
Abstract
Introduction
With the development of patient-centered medical homes, primary care in the Unites States is changing the focus of care and payment models. Many of the payment models are based on the patient’s number of medical comorbidities and their severity. The presence of more than one chronic medical condition in a patient, often termed “multimorbidity,” has been demonstrated to have a prevalence rate of at least 65% in patients older than 65 years.1-3 In a study of primary care patients older than 65 years, Rohrer et al, 4 demonstrated that those with moderate comorbidity had elevated odds of being frequent visitors to primary care (odds ratio [OR] = 6.13, confidence interval [CI] = 3.27-11.49), compared with patients with no comorbidity. In a recent study of 3309 patients in a primary care setting, when controlling for age, gender, and health care coverage, additional medical comorbidities led to increased primary care visits, hospital admissions, and total health care costs. 5 Therefore, efforts should be made to identify ways to decrease multimorbidity, as measured by complexity of care tiering systems, in order to improve clinical outcomes and control health care costs.
Depending on the payment model, mental health issues may or may not have a significant impact on defining whether a patient may need more complex care. The effect of mental health in determining multimorbidity generally has been due to the presence or absence of a mental health diagnosis. However, major depressive disorder or dysthymia have targeted goals of clinical remission, unlike many other nonpsychiatric diagnoses. Therefore, ability to reach the clinical goals (remission versus persistent depressive symptoms) may have a role in determining future complexity of care tier.
Studies have shown that collaborative care management (CCM) has been effective in the treatment of depression by decreasing depression symptomatology.6-9 CCM uses a nonphysician care manager, depression registry, and treatment guidelines with support of a consulting psychiatrist to assist the primary care provider in the care of the patient with major depression. While CCM has been shown to be effective in the treatment of depression and that achieving depression remission was correlated with decreased outpatient visit counts, 10 some studies have demonstrated increased short-term costs after implementation of CCM, despite long-term cost reduction. 11 This is thought to be because of patient “activation,” or increased patient engagement with treatment.11,12 Our prior studies of primary care patients in CCM have shown that those who have increased depression severity and other comorbidities tend to have worse clinical outcomes.13-15 However, our prior studies of patients in CCM did not evaluate the impact of clinical remission on future complexity of care tiering. This distinction is imperative for those who care for depressed patients. If persistent depressive symptoms (PDS) increase the likelihood for a patient having a future elevated medical complexity score, identification and improved management of those at risk would be indicated.
The hypothesis for this study was that for patients who were diagnosed with major depressive disorder or dysthymia and treated with CCM, clinical outcome of the depression (remission vs persistent depressive symptoms) at 6 months would have an association with a lower future complexity of care tier level. If this hypothesis was correct, it could be argued that enhanced depression treatment (such as with CCM) would be warranted, versus limiting care coordination to patients who have an elevated complexity tier.
Methods
The study setting was the primary care practice of a large tertiary clinic in Rochester, Minnesota. Approximately 100 000 adult patients were cared for by the staff of Department of Family Medicine, Division of Primary Care Internal Medicine, and Community Pediatrics and Adolescent Medicine of Mayo Clinic during the study period. Primary care adult patients who were diagnosed with major depressive disorder or dysthymia and a Patient Health Questionaire–9 (PHQ-9 16 ) score of ≥10 from March 1, 2008, through December 31, 2011, and had a complete set of intake and 6-month follow-up data were included. After eliminating patients who did not have a complexity of care tier level as of December 2012 and those who declined research participation, the study cohort included 1419 patients. The only clinical exclusionary criterion for enrollment into CCM was the clinical diagnosis of bipolar disorder.
