
Abstract
Objective: To assess the relationship between cognitive decline of older patients (≥ 65 y) and use of primary care physician (PCP) services over 24 months. Design: Retrospective analysis of prospectively collected data from a cluster randomized trial that took place from 2006-2010 and investigated the relationship between formal neuropsychological evaluation and patient outcomes in primary care. Setting: Twenty-four PCPs in 11 practices in southwestern Pennsylvania. Most practices were suburban and included more than 5 PCPs. Participants: A sample of 423 primary care patients 65 years old or older. Measurements: The association between the number of PCP visits and a decline in cognitive status, as determined by multivariable analyses that controlled for patient-level, physician-level, and practice-level factors (eg, patient age, comorbidities, and symptoms of depression; practice location and size; PCP age and sex) and used a linear mixed model with a random intercept to adjust for clustering. Results: Over a 2-year follow-up, 199 patients (47.0%) experienced a decline in cognitive status. Patients with a cognitive decline had a mean of 0.69 more PCP visits than did patients without a cognitive decline (P < .05). Conclusions: Early signs of cognitive decline may be an indicator of greater use of primary care. Given the demographic trends, more PCPs are likely to be needed to meet the increasing needs of the older population.
Introduction
With the aging of the baby boom generation and increases in life expectancy, 1 in 5 persons will be over the age of 65 years by 2030. 1 This demographic shift will be accompanied by an increase in the number of older adults with dementia and complex age-related comorbidities. 2 Currently, dementia affects up to 10% of the population over age 65 and almost half of those over age 85. 3 Mild cognitive impairment (MCI) has been shown to be a strong correlate for the development of dementia, and it is estimated that as many as 25% of adults over age 65 have MCI. 4 Given these estimates, the expected growth in the number of older adults will be accompanied by an increase in the number of visits to primary care physicians (PCPs), who frequently serve as the first point of contact for older adults when memory loss or early signs of dementia are suspected.5,6
The factors that influence use of primary care services among older adults have been examined within the framework of complex age-related comorbidities, such as depression, psychological distress, and multimorbidity. 7 A recent systematic review by Weber et al found 7 studies that investigated the frequency of older adults with dementia visiting a physician in the outpatient setting. 8 The range of visits during a 12-month period across all studies was 2.94-10.18. In each of these studies, the presence of dementia was known and identified by a diagnosis in either the medical chart or an insurance claim. The vast majority of older adults who experience cognitive decline or have cognitive impairment never receive a diagnosis, and if they do, it is late in the disease.9,10 Despite the estimated prevalence of cognitive decline and undocumented cognitive impairment among older adults in primary care, no study has investigated the relationship between cognitive decline and use of primary care services among a sample with undocumented MCI or dementia.
Cognitive impairment is becoming a common presentation in primary care, and it is important to understand the role of PCPs in caring for patients with dementia. Research indicates that PCPs offer higher-quality care and lower costs per Medicare beneficiary than do specialists, 11 yet outpatient services provided in the PCP setting account for only about 9% of total Medicare spending.12,13 Although there have been studies of increased inpatient and outpatient medical service use among elderly patients with dementia and comorbid illnesses, the relationship between cognitive decline and the use of PCP services has not been fully studied.14-16
The purpose of our study was to explore factors driving the use of outpatient PCP services by older patients with cognitive decline. In designing the analysis, we used the Andersen 17 and Fortinsky 6 behavioral models of health service use to guide our selection of factors that are potentially associated with these services. The Andersen model 17 was developed as a conceptual framework to predict and explain different types of health services used by older adults. The model indicates that the health care needs of a patient precipitate the use of services and that patient-related characteristics and conditions (eg, sex, age, and specific needs) contribute to the type and volume of services that a patient uses. The model also acknowledges the importance of external environmental factors (eg, the economic structure of health care or supply-driven variation). In 2001, Fortinsky expanded the Andersen model to address the use of health care by older individuals with cognitive impairment. 6 Fortinsky’s triad model indicates that the level and quality of PCP services used by these individuals could be affected by the ability of PCP practices to recognize psychological and cognitive symptoms in older patients, to treat and manage these symptoms, and to link social and emotional support services for patients and their families. 6
For our study, we hypothesized that patients with a greater decline in cognitive status and more self-reported symptoms of depression over a 24-month study period would have significantly higher use of PCP services, as indicated by the number of PCP visits.
