
Abstract
Background:
Clear processes to facilitate medication reconciliation in a hospital setting are still undefined. The observation unit allows for a high patient turnover rate, where obtaining accurate medication histories is critical.
Objectives:
The objective of this study was to assess the ability of pharmacists and student pharmacists to identify discrepancies in medication histories obtained at triage in observation patients.
Methods:
Pharmacists and student pharmacists obtained a medication history for each patient placed in observation status. Patients were excluded if they were unable to provide a medication history and family, caregiver, or community pharmacy was also unable to provide the history. A comparison was made between triage and pharmacy collected medication histories to identify discrepancies.
Results:
A total of 501 medications histories were collected, accounting for 3213 medication records. There were 1176 (37%) matched medication records and 1467 discrepancies identified, including 808 (55%) omissions, 296 (20.2%) wrong frequency, 278 (19%) wrong dose, 51 (3.5%) discontinued, and 34 (2.3%) wrong medication. There was an average of 2.9 discrepancies per patient profile. In all, 76 (15%) of the profiles were matched. The median time to obtain a medication history was 4 min (range: 1–48 min).
Conclusion:
Pharmacy collected medication histories in an observation unit identify discrepancies that can be reconciled by the interdisciplinary team.
Background
Medication reconciliation is defined by the American Pharmacists Association (APhA) and the American Society of Health-System Pharmacists (ASHP)
1
as the comprehensive evaluation of a patient’s medication regimen any time there is a change in therapy in an effort to avoid medication errors such as omissions, duplications, dosing errors, or drug interactions, as well as to observe compliance and adherence patterns. This process should include a comparison of the existing and previous medication regimens and should occur at every transition of care in which new medications are ordered or existing orders are rewritten or adjusted or if the patient has added nonprescription medication to his or her self-care.
A complete medication reconciliation process begins with accurate medication history-taking. Inaccuracies in the medication reconciliation process can lead to potential adverse drug events (ADEs), commonly defined as unintended complications related to medication use. ADEs occur in 12%–18% of hospitalized patients, including patients who are admitted for treatment of an ADE. 2 Prolonged length of hospital stay, increased frequency of emergency room visits, and hospital readmissions are serious consequences potentially related to ADEs. 3 Medication discrepancies, within the medication reconciliation process, occur in approximately 70% of admitted and discharged patients, 29.5% of which can lead to harm and ADEs. 4
Since 2005, The Joint Commission (TJC) has evaluated each hospital’s medication reconciliation process. Over the past few years, TJC has changed their standards when evaluating this process due to its complex nature. The July 2011 National Patient Safety Goal 03.06.01, was issued with simpler components; however, the entire medication reconciliation process remains a challenge for most institutions across the United States. 1
Medication history-taking is the first, and possibly the most influential, step in medication reconciliation. These histories have traditionally been obtained by physicians, nurses, nurse practitioners, physician’s assistants, and/or pharmacists. With this in mind, APhA and ASHP 1 collaborated to issue their goal of medication reconciliation, which is “to obtain and maintain accurate and complete medication information for a patient and use this information within and across the continuum of care to ensure safe and effective medication use.” Several studies have demonstrated the value that pharmacists and student pharmacists contribute to the medication history-taking process.5,6
In 2007, Lubowski and colleagues demonstrated the role of student pharmacists in obtaining medication histories on patients newly admitted to a general medicine or general surgery service. After obtaining daily lists of newly admitted patients, students interviewed each patient and called the community pharmacy on an as-needed basis. The students then compared the medication history they obtained to the history documented in the medical record and recorded any discrepancies found. Discrepancies included omissions, wrong dose, therapeutic substitutions, change of medication from prescription to nonprescription, and change of combination products to single agents. A total of 922 medication discrepancies were found among the 330 patients interviewed. Discrepancies were identified in 75% of patients with a mean of 2.8 discrepancies per patient. The average time per patient interview was 9.3 min. 5
Similarly, Mersfelder and Bickel investigated the frequency of discrepancies discovered and corrected by student pharmacists after obtaining medication histories on an internal medicine service. One to two patients were randomly assigned to students daily, where they would then obtain the medication history by interviewing the patient and/or family member in addition to contacting the patient’s community pharmacy. Of the 326 patient charts included in the review, discrepancies were identified for 440 prescription medications and 414 nonprescription medications. In all, 36% of patient charts required changes in the dose and 30% required changes in the frequency. Furthermore, due to omissions in the medication history, 34% of patient charts required the addition of the dose and 23% required the addition of the frequency. 6
Other studies have also evaluated pharmacy involvement in medication history-taking. Vasileff et al. 7 found 75.6% of patients had one or more unintentional discrepancies in the usual care group compared with 3.3% in the “pharmacist medication charting” arm. Marotti et al. 8 found the number of medications charted at an incorrect dose or frequency was significantly reduced in the pharmacist history arm.
