
Abstract
Evidence supports the effectiveness of interventions delivered in primary care to promote physical activity (PA). Specifically, approaches where physician counseling is coupled with other strategies (eg, referrals to community resources) have been recognized as the most promising. The purpose of this study was to compare the effectiveness of a PA prescription plus referral intervention versus a prescription only intervention delivered in primary care. Ten family physicians and their female patients (N = 35, mean age = 36 years) were randomly assigned to 1 of 3 conditions: prescription plus (n = 12), prescription only (n = 12), and usual care (n = 11). The prescription plus group received a PA prescription plus a referral to a community program, the prescription only group received only the PA prescription, and the usual care group received usual health care. The Godin Leisure-Time Exercise Questionnaire was used to measure PA. A significant increase on the PA score (P < .05, partial η2 = .178) and on total weekly PA minutes (P < .05, partial η2 = .179) was observed in both prescription groups after the intervention. There were no significant group differences (P > .05). No PA changes were observed in the usual care group. Findings from this pilot study suggest that brief PA counseling and a prescription delivered in primary care can be effective for promoting PA among women. Referring patients did not seem to enhance the effect on PA.
Introduction
Getting people active is a priority for the public health sector as physical activity (PA) translates into numerous health benefits. 1 To achieve these benefits, adults should accumulate 150 minutes of moderate-to-vigorous intensity PA per week in bouts of 10 minutes. 2 Unfortunately, 85% of Canadian adults are not meeting these recommendations, where women are the least active. 3 Higher inactivity levels have also been observed in women from other countries, 4 which calls for the development of PA promotion strategies among women.
The primary care setting represents a promising venue in which PA can be promoted because inactive patients can be effectively reached 5 and patients are receptive to health care advice. 6 Furthermore, patients view physicians as a credible source of health information, 7 putting physicians in a unique position to promote PA. A variety of PA promotion strategies have been implemented in primary care, including brief PA counseling,8,9 PA prescriptions,10-12 and physician referrals to PA resources in the community13-17 or to PA counselors.18,19 Among these, approaches where physician counseling is coupled with additional sessions delivered by physicians or PA counselors or with referrals to community resources have been recognized as the most promising.5,20 Furthermore, findings from 2 systematic reviews suggest that physician referrals to PA resources can improve PA, albeit only in some groups and for the short term.21,22 Women have been found to have lower referral rates than men, 23 and a recent PA counseling intervention for reducing cardiovascular risks was found to be less effective in women than in men, 24 suggesting that these strategies may be gender dependent. Thus, the purpose of this study was to compare the effectiveness of a PA prescription plus referral strategy to a prescription only strategy for improving PA among women.
Methods
Participants and Design
This was an experimental pilot study conducted in a convenience sample of 35 female patients and 10 physicians recruited from a family medicine clinic in a mid-size Canadian city in 2010. Eligible patients were women between 25 and 45 years old, with a body mass index ≤35 kg/m2, viewed by their physicians as patients who could benefit from the intervention and who were not likely meeting the Canadian PA guidelines. The study design was a 2 (pre–post) by 3 (treatment group) mixed design. Physicians were randomly assigned to 1 of 3 study groups: prescription plus (PP; n = 4), prescription only (PO; n = 4), and usual care (UC; n = 2). Patients were assigned to the same condition as their physician. This study was approved by the General Research Ethics Board from Queen’s University.
Interventions
Physicians in both prescription conditions received a 30-minute face-to-face training session on how to conduct brief PA counseling and issue the PA prescription. The PA counseling and prescription were based on the 7-As model 25 (an extension of the 5 As—assess, advise, agree, assist, and arrange—model for PA counseling 26 ) and conducted in less than 3 minutes. The community program for the PP group was offered by the local public health unit and consisted of 8 weekly 90-minute sessions delivered by trained public health staff and was focused on enhancing PA and healthy eating. Physicians provided a list of their female patients and those deemed eligible were invited to participate through mailed letters followed by phone calls. Consenting patients were assigned to their physician’s condition, completed the baseline questionnaire and attended a consultation with their physician to receive the corresponding intervention. Patients in the PP group received brief PA counseling, a PA prescription and a referral to the community program. Patients in the PO group received brief PA counseling and a PA prescription. Patients in the UC group received usual care (ie, no special instructions given to physicians).
Physical Activity Measure
Participants completed the Godin Leisure-Time Exercise Questionnaire (GLTEQ)
27
online prior to their consultation with their physician and again 8 weeks later. The GLTEQ total score has been validated against maximum oxygen consumption (V
Statistical Analysis
Chi-square and McNemar tests were used to assess within-subject and between-group differences in the proportion of active patients before and after the intervention. To examine group differences on PA levels at both time points, a 2 × 3 mixed analysis of variance using intent-to-treat analysis and Bonferroni post hoc comparisons were conducted. Statistical significance was set at P < .05. All data analyses were conducted using the Statistical Package for the Social Sciences, version 18 for Windows.
