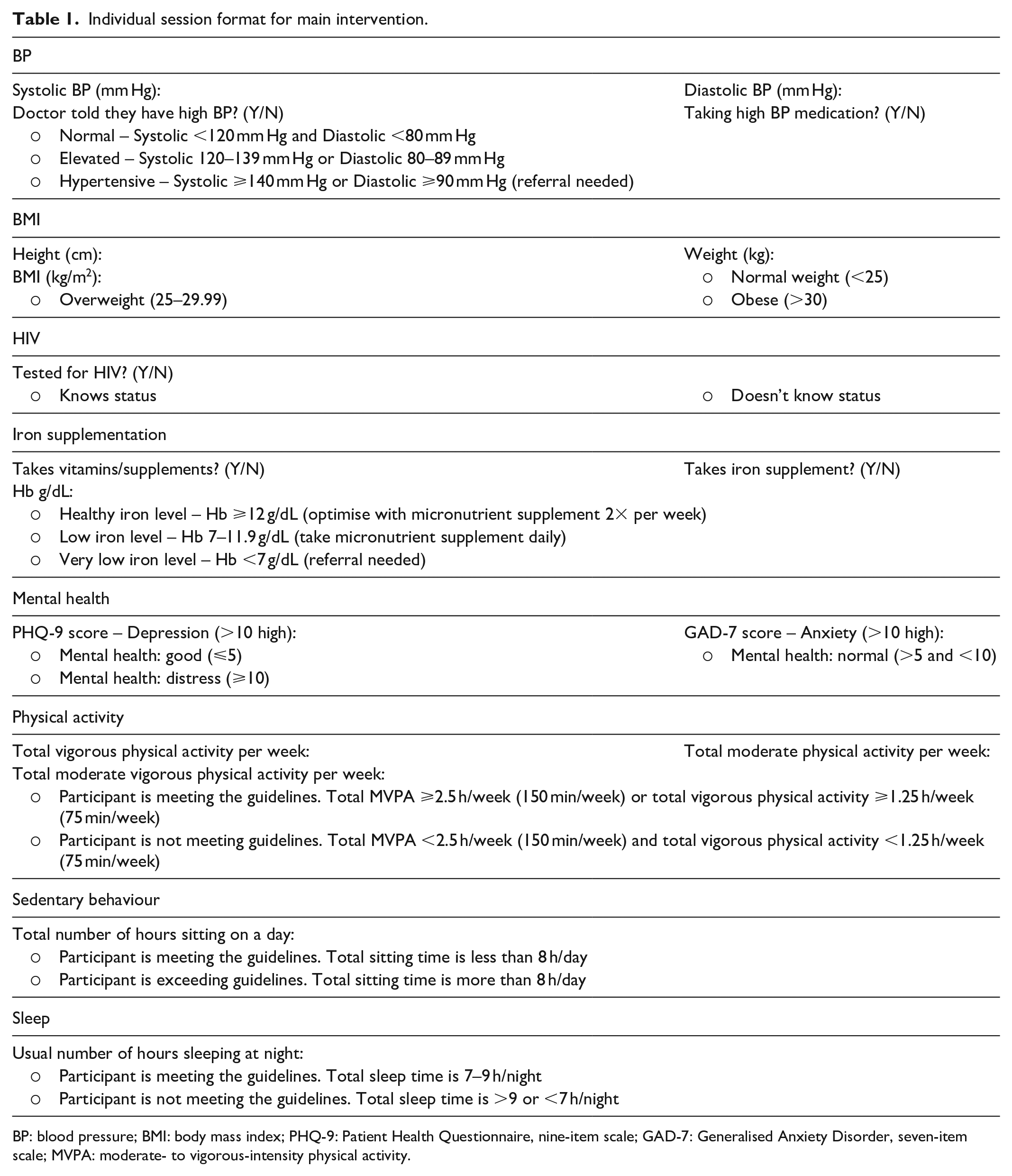
BP: blood pressure; BMI: body mass index; PHQ-9: Patient Health Questionnaire, nine-item scale; GAD-7: Generalised Anxiety Disorder, seven-item scale; MVPA: moderate- to vigorous-intensity physical activity.
