
Abstract
This study examines the utilization of convenient care clinic services outside of typical physician office hours and estimates the cost savings from potentially avoided visits to the emergency room, urgent care center, and primary care physician associated with convenient care clinic encounters. The results show that 44.6% of convenient care clinic visits occurred on weekdays, 5
Lack of access to health care, particularly after hours and during weekends, presents a barrier to effective and timely treatment for many people in the United States. 1 Only 29% of primary care physicians report having support in place to see patients outside of regular office hours if needed. 2 This often leads to overuse of emergency departments and urgent care facilities for nonurgent medical treatment. 3
Convenient care clinics (CCCs) or retail clinics offer an alternative by typically providing care on a walk-in basis for common, acute, nonurgent illnesses, being generally open during evenings and on weekends.3,4 CCCs provide services that save consumers time 3 and money.5-7 Without retail clinics, patients indicate that they would have delayed care or utilized an emergency room or urgent care center. 8
Since patients use the emergency room as a fallback option for nonurgent care outside of regular business hours of physicians, costs may be significant. According to one estimate, if alternative options were available, cost savings could be as large as $4.4 billion annually. 9
This study examined after-hours and weekend CCC encounters and estimated the cost savings associated with avoidance of visits by CCC patients to the emergency room, urgent care center, and primary care physician.
Methods
This retrospective study examined encounters with CCCs managed by Take Care Health Systems, LLC (Take Care). We assessed the day and time of encounters. Second, we estimated the potential cost savings due to avoidance of visits to the emergency room, urgent care center, and primary care physician.
De-identified encounter data were obtained from the electronic medical record system for the CCCs for all dates of service from January 1, 2007, through December 31, 2009. Encounters in which the patient checked in but elected not to see the clinician and encounters not under the scope of clinic services were excluded. During registration, over 53% of the patients responded to the question “Where would you have gone for care if you did not come to the clinic?” with 4 possible responses: emergency room, urgent care center, primary care physician, or would seek no treatment. These responses served as the basis for estimating potentially avoided visits to the emergency room, urgent care center, and primary care physician, as well as their costs. Given the findings of Mehrotra et al, 6 we used the following benchmark costs as the average visit cost to develop estimates of overall 2007-2009 savings: CCC, $110; emergency room, $570; urgent care center, $156; and primary care physician, $166.
Direct cost savings due to CCCs arise from 3 sources: avoided emergency room, urgent care center, and primary care physician visits. We offset these estimated direct savings with the cost of the CCC encounters themselves, together with the induced costs resulting from CCC visits that occurred as an alternative to no action.
We estimated the number of avoided encounters for each site of service (emergency room, urgent care center, primary care physician), applying the survey percentages to the number of encounters. Different percentages were recorded for encounters during regular hours and after hours. These percentages were applied to the total number of encounters to estimate the number of potentially avoided encounters. Estimated alternative site cost was calculated by applying the benchmark cost per unit of service to the estimated avoided encounters. Net savings was calculated as the estimated alternative site cost less the cost of the clinic encounter. Finally, we subtracted the cost of the induced demand from the overall net savings estimate.