Methods
Our study was a retrospective secondary analysis of data that were prospectively collected during a cluster randomized trial of the relationship between formal neuropsychological evaluation and outcomes of PCP services. The trial was approved by the University of Pittsburgh Institutional Review Board, and all patients provided written informed consent. The details of the trial have previously been reported.18,19
Study Population
The study population of the parent trial consisted of patients who received care from 24 PCPs in 11 PCP practices in southwestern Pennsylvania.18,19 Patients were eligible to participate if they were 65 years or older, did not have a documented diagnosis of dementia, were not acutely ill, and were referred by their PCP. They were excluded if screening by telephone revealed the presence of sensory deficits that would preclude their subsequent testing for cognitive impairment consistent with dementia. Specifically, they were excluded if screening revealed a score of ≤ 18 on the Mini–Mental State Examination.20,21
As part of the parent trial, which took place from 2006-2010, enrolled patients were assigned to a randomization group based on their PCP practice. Of the 11 practices, 6 were randomized to the intervention group, which received a detailed cognitive report of each patient’s performance on a battery of standardized neuropsychological tests, and the remaining 5 were randomized to the usual care group, which did not receive a detailed report.
Of the 533 participants in the parent trial, 423 received a battery of neuropsychological tests at baseline and again at 24-month follow-up. Our study sample consisted of these 423 participants.
Data Collection
From public information sources and data supplied by the office practices, we collected information about office practice location (urban, suburban, or rural) and size (number of physicians). From questionnaires completed by physicians, we gathered data about their age, sex, race, and number of years of practice.
Via patient self-report, we collected sociodemographic information about each participant. This information included age, sex, race, education level, and marital status. At baseline, a registered nurse used a structured chart abstraction procedure to review the medical records of each participant and collect a complete medical problem list that began 2 years before the start of the study. From the outpatient PCP medical records, we collected health insurance information. During the study, we reviewed the outpatient records after each outpatient PCP visit and collected data at 6, 12, and 24 months after baseline. We also collected data about prescription and over-the-counter medications from the medication list in the outpatient medical records, and we confirmed this information by checking the inventory of medication bottles brought by patients to their study appointments. In addition to determining the number of outpatient visits for each patient, we determined the number of emergency department visits and hospital admissions during the 24-month period.
Each patient completed a comprehensive neuropsychological test battery consisting of 14 standard cognitive tests in the domains of memory, executive function, spatial ability, attention/psychomotor speed, and language. The memory tests were the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Word List Learning Test with delayed recall, 22 the Wechsler Memory Scale–Revised Logical Memory I and II, 23 and the modified Rey-Osterrieth figure for immediate and delayed recall. 24 The tests of executive function were the Wechsler Adult Intelligence Scale–Revised (WAIS-R) Backward Digit Span, 25 the controlled oral word association test (FAS), 26 Part B of the Trail-Making Test, 27 the WAIS-R Digit Symbol, 25 and the Clock Drawing Test. 26 The tests of spatial ability were the modified Rey-Osterrieth Copy and the modified WAIS-R Block Design.24,25 The tests of attention/psychomotor speed were the WAIS-R Digit Span Forward 25 and Part A of the Trail-Making Test. 27 The language tests were the Boston Naming Test 28 and semantic fluency (animals) test. 26
To aid in analysis of the findings on neuropsychological tests, we transformed raw test scores to standardized z scores, with negative scores indicating worse performance when compared with the mean. We determined a change (improvement or decline) in cognitive score by subtracting the baseline z score from the 24-month follow-up score.