Bukhali intervention session details.

NCDs: non-communicable diseases; BMI: body mass index; SA: South Africa.
If intervention participants become pregnant during this 18-month period, Health Helpers would deliver four individual sessions using material developed specifically for pregnancy: Bukhali Baby. This included a facilitators’ manual and resource book, which cover basic information about pregnancy, healthy eating and physical activity in pregnancy; preparing for delivery and baby; and pregnancy milestones. Participants would also receive a free sonography session and gestational diabetes screening. Individual support would continue post-delivery.
To partially control for special attention given to women in the intervention arm, the control arm had a dedicated call centre which contacted participants once a month and delivered a curriculum on ‘life skills’ (not directly relating to health) via telephone, SMS and email – the ‘plus’ component. This was in addition to standard access to healthcare (standard of care). Control participants also had access to free HIV and pregnancy testing at the research centre and were advised to contact their local health facility for any other health concerns.
Data collection
We piloted the intervention and control arms in six random community clusters (three intervention, three control) commencing in early 2019. Identification and recruitment of clusters will be described elsewhere. Briefly, an online search was performed using the Google search engine to locate the information of all churches in Soweto (used to differentiate communities). The latitude and longitude of the 104 churches identified and verified were then classified using k-means clustering in order to define 30 communities with a 1 km2 radius each. We piloted the intervention and control arms in six of these community clusters (three intervention, three control) commencing in early 2019.
A mixed methods approach was used. Data on the implementation of the pilot phase of Bukhali trial were collected from (1) weekly team meetings (meeting notes, between March and June 2019), (2) two focus groups (one with the intervention team Health Helpers, n = 7; one with intervention participants, n = 8) and one paired interview with the control call centre assistants (n = 2), (3) notes from eight debrief sessions with Health Helpers and (4) quantitative trial monitoring data extracted from the project’s REDCap database. 29
All Health Helpers and call centre assistants were included in the sample and were requested to participate in the focus groups and interviews via email. One of the call centre staff was not able to attend the interview due to being ill on the day of the interview. Intervention participants were purposively selected and contacted telephonically to request their participation in a focus group. The only criterion for inclusion (other than being an intervention participant) was their willingness to participate in a focus group. Two intervention participants did not arrive for the focus group due to unforeseen conflicting commitments on the day of the focus group. No repeat interviews were conducted, and given that no substantially new information was presented in the focus group with intervention participants (i.e. data saturation was reached), no further focus groups with intervention participants were planned.
The focus groups and interviews were conducted by author C.E.D. (MA, PhD), a female senior researcher with 20 years of experience doing qualitative research. C.E.D. had a prior working relationship with Health Helpers and call centre assistants, who were explained the reasons for doing the research. Although C.E.D. is the researcher responsible for overseeing the Health Helpers and call centre assistants, we believe that her experience with and insights into the intervention and control components of HeLTI (which also included the development of all intervention control materials and training of teams) outweighed the risk of any negative influence imposed on the focus group and interview process. C.E.D. had no prior relationship with intervention participants, and apart from explaining the reasons for doing the focus groups, and that C.E.D. is a researcher on the HeLTI team, no other information about C.E.D. was shared with intervention participants. C.E.D. has extensive experience working in cross-cultural settings, and has therefore had experience in navigating the cultural and socioeconomic differences between herself and the participants.
Each focus group or interview was approximately 1 h in length and took place at the South African Medical Research Council/Wits Developmental Pathways for Health Research Unit at Chris Hani Baragwanath Hospital in Soweto. These were audio recorded, with participants’ written consent, and were conducted primarily in English and transcribed verbatim (and translated into English if necessary). An individual also fluent in local vernacular languages was present for the focus groups and was able to translate where necessary. This individual along with the facilitator took notes during the focus groups and interviews. Transcripts were not returned to participants for comment and/or correction.
