
Abstract
Introduction
Between 20% and 70% of patients have at least one medication discrepancy at discharge, and patients with discrepancies are twice as likely to be rehospitalized within 30 days.1-5 Discharge-related medication discrepancies increase health care resource utilization, including rehospitalization and emergency department (ED) visits.2,3,6 Medication discrepancies cause discharge-related adverse drug events, which occur in 12% to 17% of patients, and the incidence increases when 8 or more medications are prescribed.1,3,4,7-9 The risk of having an adverse drug event is greatest during the first 7 to 10 days after discharge, which is a particular concern for primary care providers (PCPs) who may not be able to offer patients appointments within this time frame. 10 A pharmacy intervention immediately after discharge may address this concern.
With national health care quality organizations and the Affordable Care Act increasing accountability for rehospitalization, health systems will face financial penalties if they fail to meet 30-day rehospitalization performance measures.11-13 A recently published systematic review of transitional care interventions included 47 studies evaluating various strategies to improve discharge-related patient safety, but no conclusions could be drawn regarding an optimal strategy. The review identified clinical pharmacist interventions as a promising approach based on literature evaluating primarily telephone-based strategies. 14 Five studies have evaluated the impact of pharmacist telephone follow-up to reinforce the discharge plan, resolve medication-related problems, and provide medication counseling within 2 to 7 days of hospital discharge from general medicine services.1,3,15-17 Some, but not all the studies demonstrated a significant reduction in rehospitalization rates. Although these studies suggest a decrement in health care resource utilization and the need for involving pharmacists in care transitions, evaluation of other pharmacist interventions is warranted. To date, no prospective studies have evaluated the impact of a post-discharge outpatient pharmacist visit on these endpoints. The purpose of this study is to evaluate the impact of a transitional care clinic visit conducted by a pharmacist compared with usual care on the resolution of medication discrepancies and incidence of rehospitalizations and ED visits.
Methods
Study Design
This prospective, randomized, open-label, pilot study was conducted at an 804-bed academic medical center from October 2009 to April 2011. Patients with risk factors for rehospitalization admitted to the family medicine inpatient service (FMIS) who also received primary care at the health care system’s outpatient family medicine center were eligible for inclusion. Table 1 displays the inclusion and exclusion criteria. 13 Because of difficulty in screening and enrollment of study participants during the first year of the study, the inclusion criteria were broadened for the second year of the study. Following institutional review board approval, patients admitted to the FMIS were screened for inclusion. Eligible patients were approached for participation, consented, and randomized. During the first year of the study, 30 patients were enrolled and a random number generator was used for randomization. Because of unequal allocation of patients to the study arms, block randomization with a block size of 4 was used for the second year of the study, during which 31 patients were enrolled.
Inclusion Criteria and Exclusion Criteria.
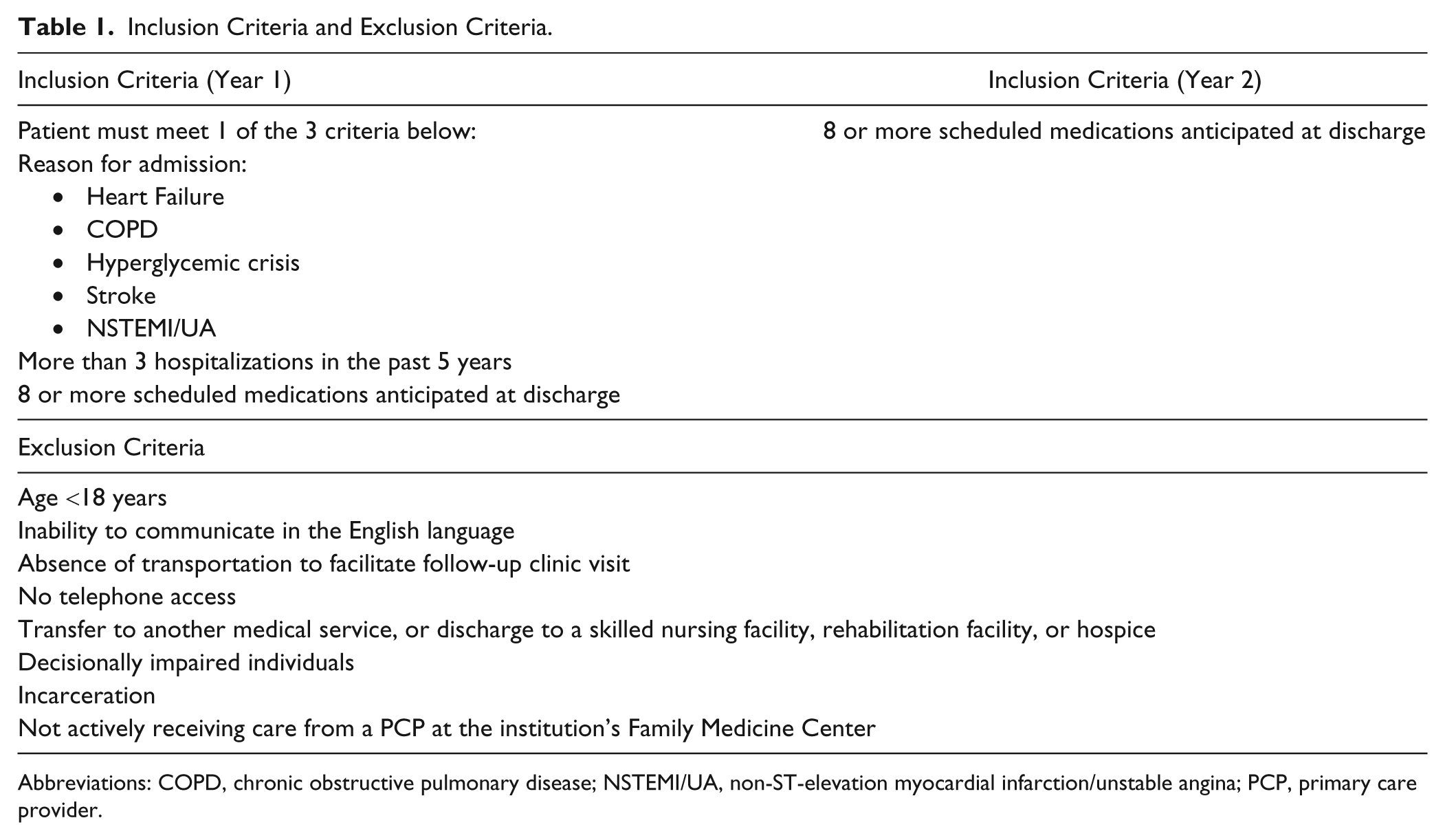
Abbreviations: COPD, chronic obstructive pulmonary disease; NSTEMI/UA, non-ST-elevation myocardial infarction/unstable angina; PCP, primary care provider.