Results
Ten (48%) out of 22 invited physicians in the clinic agreed to participate. Only 42 (11%) out of 378 eligible patients agreed to participate and 35 (9%) patients completed the study; 12 in the PP group, 12 in the PO group, and 11 in the UC group. Except for marital status and education, no significant group differences were observed on demographic characteristics and on PA levels at baseline (Table 1). Although 10 patients were classified as active at baseline, they were kept in the study given the small sample size.
Baseline Group Demographic Characteristics, Physical Activity Classification, and Physical Activity Scores.
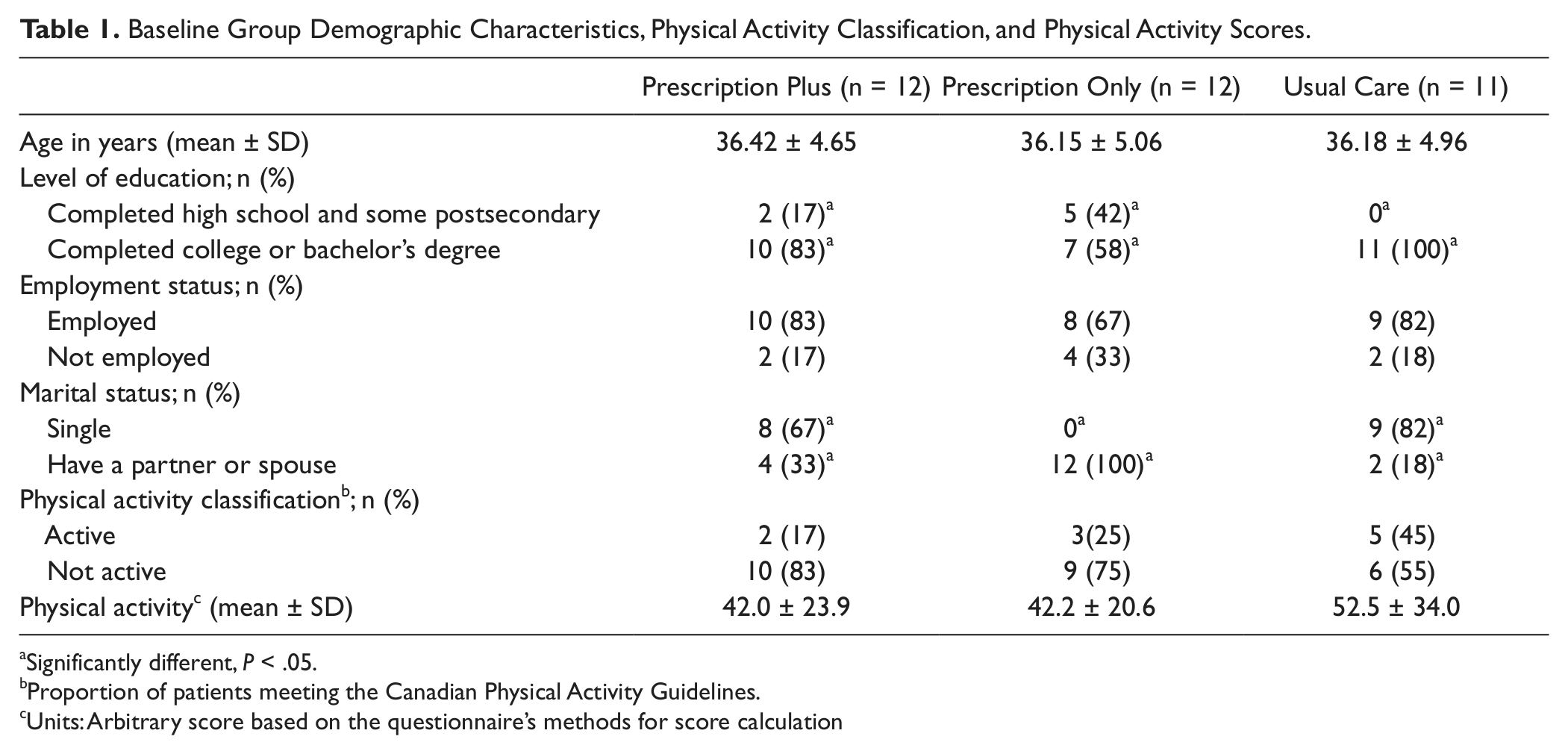
Significantly different, P < .05.
Proportion of patients meeting the Canadian Physical Activity Guidelines.
Units: Arbitrary score based on the questionnaire’s methods for score calculation
The proportion of patients meeting Canadian PA guidelines increased from baseline to post-intervention in the PP (17% to 50%) and PO (25% to 58%) groups, although these increases were not significant (χ22 = 1.12, P = .57). A significant increase on the PA score, F1,32 = 6.70, P < .05, partial η2 = .178, and the total weekly PA minutes, F1,32 = 6.90, P < .05, partial η2 = .179, was observed in both prescription groups after the intervention. Neither group differences nor time-by-group interactions were significant (P > .05; see Table 2). There were no changes on PA for the UC group.