The discussion guide for Health Helpers and control team covered issues around recruitment (challenges, reasons for refusal, young women’s priorities, solutions to boost recruitment), and their perceptions of the intervention materials and delivery method. For intervention participants, the discussion guide covered their perceptions of life as a young woman in Soweto, their priorities, their perceptions of the intervention so far (including recruitment), their reasons for wanting to take part, their perceptions of others’ reasons for not wanting to take part and their suggestions for recruitment. Given the pilot nature of this study, the discussion guides were not pilot tested.
Analysis
Data were thematically analysed (manually using Microsoft Word, by C.E.D.) using a largely deductive approach. 30 The discussion guide formed the basis of an initial thematic framework, and this was further developed to encompass three main themes: (1) challenges for young women in Soweto, (2) priorities for young women in Soweto and (3) implementation challenges and perceptions of the intervention . After the initial stage of familiarisation with the data, codes were generated based on these themes, allowing subthemes to be formed. The next step involved searching for themes and subthemes in the transcripts, and continuously reviewing and refining subthemes. Once coded sections of text were summarised for each theme and subtheme, illustrative quotes for each theme and subtheme were extracted. The results of the analyses were not checked with participants.
Results
Challenges for young women in Soweto
It is clear from the data collected that young women in Soweto face numerous challenges (illustrative quotes in Table 3), relating mostly to their socioeconomic circumstances, and poverty and unemployment in particular. Intervention participants spoke of having limited opportunities for education and employment, which were made more stressful if they had children to care for. Within the context of these challenges, intervention participants spoke about young women in Soweto as having an ‘undisciplined’ lifestyle, and some were described as ‘lazy’.
Challenges for young women in Soweto.

Living a healthy life was described in all groups as difficult, particularly in relation to healthy eating and exercise opportunities. Intervention participants believed healthy food was expensive, inaccessible and often unappealing. Non-communicable diseases were acknowledged to be widespread, but these were considered the norm rather than something to be concerned about. Conversely, intervention participants perceived HIV/AIDS to still be a major issue.
Priorities for young women in Soweto
Not surprisingly, the priorities expressed by intervention participants were largely to do with employment and educational opportunities (illustrative quotes in Table 4). Health was not seen to be a priority by intervention participants, and this was also expressed by Health Helpers as part of their debrief sessions. However, views around certain health topics seemed to be mixed according to intervention participants. An example of this is pregnancy: some women are seen to prioritise their health when pregnant (for the sake of their baby), while others are willing to take risks during pregnancy (such as smoking or drinking alcohol) and were perhaps not informed about the consequences of these risks. These views reinforce the mind-set of ‘living for the now’ and not prioritising the future.
Priorities for young women in Soweto.

This was highly pervasive from the discussions and links to young women’s agency regarding their ability to influence their future. For some intervention participants, they vocalised that this mind-set came from their parents as a result of living tough lives. However, other participants spoke about changing this mind-set and breaking the cycle of poverty, and had aspirations to change things in their lives in order to affect the next generation. These responses indicate that Soweto is a diverse community in economic transition, described by one intervention participant as a ‘culture’ that is difficult to change.
Implementation challenges and perceptions of the intervention
Illustrative quotes for this theme are provided in Table 5.
Implementation challenges and perceptions of the intervention.

Incentives
There was a widespread view across the groups that participating in the trial (or any research) in Soweto must involve tangible benefits for young women. The most tangible benefit mentioned was money – the R150 (approximately US$10) that women receive to cover their transport costs when they come to the research centre in Soweto for surveys and assessments. The intervention was intended to be conducted in participants’ homes and neighbourhoods; it was not believed to be necessary to provide transport reimbursement when transport would not be required. This, however, was not the view of study participants, and the R150 turned out to be the only tangible benefit that could be provided in exchange for participation, even when the empowerment aspects of the intervention were emphasised. Knowledge about health, awareness of one’s own health status or an improvement in health status were not perceived to be a sufficient benefit for young women in Soweto. Participating in research for the improvement of their own health was not a widely held motivator.