At the study institution, pharmacists provide clinical pharmacy services for the FMIS and outpatient family medicine clinic. Inpatient clinical pharmacists round with the medical team daily, review and monitor medications for effectiveness and safety, and make recommendations to the physician staff to optimize medications. Subjects in both groups received this usual care from the inpatient pharmacist. The role of the inpatient pharmacist in the study was to collaborate with the inpatient medical team to create a Best Possible Medication Discharge List (BPMDL) for all study subjects just prior to discharge. Use of BPMDLs as a research method for identification of discharge-related medication discrepancies has been described previously by Wong and colleagues. 5 As in the study by Wong et al, 5 the BPMDL was used to identify medication discrepancies, and it served as the gold standard list of medications that the patient should take after discharge. The BPMDL accounted for home medications, medication changes made during the hospitalization, and medications that should be initiated or discontinued on discharge.
Subjects in the intervention group were scheduled for a care transitions clinic visit with a clinical pharmacist approximately 72 hours postdischarge, and prior to the posthospitalization PCP visit. The visit involved performing a complete medication history, identifying and resolving medication discrepancies, creating a current medication list for both the medical record and the patient, and counseling on appropriate medication use. During these visits, the pharmacist identified discrepancies between the BPMDL and the discharge summary and characterized medication discrepancies using predefined categories. 5 Study subjects in the usual care group were scheduled to see their PCP for a posthospitalization visit with no interim pharmacist intervention. Medication discrepancies of study subjects not attending care transitions visits were identified and characterized by study personnel in the same manner as those in the intervention group.
Study personnel reviewed study subjects’ medical records to quantify 30-day ED visits and rehospitalizations at the study institution. All study subjects received a phone call approximately 30 days after discharge to report hospitalizations or ED visits at outside institutions. Only hospitalizations and ED visits at the study institution were included for those patients who were not able to be contacted after 3 phone call attempts.
Study Outcomes
The 3 prespecified primary outcomes of this study were a composite of the occurrence of a hospital admission or an emergency room visit within 30 days after hospital discharge and the resolution of medication discrepancies before the PCP visit. Secondary outcomes include the individual rates of rehospitalization and ED visits within 30 days after discharge.
Statistical Analysis
The association between the intervention and each of the primary outcomes and secondary outcomes of 30-day rehospitalization and 30-day ED visits (all dichotomous), was evaluated using a 2-sided Fisher’s exact test to determine the significance with an α = .05. The intention-to-treat population included all randomized individuals, and the per-protocol population included only those attending the pharmacist clinic visit. The pre-specified primary outcomes were for the intention-to-treat population. We counted no more than one rehospitalization and ED visit for each study subject. If patients were admitted to the hospital from the ED, they were not considered to have both an ED visit and a hospital admission. Using an estimated incidence of 5% for the primary composite outcome (30-day rehospitalization and ED visits), a sample size of 60 patients (30 patients in each arm) was calculated to reach at least 80% power to detect a 32% reduction in the primary outcome with an α = .05. Although the intervention arm was slightly below the enrollment target for the power calculation, the overall study met power since the enrollment target was exceeded in the control arm. All statistical procedures were performed by SPSS 20.0 (IBM SPSS Inc, Chicago, IL).
