
Abstract
Introduction
In Kenya, a sub-Saharan African country of nearly 40 million people, patients typically seek care at a local clinic or dispensary and are subsequently referred to provincial or national hospitals, if necessary. Currently, because of unequal distribution of limited health professionals, many sick individuals living in rural Kenyan areas must travel long distances to reach a dispensary (the most basic level of care available in Kenya) for a face-to-face consultation (FTF).1,2 The cost of transportation can amount to almost a day’s income, not including the income lost from missed work.3,4 The price barrier alone results in many individuals delaying care and only visiting a medical professional when the health problem becomes critical. For certain health conditions and diseases, early intervention decreases the cost of treatment and drastically improves the patient’s prognosis.5,6
Mashavu is a store-and-forward (SAF) telemedicine system operated by community health workers (CHWs) who travel with the system and connect rural patients to nurses (Figure 1). The mobile system is able to collect and send vital statistics, including weight, body temperature, blood pressure, photographs, and basic hygiene information via Internet to a nurse who can then respond with appropriate health advice by Internet, text message, or phone. 7 It does not replace any component of the Kenyan system; instead, it enhances the availability and access to preprimary care within the existing health system. The use of such a telemedicine system also promotes task shifting in a nation with a marked shortage of physicians by enabling patients to receive immediate and low-cost medical feedback from a nurse. 8

Mashavu telemedicine system implementation map
This study quantifies the accuracy and appropriateness of remote diagnoses in the current health infrastructure. Studies testing the reliability of telemedicine studies primarily rely on the comparison of FTF consultations and SAF telemedicine results, which yields a diagnostic agreement range of 64% to 90% interobserver reliability.9,10 Interobserver accuracy is determined by comparing the diagnoses of 2 different health professionals during FTF consultations for the same patient. Conversely, intraobserver reliability is the agreement rate of the health professional’s diagnosis of the same patient during 2 separate occasions with enough time between to eliminate recall bias. There are numerous studies on the reliability and outcomes of numerous medical specialties using telemedicine in developed nations. 11 As a benchmark, the established intraobserver agreement rate for FTF tele-dermatology consultations in North America is approximately 94%. 12 Intraobserver agreement rates in studies similar to this preprimary, developing nation, SAF system were not found.
Although many resource-constrained communities use telemedicine systems,13,14 telemedicine ventures in these developing nations rarely publish patient outcomes because of time and/or financial constraints. 15 Lessons that are published remain piecemeal because they cannot be generalized to all resource-constrained areas. Although each context has unique characteristics that directly affect a system’s capacity to thrive, statistical analysis of system success and published results are extremely valuable because they facilitate the formation of trust among health care professionals who are often reluctant to adopt health care information technology despite its vast potential to solve critical health challenges.16-18
This study evaluates the system’s most basic function, providing the patient with accurate and appropriate health feedback. Accuracy and appropriateness are tested by comparison of telemedicine results with traditional FTF consultation results. In both cases, certified nurses gave advice on how to progress, if necessary, into the Kenyan health system. This ensures that the SAF telemedicine system is at least on par with the traditional alternative. It is essential to ensure that although the system is created for a low-cost, developing nation context, the quality and standard of care received are not compromised when delivered remotely via a telemedicine system.
Methods
This study was conducted in the village of Gatitu, in Kenya where the Mashavu telemedicine system was piloted in May of 2011. The study examined the intraobserver concordance of advice provided by nurses when meeting patients FTF and by using the SAF telemedicine system. In this study, the nurse met with the patient FTF, and 2 days later, was given a copy of the SAF data with the patient’s name removed.
This study compared chief complaint, nurse feedback, and nurse diagnosis. In the traditional FTF manner, the nurse was able to listen to a patient’s chief complaints and inquire about relevant topics. The nurse then verbally provided feedback and diagnosis, which the authors documented. Feedback was organized into 3 categories: visit health care professional immediately, visit health care professional for follow-up, or no additional visits needed. Diagnosis entailed the disease or illness that the nurse believed the patient to have. Later, the nurse received SAF profiles for the same patients and then provided feedback and diagnosis.