Of the 423 participants in the sample, 3 had fewer than 3 missing test scores, and there was no pattern to the missing scores. For these participants, we imputed the mean test score of the group that had the same clinically adjudicated diagnosis: normal findings, mild cognitive impairment, or dementia.
To measure depressive symptoms in our sample, each patient completed a modified version of the Center for Epidemiological Studies–Depression (CES-D) Scale 29 during the baseline visit and again at the 24-month follow-up. This instrument asked participants about whether they experienced any of 20 symptoms during the past 2 weeks. They were considered to have depression if they experienced 4 or more of the symptoms at baseline and follow-up or at follow-up alone. The cutoff of 4 was chosen because nearly everyone in the 75th percentile reported experiencing at least 4 symptoms on the CES-D.
Statistical Analyses
First, to summarize the characteristics of the 3 categories of variables (office practices, PCPs, and patients), we used descriptive statistics. Second, to test which variables in the 3 categories were independently predictive of PCP visits, we performed bivariable analyses. In subsequent multivariable analyses, we included all variables that were significant at the level of P < .05 plus variables that previous studies have shown to be relevant to the number of PCP visits. 30 Third, to test whether the number of PCP visits was associated with a decline in cognitive status or the presence of depressive symptoms, we used a linear mixed multivariable model with a random intercept to adjust for the clustering of patients with physicians and for the clustering of physicians within practices. Fourth, to test whether the number of PCP visits was associated with the number of medical comorbidities, we stratified visit frequency by quartile and assessed the distribution of clinical covariates in the upper quartile versus the lower quartile. Finally, to test whether the number of PCP visits was associated with greater overall contact with the health care system, we performed secondary analyses in which we stratified patients by visits to the emergency department (0 vs ≥1 visit) and by hospital admissions (0 vs ≥1 hospitalization) during the 24-month period.