Results
Patients
A total of 61 subjects (24 randomized to the intervention arm and 37 to the usual care arm) with a mean age of 62.8 years were included in the study. Of the 61 subjects included in the study, 37 (61%) were women, 36 (59%) were African American, and 25 (41%) were Caucasian; there were no statistically significant differences in baseline characteristics between groups.
Thirty-three patients (54%) had medication discrepancies at discharge, with a mean of 1.03 and range of 0 to 7 discrepancies per subject. There was no difference between the intervention group and usual care group in percentage of subjects with discrepancies at discharge (50% vs 56.8%, P = .793). Medication discrepancies were categorized as inappropriate medication omission (n = 23), wrong dose (n = 18), inappropriate drug continuation (n = 16), inaccurate instructions (n = 3), incorrect duration (n = 1), wrong schedule (n = 1), and medication without known indication (n = 1). Ten patients (42%) randomized to the intervention arm attended the pharmacist clinic visit; an additional 2 patients did not attend their appointment, but followed up with the pharmacist by phone for medication reconciliation. The mean time to the pharmacist visit was 4.7 days after hospital discharge.
Outcomes
Study participants randomized to the intervention had a significant reduction in the primary composite outcome of 30-day rehospitalization and ED visits compared with the usual care arm (0% vs 40.5%, P < .001). In addition, there was a significant difference in the 30-day rehospitalization rate (0% vs 32.4%, P = .002) and 30-day ED visit rate (0% vs 29.7%, P = .004) between the intervention and usual care arm. Of the subjects with medication discrepancies at discharge, 50% of the discrepancies were resolved in those in the intervention arm versus 9.5% in the usual care arm by the conclusion of the posthospitalization PCP visit (P = .015). In the per-protocol analysis, all discrepancies were resolved in patients attending the pharmacist visit versus 9.5% in the usual care group (P < .001; Table 2).
Primary and Secondary Outcomes.

Abbreviations: ED, emergency department; ITT, intention to treat; PP, per protocol; PCP, primary care provider.
Statistically significant difference (P < .05).
Discussion
A face-to-face posthospitalization care transitions visit with a pharmacist improved medication discrepancy resolution and reduced 30-day rehospitalization and ED visits in this study. These results are consistent with the findings of other studies evaluating pharmacist telephone interventions, but suggest a possible benefit with face-to-face encounters over telephone interventions, which have not consistently decreased 30-day rehospitalizations. The additional benefit with a face-to-face intervention may be associated with use of nonverbal communication to assess for understanding, and the ability to review correct use of medical devices such as inhalers, glucometers, and injectable medications. The medication discrepancy rate in our study is consistent with rates reported in the literature.1-5 The pharmacist visit no-show rate in this study roughly approximates the no-show rate for initial primary care visits reported in the literature of 45%. 18 After the initial scheduling of the pharmacist visit in this study, patients were not reminded of the appointment. A phone call reminder prior to the visit may have improved the show rate to this visit.
The most significant limitations of this pilot study are the small sample size and clinic no-show rate. Additionally, despite randomization, study arms were unequally sized at the conclusion of the trial. Although a medication discrepancy identification tool was used and discrepancies were categorized into prespecified groups to reduce subjectivity, clinician judgment was required, which could introduce bias. Other limitations include the broadening of inclusion criteria for the second year of the study because of difficulty in screening and enrollment. The possibility of recall bias due to subjects’ self-reporting of outside hospital ED visits and rehospitalizations cannot be excluded. Only rehospitalization and ED visit data from the academic medical center, not outside institutions, were reported for 7 subjects who were not able to be contacted by phone (n = 5 in the intervention arm and n = 2 in the usual care arm). Thus, some ED visits and rehospitalizations may not have been captured in these subjects. Finally, the study may have been strengthened by not limiting inclusion to only English-speaking subjects.
Although our study did not address cost-effectiveness, if the findings of this pilot study are validated in larger studies, transitional care pharmacist interventions may provide cost savings through rehospitalization and ED visit-related cost avoidance. They may also reduce indirect costs as health systems avoid reimbursement penalties by meeting reshopitalization-related performance measures. Cost savings associated with postdischarge pharmacist telephone interventions’ rehospitalization decrements have been estimated at approximately $35 000 for every 100 patients receiving the intervention. 16 The cost-effectiveness of a face-to-face pharmacist intervention needs to be further evaluated.
In conclusion, results from this study demonstrate that posthospitalization, face-to-face pharmacist interventions improve medication discrepancy resolution and decrease the incidence of 30-day ED visits and rehospitalization. Given the burden of medication-related problems on patient safety and health care costs, such a strategic intervention could improve health care quality and decrease costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from the American College of Clinical Pharmacy Ambulatory Care Practice and Research Network was used to provide compensation in the form of a $15 gift card from a large retail store to subjects for study participation.