When data collection concluded, the nurse and authors determined if chief complaint, feedback, and diagnosis matched under various test conditions. Chief complaint was determined to be matching if the patient complaint involved at least one similar body part or system. Patients complaining of chest pain to the SAF operator and headache during the FTF consultation were determined to be different. Feedback was the same if it belonged to the same category: visit health care professional immediately, visit health care professional for follow-up, or no additional visits needed. Diagnosis was determined to be the same if the same root cause or same disease were mentioned. Synonymous terms were accepted to be the same (eg, hypertension and high blood pressure).This study was approved by local authorities as well as Penn State’s Institutional Review Board. All 102 patients in this study gave their informed consent prior to participating in the study.
Results
FTF Versus SAF: Chief Complaints
Of the 102 patients studied, 81 (79.4%) provided the SAF kiosk operator and the consulting nurse with the same chief complaints (Figure 2). Patients were asked to treat SAF and FTF visits as independent visits; however, they were not explicitly instructed to provide the same complaint to both the CHW and the nurse. Additionally, patients visited the nurse FTF immediately after completing the SAF encounter. The FTF visit may have been misinterpreted as an opportunity to discuss additional complaints, and could have skewed the reliability numbers to be lower than expected. Despite varying chief complaints from the same patient, the nurse was often still able to use information from either the FTF consultation or SAF visit to provide the same recommendation.
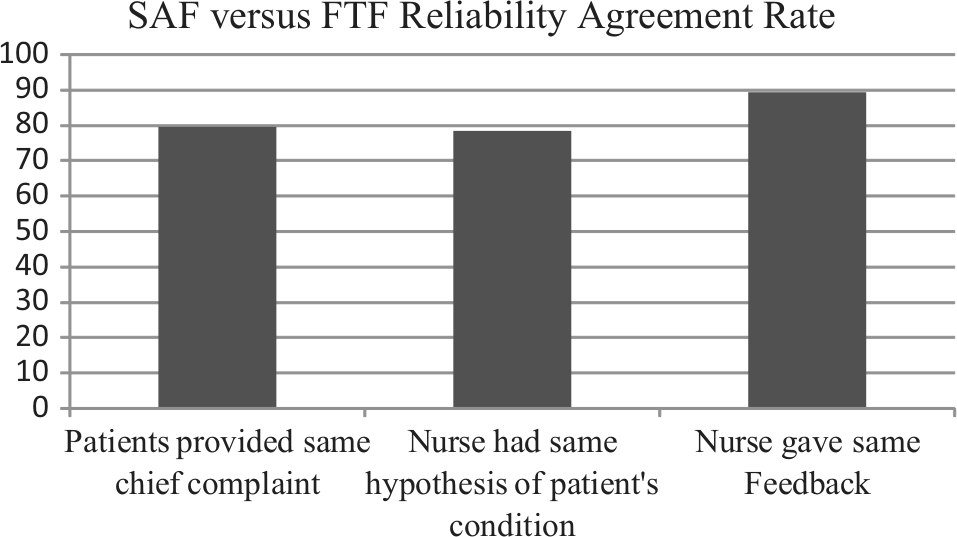
Comparison of the percentage of patients who provided the same chief complaint, nurse’s hypothesis of patient condition, and nurse’s feedback to patients between FTF and SAF
FTF Versus SAF: Diagnosis and Feedback
Regardless of chief complaint similarity or dissimilarity, the nurse had access to the complete SAF profile and arrived at the same hypothesized diagnosis in 80 patients (78.4%) of the total 102 participants (Figure 2). Feedback was often shared with patients only as a nondefinitive diagnosis. Examples include possible parasitic infection requiring stool test; patient is known diabetic, continue clinical follow-ups; or blood pressure within normal range and no further referrals required. In 91 patients (89.2%), the final feedback provided to the patients was the same between SAF and FTF (Figure 2).