For all multivariable analyses, we used SAS procedure PROC MIXED (SAS/STAT 9.2 software, SAS Institute Inc., Cary, NC, 2008) and considered P values of < .05 to be significant.
Results
Of the patients in the sample, most were seen in suburban office practices that employed more than 5 physicians, and most were seen by male physicians aged 55-69 years old (Table 1). The mean number of study patients per PCP was 17.6 (range, 1-56), and the median number of study patients per office practice was 29.5.
Characteristics of the Sample of 11 Primary Care Practices, 24 Physicians, and 423 Patients
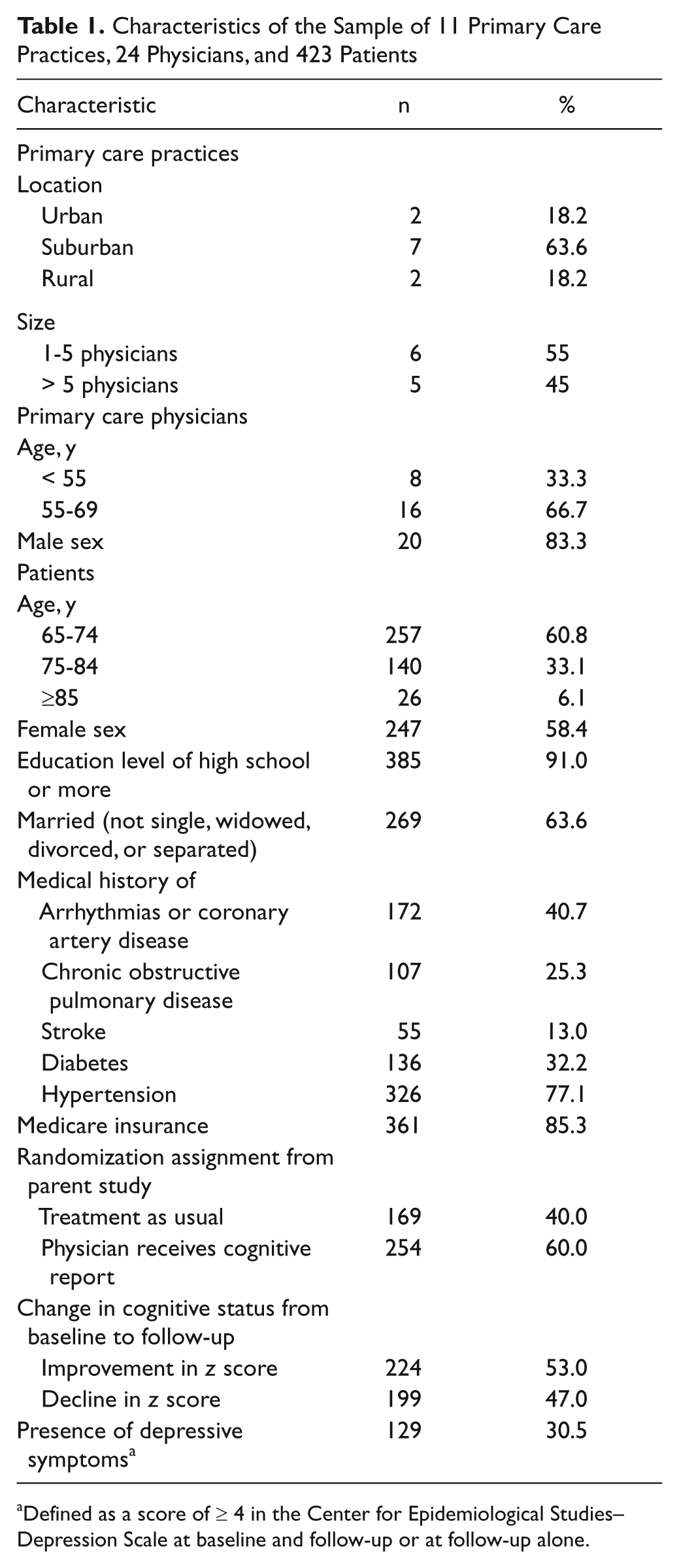
Defined as a score of ≥ 4 in the Center for Epidemiological Studies–Depression Scale at baseline and follow-up or at follow-up alone.
Of the 423 patients, most were 65-74 years old, female, and married, and most had at least a high school education and were Medicare beneficiaries. From baseline to follow-up, 224 patients (53.0%) experienced an improvement in cognitive status and 199 (47.0%) experienced a decline in cognitive status. In total, 129 (30.5%) had depressive symptoms (Table 1).
In primary multivariable analyses (Table 2), the number of PCP visits was associated with 1 practice-level variable (rural practice location) but no physician-level variables. The number of PCP visits was also associated with all of the following patient-level variables: age; education level; history of chronic obstructive pulmonary disease (COPD), stroke, or hypertension; mean number of prescription medicines; cognitive change; and depressive symptoms. On average, patients who had a decline in cognitive status had 0.69 more visits than patients who did not (P < .05), and patients with depressive symptoms had 0.76 more visits than those who did not (P < .05). Similarly, patients who had a history of COPD, stroke, or hypertension had 1.70 more visits (P < .001), 1.43 more visits (P < .01), and 1.21 more visits (P < .01), respectively, than patients who did not.
