
Abstract
Introduction
The patient-centered medical home (PCMH) ideally tailors and individualizes health care services to patient needs by increasing access and managing all aspects of care, and through a team-based approach that is led by the patient’s personal physician. 1 Members of the care team may include medical subspecialists, pharmacists, nonprofessional peer supporters, nurses, family members, and care managers. 2 Care managers are playing an increasingly major role in the redesign of primary care and in the evolution of PCMH by providing patient education in disease self-management skills, coordinating services across a continuum of care providers, and linking patients to community and social services. 3 Although care managers have been referred to in various ways, such as navigators, coaches, or care coordinators, 3 they are generally considered to be licensed health care professionals who have direct contact with patients and facilitate and coordinate health care services across providers, settings, and conditions. 3 In contrast, case management typically involves discrete episodes of care and may not involve direct interactions with patients. 4
Care managers are usually nurses, social workers, or other professionals who work with PCMHs and other health care units to extend organizational reach and capacity.1,3 These individuals often serve as liaisons between health care providers, patients, and ancillary care services. They have a variety of responsibilities including engaging patients in care planning, care transition coordination, facilitating referrals to health care resources, and linkages to community-based organizations. 5 Despite the benefits of care managers, their adoption within PCMHs and the day-to-day practice of primary care remains uneven and approaches for implementation into workflows have been minimally reported or evaluated.6-9 This case study describes an implementation strategy for incorporating care management into the operations of a family medicine center and assesses the preliminary effectiveness of this approach.
Methods
Setting and Participants
The setting was University of North Carolina at Chapel Hill Family Medicine Center (FMC), which is the largest primary care unit within the UNC Health Care System (UNCHCS). The FMC is currently the clinical setting for 40 faculty members and 26 resident physicians, caring for a population of approximately 17 800 patients that have more than 55 600 outpatient visits per year. The demographic breakdown of the patient population is approximately 57% Caucasian, 29% African American, 4% Hispanic, and 4% Asian. Approximately 13% of patients have Medicaid as their primary insurance and another 13% are uninsured.
The FMC is a level 3 Patient-Centered Medical Home by the National Committee for Quality Assurance. On-site services include preventive and well care for all ages, same-day urgent care, chronic illness care, sports medicine, patient education, such as diabetes and smoking cessation, minor surgery (dermatological procedures, colposcopy, vasectomy, etc), acupuncture, and physical therapy. Patient care is supported by approximately 40 clerical/administrative and clinical support staff (nurses and medical assistants), plus security and financial counselors.
Implementation Strategy
We used an organizational model of innovation implementation to guide the parameters of our implementation and evaluation. 10 In brief, this framework looks to determine how courses of action taken to execute a program or innovation result in observed patterns of initial use by examining an organization’s readiness for change, the quality of the implementation policies and practices, and the climate for implementation. 10 There were 3 phases to the implementation strategy. The first phase engaged FMC leadership and clinical champions around the concept and evidence-base of care management, and its potential contribution to improving patient-centered care. Although initial funding for the care manager position was provided through state agency grants for defined populations, such as Medicaid and uninsured patients, an operational decision was made for care management services to be made accessible for all FMC patients. A job description was developed for the care manager position with a requirement of clinical licensure (eg, registered nurse or licensed clinical social worker), excellent communication and problem-solving skills, and a minimum of 3 years of experience in health care. The responsibilities and functions of the care manager included (a) receipt of referrals and identification of patient candidates via health service databases, (b) comprehensive assessment of patient barriers to care and concomitant care planning, (c) facilitation of services and communication with care team, and (d) participation in interdisciplinary case reviews and quality improvement activities.
Phase II began posthiring and included several promotional strategies to raise the visibility of the care manager, such as screensavers at computer workstations, bookmarks for providers and patients, and attendance and announcements at FMC meetings and other clinical venues. We worked with the UNCHCS health information technology unit to create a care management template in the electronic health record during this phase. Phase III of implementation focused on effectively integrating the care manager within the FMC operational structure and workflow. Strategies included locating the care manager workplace centrally within the FMC, securing access to the appointment scheduling and health care system care management informatics systems, embedding the position into ongoing FMC quality initiatives, and establishing an evaluation plan for reporting interventions and utilization, such as point-of-care contacts and referrals.
Data Collection and Analysis
Two sources were used to determine the effectiveness of our implementation strategy; data elements from the care management system in the UNCHCS health record and electronic survey data from FMC providers and care staff. Process elements included the frequency of care manager assessments, types of interventions, and clinician reasons and communication patterns for referral to care management. We used satisfaction with care management services and frequency of emergency department visits and acute hospitalizations at UNC hospitals as primary outcome measures.