After the clinical diagnosis and the patient agreement to enrollment into CCM, the care manager met with the patient for the intake process. This involved a review of prior mental health history (diagnoses and treatments), further patient self-assessment with the Alcohol Use Disorders Identification Test (AUDIT 17 ), Generalized Anxiety Disorder Questionnaire (GAD-7 18 ), and Mood Disorders Questionnaire (MDQ 19 ). The consulting psychiatrist met weekly with the care manager to review new patients as well as any enrolled patients with concerns. Recommendations for treatments were reviewed with the primary care provider prior to initiation. The number of care manager/patient contacts varied based on the clinical need. Full details of the development and implementation of our CCM have been described previously.15,20
In this study, the dependent variable was complexity of care tier level as of December 2012. The tiers were constructed with a software product called Adjusted Clinical Group (ACG) from Johns Hopkins. The ACG software determines patient complexity tiers using each patient’s age-, gender-, billing-based ICD-9 (International Classification of Diseases, 9th revision) diagnoses, and a tool that groups patients into 267 Expanded Diagnosis Clusters (EDC). The ECD group structure helps identify patients who exhibit specific symptoms or diseases. EDCs are further categorized into 27 major EDCs (MEDCs). Only 22 out of 27 MEDCs are used for care coordination tiering. Tiers are then calculated by the patients’ counts of MEDCs. All diagnoses with a MEDC are counted only once, therefore, the number of diagnosis is not always equal to the number of MEDC that propels each tier. Tiers are driven by diagnosis clusters and range from 0 (the least medically complex patient) to 4 (the most medically complex patient). Any diagnosis that was not billed in the past year may not have been captured due to the lag in billing data.
The validity of the Johns Hopkins complexity groups (originally called Ambulatory Care Groups) was investigated soon after their initial development when the association between the ACG score and geographic variation in utilization of primary care services and expenditures were demonstrated for some but not all of the groups. 21 The ACG system has been refined over 2 decades of use. It is currently at version 10.0. 22
The independent demographic variables for this study were age (at enrollment into CCM), gender, race and marital status. The clinical predictor variables were baseline PHQ-9, clinical diagnosis, depression outcome at 6 months (PHQ-9 score), and the presence of medical comorbidities. A diagnosis of diabetes, cancer, chronic obstructive lung disease, dementia, congestive heart failure, or coronary artery disease was determined by an automated screening of ICD-9 codes in the electronic medical record. This was a multiclinic study within the same practice; therefore, location was also defined as a variable. Also, the year of enrollment into CCM was recorded, to determine if length of time from enrollment impacted the tier level determination.
Categorical data were analyzed with χ2 testing while Mann-Whitney testing was used for statistical analysis of the continuous variables (because of nonnormal distribution). Multiple logistic regression modeling for health care home tier was performed while retaining all independent variables studied. Calculations were performed on MedCalc software (http://www.medcalc.org, version 12.4.0.0). This study was reviewed and approved by our institutional review board.
Results
Of the 1894 patients enrolled in the study, a minority were tier 0 (3.9%, n = 73) whereas the majority were tier 1 (47.4%, n = 898). The remaining participants were tier 2 (30.8%, n = 583), tier 3 (12.3%, n = 233), and tier 4 (5.6%, n = 107).