Proportion of Active Patients and Group Means With Standard Deviations for Physical Activity Scores and Physical Activity Minutes at Baseline and Postintervention.
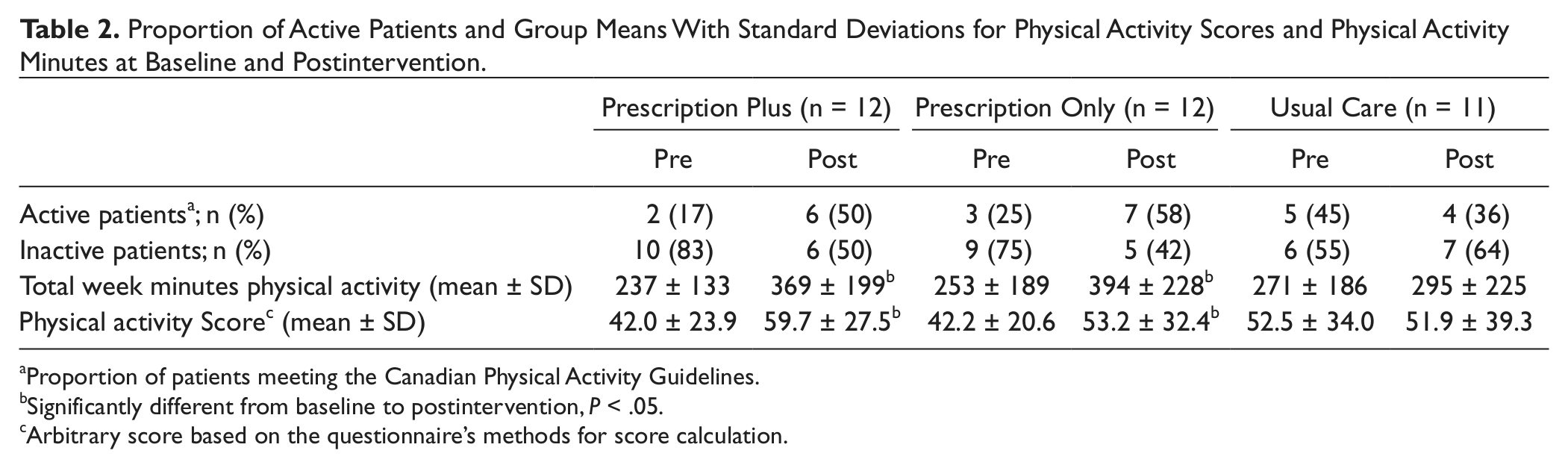
Proportion of patients meeting the Canadian Physical Activity Guidelines.
Significantly different from baseline to postintervention, P < .05.
Arbitrary score based on the questionnaire’s methods for score calculation.
Discussion
This study showed that, compared with usual care, both prescription interventions resulted in similar improvements in PA among this sample of Canadian women. The self-reported PA scores and PA minutes significantly increased form baseline to postintervention in both prescription groups. However, these PA indicators were not significantly different between these groups. Our findings suggest that having physicians prescribe PA to their patients is an effective way for improving PA among women in the short term.
These findings are similar to those found in prescription only interventions where short-term PA improvements have been achieved.8-12 In this study, the PO intervention was as effective as the PP intervention for improving self-reported PA in the short term. This suggests that brief PA counseling and a prescription may be more cost-effective for promoting short-term PA improvements than the prescription plus referral strategy, which is consistent with cost-effectiveness findings from similar studies7,16 If indeed the prescription only scheme is as effective for mid-life women as the more expensive prescription plus referral scheme, it would be a cost-effective strategy for promoting PA among women in general. Larger trials among women are needed to establish true cost-effectiveness.
Our findings differ from those in which the referral strategy achieved superior short-term improvements on self-reported PA as compared with prescription/counseling alone.13,16,17 It may be that the referral intervention in this study had no added value because the community program to which patients were referred was not focused solely on PA but also on healthy eating, which could have reduced the impact of the program on PA.
Although changes in the proportion of patients becoming active were not significant, these changes may nonetheless be clinically meaningful. For instance, most of the PA health benefits are experienced when inactive people become active, 1 and our findings suggest that the PA counseling/prescription promotes this transition. Furthermore, it has been suggested that even low levels of energy expenditure are associated with health benefits in women, 30 which means that even small increases in PA can have a significant impact on health. Thus, offering brief PA counseling and prescriptions can be a cost-effective strategy that can improve the health of inactive women.
The main strength of this study is the use of an experimental design that ensured the internal validity of the findings. The study limitations include the short follow-up and self-reported PA measurement, the fact that within-physician correlation among patients was not controlled for, and the small convenience sample.
Primary care is an effective setting for initiating PA changes among inactive women. Findings from this pilot study suggest that brief PA counseling and a prescription can be effective for improving short-term PA among women. Referring patients to the community program was no more effective than the counseling/prescription alone. More studies with PA objective measures, larger and more representative sample sizes are imperative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.