Health awareness and testing
Participants acknowledged that receiving information about their own health was useful. They were concerned about HIV self-testing as it theoretically does not require pre- and post-test counselling, and the anticipated trauma of receiving a positive result was perceived as a barrier to uptake. However, participants acknowledged that even counselling does little to lessen the blow of knowing one is HIV positive. A further complication was the perception of weight loss being linked to being HIV positive, which presents challenges for a trial that is promoting healthy weight. With regard to the free pregnancy tests, Health Helpers reported that some participants stated that these were viewed with the same scepticism as HIV tests, while others liked the opportunity to test. Some participants reported to be more afraid of being pregnant than having HIV (and hence not wanting to take a pregnancy test), and yet did not seem to feel empowered to make their own choices about contraception use.
Cluster contamination
A critical finding was that, according to trial monitoring data, 23% of participants in the pilot study migrated across several households during the pilot intervention period, which was reported as a strategy to share resources across family–friends–partner households. In most cases, these households were outside of the cluster within which the women had initially been recruited. It was reported by Health Helpers that in many cases, family members did not know where the young women had moved to or when they were coming back, and did not seem particularly concerned about finding out where they were.
Education material and peer sessions
Despite the need for financial benefit, intervention participants felt that the materials were appropriate for young women in Soweto and found them to be helpful and educational. Health Helpers also indicated that the resource book provided a good starting point for conversations with young women. Although the peer sessions (originally intended to take place on Saturdays) proved not to be feasible for the majority of intervention participants, these sessions were appreciated by those participants who did attend. One of the reasons given by the Health Helpers for the peer sessions proving not to be feasible was the co-occurrence of other community activities taking place on Saturdays, such as social grant pay-out days and funerals. A reason given for funerals being prioritised was the fact that free food was provided. Even after providing refreshments and shifting to offer multiple sessions per day and multiple Saturdays per month in close proximity, the peer sessions were still poorly attended. It was the perceptions of the Health Helpers that poverty and the difficulty to prioritise peer sessions exacerbated the challenges experienced with intervention implementation.
HCS
Health Helpers’ impressions about the use of HCS was that these were sometimes difficult to implement in African languages that they used with participants. In particular, the HCS approach promotes the use of ‘Open Discovery Questions’ which start with ‘what’ or ‘how’, which comes across as ‘rude’ in some South African languages. The HCS approach supports individuals in finding their own solutions (as opposed to being told what to change). However, Health Helpers mentioned that some participants preferred just having solutions given to them, that participants differed greatly in their willingness to talk and some participants were not willing to engage at a level that would help them identify solutions for themselves. Related to this, setting goals for health behaviour change (a key component of the HCS approach) was not viewed as a priority, which aligns with the lack of prioritisation of health itself. Health Helpers also raised the question of whether listening to (and not necessarily counselling) participants was enough in a setting like Soweto given the contextual challenges mentioned earlier. They pointed out that many participants wanted to talk about other problems that did not necessarily directly relate to health.
Micronutrient supplement
The mobility of study participants within Soweto and the difficulty of meeting up with the participant made it difficult to physically give the supplements to participants, and so supplements were left with another household member if the participant was not home at the time. Some participants were sceptical about the supplements, expressing concerns about whether the supplements would cause them to become pregnant.
Control arm
The monthly telephonic contact was mostly well received, particularly since it was not demanding of participants’ time, and was not perceived to be too frequent. Topics that dealt with economic challenges, such as job readiness, were appreciated by control participants. Given the prevalence of these young women’s social challenges, call centre team members mentioned that it was difficult to stay within the scope of the topic for the month, and not discuss the other challenges that participants were facing.
Discussion
This article highlights the value of piloting complex interventions and presents preliminary findings from a novel preconception health trial in Soweto. This is a setting with numerous challenges for young women, which influence their priorities and willingness to participate in intervention activities. The findings of this pilot confirm the challenges mentioned in the formative research in this setting regarding healthy choices 25 and the need for social support. 26 The most striking finding was the difficulty in successfully administering peer sessions despite success in other settings and interventions.