Results of Multivariable Analyses to Test the Effect of Cognitive Decline on the Number of PCP Visits over a 24-Month Period
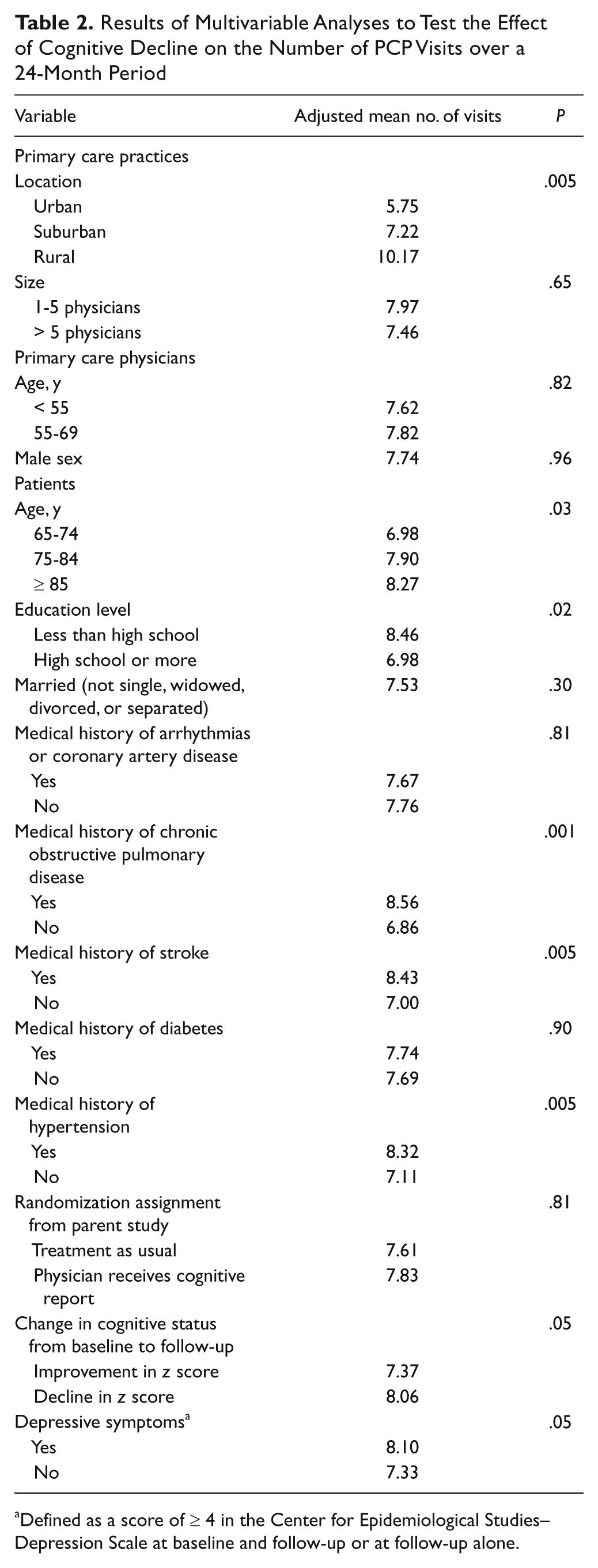
Defined as a score of ≥ 4 in the Center for Epidemiological Studies–Depression Scale at baseline and follow-up or at follow-up alone.
The stratification of visit frequency (not shown) indicated that patients in the upper quartile of comorbidities had a mean of 12.33 PCP visits (SD, 3.74), whereas those in the lower quartile had a mean of 2.85 PCP visits (SD, 1.14). Patients in the upper quartile had a mean number of medical problems of 8.70 (SD, 3.93) and patients in the lower quartile had a mean of 5.87 (SD, 2.59). There was no overall change in the number of medical problems across time. That is, at baseline and 24-month follow-up, patients in the upper quartile had 8.9 and 8.5 medical problems, respectively, whereas those in the lower quartile had 6.4 and 5.3 medical problems, respectively. Thus, a higher frequency of PCP visits was not associated with comorbidities across the 2-year period.
Secondary multivariable analyses (Table 3) indicated that although patients who experienced a cognitive decline had more PCP visits than those who did not experience a cognitive decline, the difference in number of visits was statistically significant only in those who had at least 1 visit to the emergency department during the 24-month period.
Results of Multivariable Analyses to Test the Effect of Cognitive Decline on the Number of PCP Visits Stratified by Emergency Department Visits and Hospital Admissions over a 24-Month Period

Of the 423 patients, 312 had no emergency department visits and 111 had ≥ 1 emergency department visit.
Of the 423 patients, 269 patients had no hospital admissions and 151 had ≥ 1 hospital admission.
Defined as a score of ≥4 in the Center for Epidemiological Studies–Depression Scale at baseline and follow-up or at follow-up alone.