Results
A total of 110 FMC physicians and support staff were surveyed and we received responses from 71 individuals (64.5% response rate). Table 1 depicts the characteristics of the survey respondents. A majority of physicians (75%) and support staff (82%) reported interactions with the care manager, primarily via face-to-face, telephone, or electronic means. Nearly 70% of the contacts were for facilitating referrals for behavioral health services; however, assistance with financial, social, and community-based resources was also prevalent (60% to 70%). Satisfaction with care management services was very high (98% of respondents reporting satisfied or very satisfied), and 79% of the clinician and care staff reported that the care manager was frequently or always accessible when needed. Regarding the implementation strategy, clinicians and care staff noted that the most effective strategy was the outreach and direct contact that the care manager made with stakeholders (80%). In addition, personal introductions and an ongoing presence at standing FMC organizational meetings were also cited (63%), but other strategies such as handout cards and screensavers on clinic laptops were reported as less effective.
Characteristics of Survey Respondents (N = 71). a
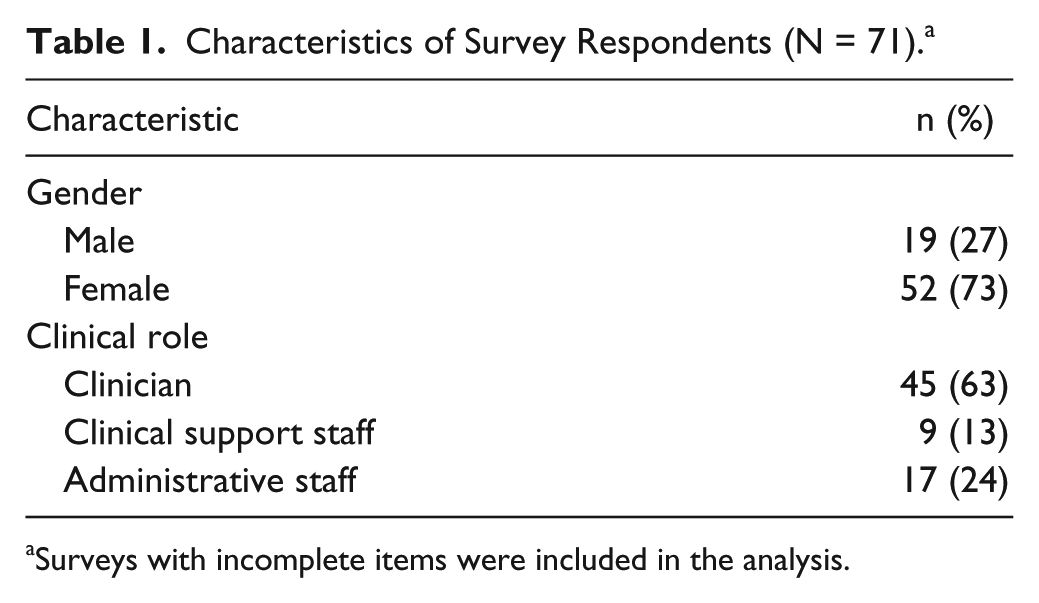
Surveys with incomplete items were included in the analysis.
Figure 1 displays a trend of emergency department visits and inpatient hospital admissions over a 24-month period for FMC patients who received services from the care manager. Trend shows an absolute decrease of 8 emergency department visits per month and an absolute decrease in inpatient admissions of 7.5 admissions per month during the initial 2-year implementation period.

Trend line for emergency department (ED) visits and acute hospital admissions.
Discussion
Care managers will play an increasingly vital role in the ongoing transformation of primary care.3,11 Although several studies have documented the efficacy of care managers or care management services with clinical and health service outcomes,6-9 this prior work is remarkable for the lack of attention given to how effectively care managers were incorporated into clinical practice workflows. To our knowledge, the present study is the first to describe and evaluate an implementation strategy for embedding care management in a PCMH. Conceptually, implementation may be considered as the period during which intended users of an innovation become skillful in using a new procedure or program; evaluating the implementation process requires determining how well the innovation is delivered or used. 12 A primary concept in the organizational model of innovation implementation is implementation effectiveness, which is the aggregated consistency, quality, and appropriateness of innovation use within an organization.12-14 Operationally, this concept influenced 2 strategic decisions: (a) targeting FMC leadership and other stakeholder support for the care manager as an initial aim and (b) making care management services available for all FMC patients in order to standardize the practices associated with accessing the care manager.
Within organizations, effective implementation of innovations balances the competing demands of adaptation and fidelity.15,16 We allowed for adaptation by deploying several strategies, such as screensavers at computer workstations and bookmarks for providers and patients, with overall fidelity to effectively promoting the visibility of the care manager. Physicians and care staff uniformly noted that outreach and personal communication by the care manager were key elements in effectively implementing the position into the FMC workflow.
The effectiveness of any innovation depends on the effective implementation of that intervention. 17 Health care organizations often quickly adopt complex innovations and subsequently find that sustained implementation proves challenging, time consuming, and costly. 18 For example, findings of the National Demonstration Project showed that adoption of PCMH components resulted in only modest improvements in chronic care outcomes, was costly, and resulted in lower overall patient centeredness, 19 which may be the result of ineffective implementation of PCMH innovations. In the present study, attention to the parameters of implementation may have contributed to the overall reductions in emergency department and hospital utilization.
In summary, although our setting is an academic family medicine center—which limits the generalizability of our findings other PCMHs—we found that an organizational model of innovation implementation was an effective approach to guide the process of incorporating care management services into the structure and workflows of a PCMH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.