There are limited preconception health trials in LMICs, and few reflect on the challenges around trial study design and implementation. Of those that are published, similar and context-specific challenges have been reported. These findings have implications for the implementation of preconception health interventions in LMICs. A preconception trial being implemented in Tajikistan, Bolivia and Palestine using mobile technology to reduce unintended pregnancies 31 found that short text messaging was the preferred method for communicating intervention content. A community-based lifestyle intervention with 18- to 59-year-old women in their homes in Malaysia also experienced potential contamination between intervention arms due to the community setting. 32 Another CHW-delivered trial in Malaysia has experienced similar challenges to HeLTI with scheduling intervention sessions and low interest in the pilot stage of their trial. 33 A preconception calcium supplementation for the prevention of preeclampsia implemented in SA, Zimbabwe and Argentina experienced significant difficulties and delays with recruitment due to inadequate medical records, redundant patient contact details and delayed pre-pregnancy hospital visits. 34
Despite the low prioritisation of health by young women as part of the HeLTI trial, the health status of women in Soweto warrants intervention, especially given the overburdened health system in settings like Soweto. Future research on preconception health trials in LMICs should consider as part of the intervention development and piloting: (1) identify the best approach to position crucial health messages for young women and engage with them and their community, (2) education material is appreciated when health literacy levels are low, (3) carefully consider study design (cluster versus individual randomisation), (4) understand that even best practice from successful interventions may not always translate in all settings and (5) preconception health messages may need to be embedded in intervention content that primarily focusses on other salient issues for young women, such as job readiness, entrepreneurship skills and educational attainment.
Adaptations to the HeLTI study design
Based on the findings from this pilot phase, there have been numerous changes made to the trial. Recruitment is still happening at community level, but randomisation is at the individual level, rather than by cluster. The intervention group will no longer receive peer sessions but will have strengthened monthly face-to-face or telephonic contact with their Health Helper. Specific adaptations include the following: (1) A social messaging community campaign has also been launched as part of HeLTI in Soweto so as to address health literacy, issues around values and priorities of young women and sensitising the importance of preconception health through linkages with priorities of young women; (2) health awareness results are provided after randomisation following baseline assessments on the same day (immediate feedback and commencement with either intervention or standard of care plus protocol); (3) all HIV testing (in person with Health Helper or self-testing) comes with pre-counselling and post-test counselling follow-up, with linkages to further support within the community and to health services; (4) transport costs are reimbursed for all research centre visits, and token incentives will be provided as the participant progresses to offset economic barriers and improve motivation (e.g. participants will also be able to request help with printing their resume to address the unemployment challenges mentioned); (5) the education material originally intended for peer sessions will be provided during the individual face-to-face sessions for the young women to work through the modules, and questions arising from this will be given time during the monthly follow-up sessions; (6) the HCS approach has been modified to allow time to build rapport before commencing, in so doing minimising the perception of rudeness, and increasing sensitivity relating to non-health-related goals while finding ways to weave in health prioritisation; and (7) a driver has been appointed to assist with the delivery of the micronutrient supplements to participants at their homes, and follow-up SMS supportive texts are sent to encourage compliance.
The location of this trial being limited to one particular setting in SA, the analysis of the data by one author and the small sample size could be perceived as limitations of this study. However, the contextual complexities of Soweto presented in this article suggest that this focussed approach allows the research team to become fully immersed in the development, implementation and evaluation of a contextually relevant intervention that has the potential to be scalable. The use of focus groups, a paired interview and debrief notes as data sources strengthens this study, in spite of the small sample size. Furthermore, this article represents the initial stage of evaluating the implementation of the Bukhali trial, which is ongoing and is informed by the UK Medical Research Council guidance on process evaluation. 35
Conclusion
In conclusion, complex interventions in poor communities are challenging, and there is a need for greater process evaluation before and during a trial, and flexibility in study design allowing for adaptation to improve the approach as new information is attained. This combination of evaluation and adaptability may ensure greater acceptability, feasibility and impact on the primary and secondary outcomes of a trial.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Beverly Draper and ITL Communication & Design for the development and production of the intervention materials, along with the Healthy Life Trajectories Initiative (HeLTI) intervention team for their role in the implementation of the trial.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the South African Medical Research Council and the Canadian Institutes of Health Research.
Ethical approval
Ethical approval for this study was obtained from the Human Research Ethics Committee (Medical) at the University of the Witwatersrand (Ref.: M1811111).
Informed consent
Written informed consent was obtained from all subjects before the study.