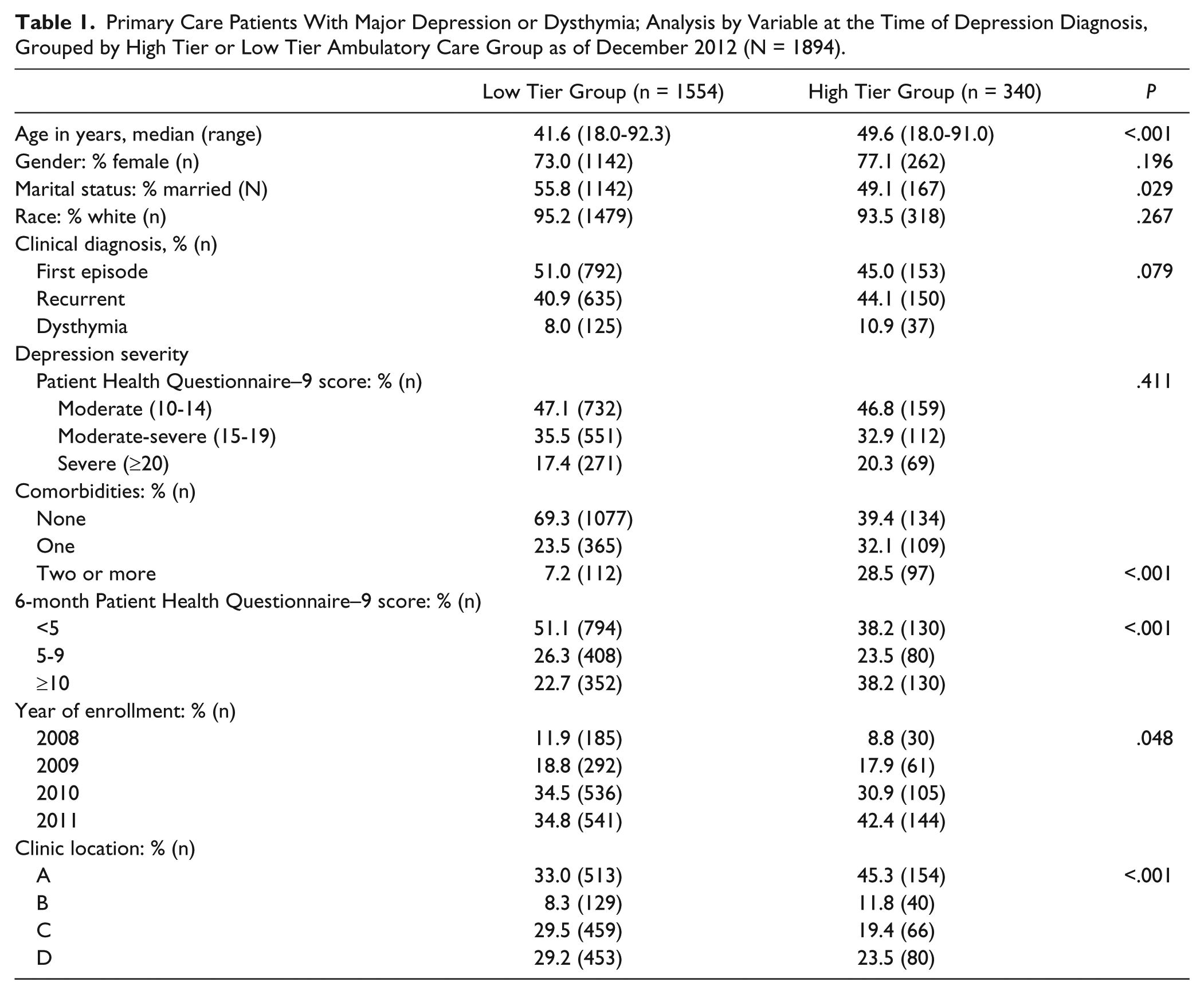
Clinical practices such as ours generally are more concerned with the more complex (higher tiered) patients as they generally are assumed to require more resources and may be involved in care management programs. Thus, further analysis was performed by categorizing those patients into the higher tiers (HT group) of levels 3 and 4 and the lower tiers (LT group) of levels 0, 1, and 2. Table 1 demonstrates that the HT group was more likely older, not married, and have more comorbidities that the LT group. Since age and comorbidities helped to define tier, these results were not unexpected. There were no significant differences between the LT and HT groups for gender, race, depression diagnosis or severity. The presence of PDS after 6 months of enrollment into CCM was 38.2 % in the HT group compared with 22.7% in the LT group (P < .001).
Primary Care Patients With Major Depression or Dysthymia; Analysis by Variable at the Time of Depression Diagnosis, Grouped by High Tier or Low Tier Ambulatory Care Group as of December 2012 (N = 1894).