The recent literature is unable to define clear processes to facilitate medication reconciliation in a hospital setting. To the best of our knowledge, a similar study has not been conducted in an observation setting. The observation unit experiences a high patient turnover rate by design, where obtaining accurate medication histories within 24 h is critical and challenging. The objective of this study was to assess the ability of pharmacists and student pharmacists to identify discrepancies in medication histories obtained at triage in observation patients.
Methods
After receiving approval from the HackensackUMC Institutional Review Board (IRB), approval number 00003690, we included the patients if they were in an observation status, located in the observation unit, and under the care of the observation team. Patients were excluded if they or their family, caregiver, or community pharmacy were unable to provide a medication history.
Prior to initiation of student involvement, each student was trained on how to collect a comprehensive medication history, regardless of prior medication history training. A 2 h didactic lecture was presented to the students reviewing appropriate medication history-taking techniques. A pharmacist then demonstrated a live medication history collection and supervised several student pharmacist led sessions. Student pharmacists were supervised until they were deemed competent to independently obtain medication histories by a supervising pharmacist. Student pharmacists were also periodically monitored anonymously throughout the study by a pharmacist to maintain quality control. A waiver of informed consent was granted by the local IRB.
After evaluation in the Emergency Department, patients are discharged, placed into an inpatient status, or an observation status for a period of up to 48 h. Pharmacists and/or student pharmacists obtained an updated list of patients in the observation unit from the unit clerk daily. Pharmacists and student pharmacists then attempted to obtain medication histories from all patients under the care of the observation team.
To obtain the medication history, pharmacists and student pharmacists would first approach the patient to obtain the medication history, if the patient could not provide their medication history, the pharmacist or student pharmacist would then contact the patients caregiver and/or community pharmacy. When taking a medication history, pharmacists and student pharmacists used the medication reconciliation data form to record their findings. After collecting the medication history, the pharmacists and student pharmacists then compared their history to the history collected at the time of triage, documented in Epic, the electronic health record (EHR). The triage-collected history is typically obtained by registered nurses, which served as the control. The triage medication history may have been obtained by the same or different source than the pharmacy collected medication history. Pharmacists and student pharmacists then populated a spreadsheet with the medication history and allergy information obtained during the interview, the documented medication history and allergies in the EHR, and the time needed to perform the medication history. All discrepancies noted were re-evaluated with the patient, caregiver, and/or community pharmacy and then reported to the patient’s care provider for reconciliation to the fullest extent possible. Utilizing this information, discrepancies and “unable to compare” drugs (see Appendix 1) were tallied. Patient profiles and the accuracy of individual medication records were counted as well. Discrepancies included incorrect drug, dose, frequency, and omissions. Medication records and patient profiles were considered “unable to compare” if the EHR contained information in the documented history, which the pharmacist or student pharmacist was able to obtain through interview and could not be confirmed by an additional information source. In this instance, it cannot be determined which medication history was more complete.
The primary outcomes included quantifying the total number of discrepancies and characterizing those discrepancies as omissions, wrong dose, wrong frequency, wrong drug, or discontinued drug. Secondary outcomes included the percentage of matched versus mismatched patient profiles, drug records, and documented allergies, as well as the mean time to obtain a medication history, mean number of discrepancies per patient profile, and mean number of medications per patient profile.
Results
A total of 501 medication histories were collected, accounting for 3213 medication records. There were 1467 discrepancies found, including 808 (55%) omissions, 296 (20.2%) wrong frequency, 278 (19%) wrong dose, 51 (3.5%) discontinued, and 34 (2.3%) wrong medication (Figure 1).

Total medication reconciliation discrepancies (n = 1467).
Of the patient profiles analyzed, 379 (76%) were considered mismatched, defined as containing at least one discrepancy, with 76 (15%) matched and 46 (9%) unable to compare (Figure 2).Of the 3213 medication records analyzed, 1312 (41%) were found to be mismatched, and 1176 (37%) were matched, with 725 (22%) unable to compare (Figure 3).
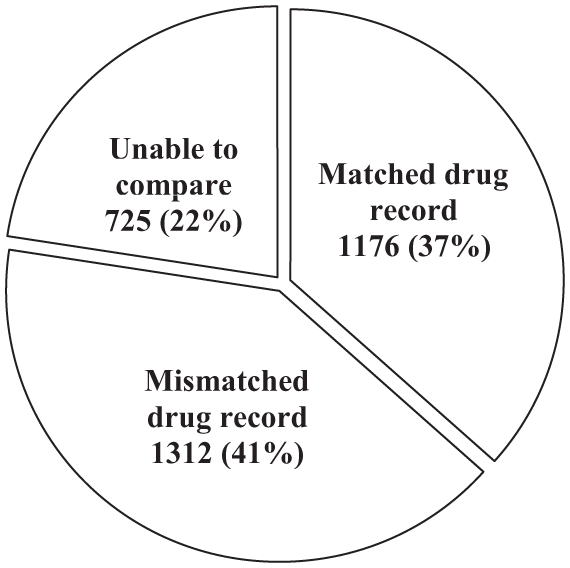
Matched versus mismatched drug records (n = 3213).