Results
The CCC study population comprised 2 675 303 encounters, consisting of more women than men (60.9%) and patients with an average age of 37. Our analysis found that 44.6% of the CCC encounters occurred on a weekend or on a weekday at or after 5
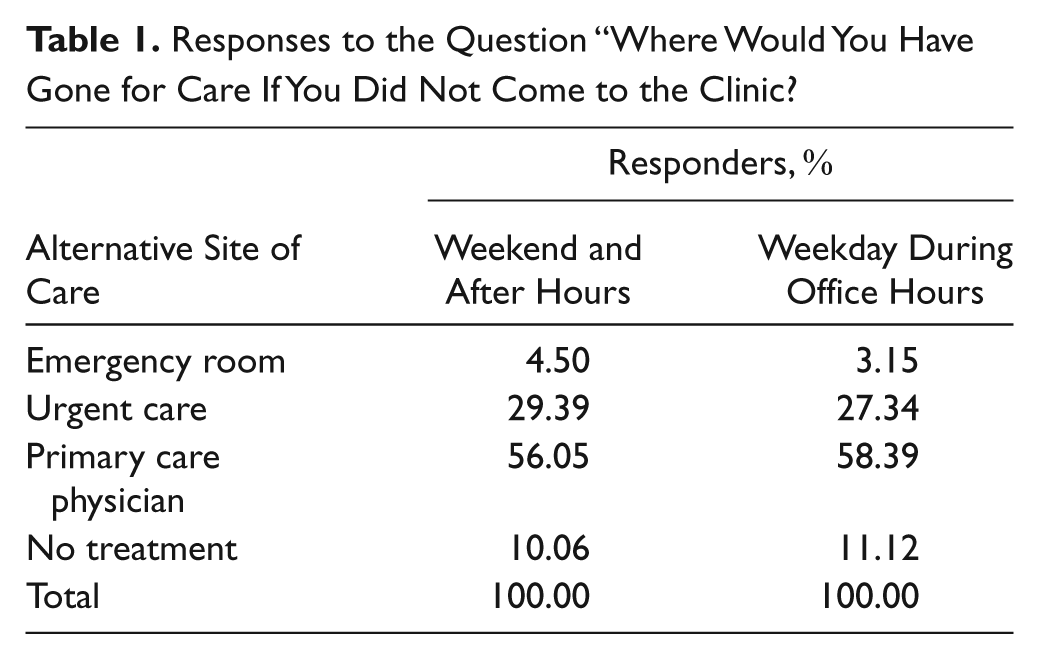
We found that in the absence of CCCs, 4.5% of all patients would have gone to emergency room for weekend and after-hours encounters and 3.15% for weekday encounters during office hours. Equivalent numbers for the urgent care center were 29.39% and 27.34% and, for the primary care physician, 56.05% and 58.39%. Finally, 10.06% would not have sought treatment for weekend and after-hours encounters, and 11.12% would not have sought treatment for weekday encounters during office hours (Table 1). Potential cost savings due to avoidance of a visit to the emergency room, urgent care center, or primary care physician is estimated at $135.53 million (Table 2) or $51 per patient encounter for the encounters examined in this study.
Responses to the Question “Where Would You Have Gone for Care If You Did Not Come to the Clinic?
Estimated Cost Savings, 2007-2009

Discussion
Access to timely care is necessary but often difficult to obtain. 10 Our analysis has several implications. First, almost half of patients are utilizing CCCs on the weekend or on weekdays during evening hours. The ability to see patients outside of typical physician office hours makes CCC clinicians an important extender for physician practices. Second, patients are choosing to visit retail clinics even during office hours. It could be that the patients have started to trust retail clinics more for nonemergency care for minor illnesses. Finally, the ability of CCCs to treat patients with these minor ailments during “off hours” gives patients an alternative to seeking care in more expensive settings. Our results on cost savings due to avoidance of emergency room are consistent with a study by Weinick et al 8 —namely, CCCs can treat an estimated 14% of all patients currently presenting to an emergency room.
Limitations
The results presented in this study are based solely on one CCC network. Other CCC companies and locations may experience different results, making generalization difficult. We have also not attempted to estimate the effect of recidivism or displacement (ie, seeking a subsequent visit somewhere for the same ailment), though Rohrer et al 11 found that retail clinics do not cause displacement. Last, our survey response was limited.
Conclusion
CCCs can be ideal alternative venues for nonurgent care, especially outside of regular physician hours. Many patients indicated that they would have sought treatment at one of these higher-cost sites, if not for the ability to be treated at a CCC. The use of CCCs may therefore result in cost savings for the health care system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors are employed by the Walgreen Co. and the paper is about the work done at one of its subsidiary company (Take Care Health Systems).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the funding for this research came from Walgreen Co.