Multiple logistic regression analysis of the odds ratio for a patient being included in the HT group was performed. Figure 1 shows that when controlling for all the other independent variables, age (OR = 1.022, CI = 1.013-1.030, P < .001), gender (female, OR = 1.380, CI = 1.020-1.868, P = .037), marital status (married, OR = 0.730, CI = 0.563-0.947, P = .018), and the presence of comorbidities (1, OR = 1.986, CI = 1.485-2.656, P < .001; ≥2, OR = 4.678, CI = 3.242-6.750, P < .001) were the only baseline characteristics that were associated with future HT levels. The presence of PDS at 6 months conferred 2.280 (CI = 1.673-3.107, P < .001) times likely odds of HT level compared with clinical remission at 6 months. Year of enrollment into CCM, race, and clinical location, were not significant predictor components in multiple regression analysis.

Odds ratio for being classified as high tier (3 or 4) of Ambulatory Care Groups in primary care patients with major depression or dysthymia, by variable.a
Discussion
The original hypothesis for this study was correct. In CCM patients, treatment of their depression to remission by 6 months was associated with a lower future complexity of care tier, while PDS at six months was associated with a significantly elevated OR of a future higher complexity of care tier (OR = 2.280, P < .001). This effect did not diminish over the course of the 4 years of this study. The clinical outcome of the depression at 6 months, specifically PDS with a PHQ-9 of ≥10 was highly predictive of at least a tier 3 complexity level, controlling for all other studied variables. The time (years) from enrollment was not a factor in the tier levels, suggesting that PDS at 6 months placed a patient at higher risk, irrespective of current depression status or length after treatment (at least within the 4 years of this study).
In patients who have a history of depression, as expected, age and the number of medical comorbidities are associated with increased odds of being in a higher health complexity tier. There are 2 significant clinical finding from this study. First, it should alert the clinician to the importance of active management of depression, with a goal of significant improvement (ie, remission) by 6 months, in an attempt to keep patients (especially those older patients with more comorbidity) from entering into the higher medical complexity tiers. Future studies looking at these high-risk patients and prospective outcomes would be intriguing. Second, it would appear that in a depressed patient population, PDS after 6 months conveys as much risk as an additional comorbidity in determining future health complexity.
Use of the ACG tier level as an outcome measure reflecting resource use was a novel feature of this study. One previous study assessed tier (via the ACG assignment) in patients with depressive symptoms but did not evaluate impact of successful depression treatment on future tier assignment. However, it did find that participants with depressive symptoms were more likely to be assigned to the 2 highest tiered ACGs. Also, the study investigated whether medical comorbidities contributed to higher diagnostic test costs in depressed patients. When controlling for the ACG tier assignment, depression symptoms were no longer associated with higher diagnostic charges. 23
There are several limitations to this study. This was a retrospective analysis of the data and there was only a single complexity of care tier level (not compared over time). Another limitation is the fact that only 4 years of data are presently available; long-term impacts of tier rankings beyond 4 years are not yet available. Additionally, this study only evaluated those patients who were in CCM; whether the lower future tier was secondary to successful depression treatment or CCM itself is unknown.
Conclusions
Patients with the diagnosis of major depression or dysthymia and an initial PHQ-9 score of 10 or greater, show greater association with future complex ACG tier levels if depression was not treated to remission by 6 months. This association was demonstrated while controlling for the patient’s age, gender, race, and health comorbidities. This study demonstrated the importance of the goal of significant improvement (ie, remission) of depression symptoms by 6 months, in an attempt to keep patients (especially those older patients with more comorbidity) from entering into the higher medical complexity tiers.
Footnotes
Acknowledgements
Mr Isaac Johnson, MBA, assisted with abstraction and collection of the data.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Angstman has a consulting agreement with Tamber Health. Tamber Health was not involved in study design, data analysis, or article preparation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received departmental funding.