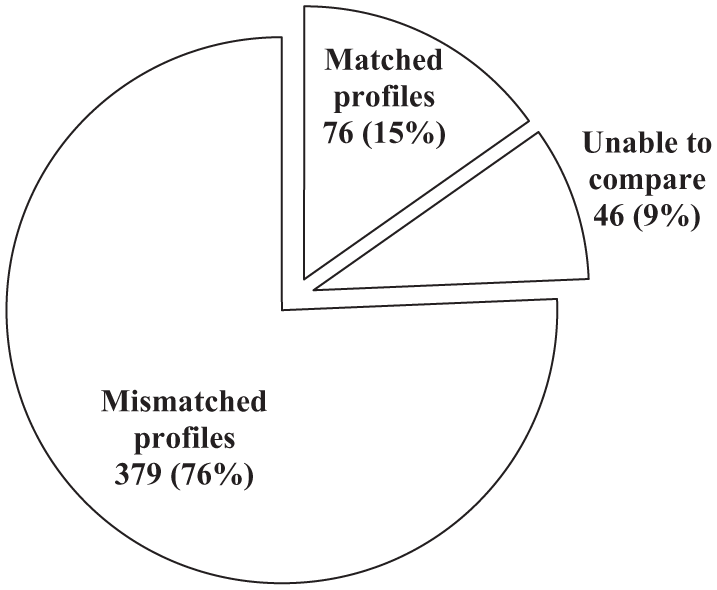
Matched versus mismatched patient profiles (n = 501).
There was an average of 6.4 medications and 2.9 discrepancies identified per patient profile. Of 257 profiles analyzed for allergies, 217 (84%) matched the EHR data obtained during triage. The median time to obtain a medication history was 4 min (mean: 5.3 min; range: 1–48 min). This time did not include documentation or discussion with the providers. Association between medication profile complexity and time of the interview was not conducted.
Discussion
The percent discrepancies identified and the mean number of discrepancies from the study by Lubowski et al. 5 were similar to the results of our study, 76% and 2.9, respectively. The average time per patient interview for our study was less, with a median time of 4 min. In the Lubowski study, students would state to the patient, as per the documented script, that their interview would last approximately 15 min in length and would also discuss the patient’s prior experiences with medications.
When compared to the study by Mersfelder and Bickel, in our study, changes and additions were not differentiated for either frequency or dose. However, we found when changes and additions were combined, the results were similar: 59% of patient charts required an addition or change in frequency and 55% of patient charts required an addition or change in dose.
The observation unit was chosen due to the high patient turnover rate, with a typical length of stay less than 48 h. These data may be extrapolated and generalized to other units throughout the hospital because critical medication decisions are made within the first 24 h of a patient’s stay. Patients in the observation unit are not in critical condition and generally have fewer medications than patients in more critical units. This implies, then, that the potential impact throughout the facility is greater than that which was identified through our study.
Limitations
There were limitations to our study. A convenience sample of 501 observation patients was utilized. If patients had less than a 24 h length of stay, were in observation status on a weekend or national holiday, or were located outside of the observation unit, they were not included. There is also a limitation to comparing medication histories taken at triage and medication histories taken while the patient is in observation status. Patients in observation status potentially had more time to compile an more complete medication list, that is, a family member brought a list or bag of medications into the hospital, the patient is more alert and responsive when asked about their home medications. Allergy evaluation and time analysis was only performed on 51% and 35% of the total sample population, respectively. Pharmacists and student pharmacists were not formally blinded to the EHR prior to patient interview; however, as required by the study design, all pharmacists and student pharmacists referred to the EHR only after they obtained the patient’s medication history to ensure that the history obtained was strictly through interview and not subject to outside influence. If the pharmacist or student pharmacist noted any discrepancies with the EHR, they would contact the prescriber in charge of the care for that patient and notify them of the discrepancies for reconciliation purposes. Additionally, to maintain quality control throughout the study, student pharmacists were periodically monitored without their direct knowledge by a pharmacist. Notably, the overall impact of pharmacist-led medication history-taking on patient outcomes is unknown. After reviewing 22 hospital-reported medication incidents that were related to the observation units included in our study, there were two reports that were related to incorrect medication histories, during the time of this study. However, it is recommended that future studies employ the medication reconciliation model described in our study when evaluating the impact of pharmacist-led medication history-taking and medication reconciliation on positive and adverse outcomes related to medication errors and ADEs secondary to medication discrepancies found in patients’ medical records. Our study also did not capture the use of secondary resources to confirm medication histories if the patient was unable to provide it, or what specific medications were most frequently associated with particular discrepancies.
Conclusion
Our study demonstrated that pharmacy collected medication histories in an observation unit identify discrepancies to be reconciled by the interdisciplinary team. Several types of discrepancies were discovered but medication omissions occurred most commonly. Medication history-taking by pharmacists and student pharmacists can be done in a timely manner, with a median time of 4 min per history. Furthermore, studies are needed to determine whether pharmacist or student pharmacist collected medication histories has a measured effect on patient outcomes, such as decreasing adverse drug reactions.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.