Discussion
Value Created by the SAF Telemedicine System
This study supports the notion that nurses, CHWs, as well as patients in Kenya can benefit from SAF telemedicine systems at the preprimary level. Such a system connects rural patients who otherwise may not have the resources to physically travel to the closest health care center. Despite physical distance from the health care professionals, this study has proven that remote consultation with a nurse is able to yield the same advice as a FTF visit in nearly 90% of the consultations (Figure 2). The nurses are able to remotely provide health advice of the same quality and reliability, saving travel time and expenditure for both nurse and patient. Furthermore, the presence of a SAF system in previously inaccessible communities provides jobs for CHWs and also as promotes task shifting and creating more jobs for nurses. 8
Finally, a SAF telemedicine system’s presence in local communities can act as a useful tool for community health workers. The biomedical devices that are integrated into the Mashavu system inspire individuals to take an active interest in their health. Additionally, knowing community health statistics can allow CHWs and patients to better understand the importance of preventative health measures such as lowering sodium levels to prevent common and chronic conditions.
Limitations of This Study
The inherent limitation of this method of study was time did not allow for the proper washout period required for intraobserver studies. Though the name on the SAF telemedicine profile was removed to prevent the nurse from remembering his personal encounter with the patient, and the nurse gave FTF advice to 30 to 40 patients each day, it is still possible that the nurse was able to make the connection between patient and telemedicine profile. To avoid this bias, one could use large numbers of nurses to consult on FTF and large numbers of nurses to consult on the SAF. Practically, however, this would be extremely challenging to accomplish in the Kenyan context, though it would eliminate bias and result in more statistically significant findings. With the available time and resources, the method used in this study was effectively the only way to determine if a nurse would be able to use Mashavu and an FTF consultation in a similar manner.
Limitations of Mashavu Telemedicine System
Telemedicine has a number of inherent limitations such as the inability for the health care provider to personally conduct a physical exam. Though Mashavu has a comprehensive list of questions on its Web application, it is clear that health care providers are better able to freely question the patient and to probe for additional information during FTF consultations.
Apart from the standard and expected limitations of providing remote health care, there were other problems presented by Mashavu that were unique to the system and the location. The system uses CHWs to collect patient information and send it to a nurse. About 1 in 5 patients gave the CHW and nurse different complaints. One of the interviewed nurses believes that this is because of differing levels of trust afforded to a CHW compared with a nurse with a 4-year degree. Another possible reason is the patient’s incorrect assumption that the consultation with the nurse is a follow-up to the SAF consultation.
Another issue was the system’s inability to test for blood sugar glucose/diabetes and malaria, both of which are prevalent in Kenya’s Central and Northern/Western Provinces.3,19 Other features that would enhance the nurse’s ability to provide more accurate feedback include measuring respiration rate and measuring blood pressure twice in the event of suspected hypertension (>150 mm Hg systolic).
Conclusion
This study characterized Mashavu: Networked Health Solutions as a reliable store-and-forward telemedicine system able to provide both economic and social value to rural Kenyans by connecting patients with remote preprimary health care. It was established that the Mashavu telemedicine system’s intraobserver reliability rates correspond to those at established programs in the Western world. Nurses were able to reliably provide rural patients with the same medical advice as if the patient had spent the resources to travel to meet a nurse for a traditional face-to-face consultation. Further studies ensuring the continued reliability and accuracy of the telemedicine system will depend on methods of guaranteeing quality control among the employees.
Footnotes
Authors’ Note
Mashavu is the collaborative work of 234 students from 9 colleges across Penn State over 3 years.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mashavu, the telemedicine system being studied, has received funding support from the National Collegiate Inventors and Innovators Alliance (NCIIA), Clinton Global Initiative University, and private donors.