Discussion
In our study of community-dwelling older adults who completed comprehensive neuropsychological testing as part of a clinical trial, we found that a higher number of PCP visits was associated with being in a rural practice and having more medical comorbidity, depression, and cognitive decline over a 24-month period. Moreover, the association between cognitive decline and PCP visits was independent of the burden of depressive symptoms and medical comorbidities. This finding is similar to what Grober et al found regarding Medicare beneficiaries with documented dementia and use of emergency department and inpatient hospitalization. 31
With the focus of United States health policy both on improving access and quality of care and on controlling costs, it is important to understand the factors that are associated with PCP use among older adults. Previous work has demonstrated that patterns of PCP use are influenced by characteristics of PCP practices, physicians, and patients,32,33 and many of our findings are in keeping with these results. Although most older adults in the United States receive health care from a PCP, 32 studies indicate that the current PCP health system is poorly designed to match the needs of older adults with a diagnosis of dementia. 34 Our results indicate that prior to a diagnosis of dementia, when patients are beginning to show signs of cognitive decline, they increase the number of PCP visits. It is possible that in practice, PCPs may be aware of a patient’s changing cognitive status and are using the more frequent PCP encounters as periods of “watchful waiting” with regard to suspicious cognitive symptoms.4,34 In the face of the changing demographics and the expected increase of older adults with dementia, it is necessary for PCPs to have the tools and resources to identify patients with cognitive decline.
The Institute of Medicine recognizes that the patient-clinician relationship is “central to primary care” and “occurs within the context of a personal relationship between patient and clinician that extends beyond an episode of illness.” 35 Our finding that older adults in rural practices tended to have more PCP visits than patients in urban and suburban practices may stem from this type of personal relationship between the physician and the older patient, or even the relationship between the physician and the patient’s caregivers. In contrast to this finding, Mobley and colleagues 36 found that older adults in rural settings tended to have higher rates of hospital admissions for conditions that could have been easily addressed in the outpatient setting. In our study, however, there was a smaller number of patients within the rural subset (42 vs 118 in urban and 263 in suburban subsets), and there were only 2 practices in the rural setting. The fact that the patients in the rural setting had almost twice as many visits as the patients in the other settings is in keeping with the observation of Baldwin and colleagues that rural patients have fewer alternatives for care and use PCP services for both routine and specialized care. 37
Some investigators have found that a higher number of comorbid medical problems in people of all ages increases the number of visits to specialty care physicians, but not to PCPs. 38 In contrast, others have found that a higher number of comorbid medical problems in older adults increases their number of visits to PCPs 39 and that chronic problems are the most frequent reason for older adults to see a PCP. 40 In our sample, we found that several comorbidities (COPD, stroke, and hypertension) were associated with a higher frequency of visits and that the upper quartile of patients with multiple comorbidities had a mean of 8.7 visits over a 24-month period, or roughly 1 visit to a PCP every 3 months. We do not know whether these patients sought additional care from specialty practitioners. We did not find that older adults with a higher number of PCP visits over the 24-month period had any reduction in the overall number of comorbidities recorded in their medical records.
Research concerning educational attainment and health service use has yielded somewhat contradictory results. The majority of older adults in our study sample had at least a high school education, making them more highly educated than the general population of older adults. We found that those with a lower educational status had more frequent visits to their PCP. Although this finding is consistent with studies showing that older adults with a lower educational status are more likely to use community services, such as senior centers, 41 it contradicts previous research showing that more highly educated older adults tend to visit physicians more often. 37 In our sample, the educational level of patients in rural practices was 2 years lower than that of patients in urban and suburban settings, so there may have been some confounding between the level of education and the PCP practice setting.
Depression is known to be both common in older adults and associated with coexisting medical disorders and increased health care use. Baune and colleagues found that depression was associated with a 24%-42% increase in physician visits after taking into account comorbid medical disorders. 42 In our sample, both depression and cognitive decline were predictive of a higher number of PCP visits. Consideration of clinical assessment for both cognition and depression and management would likely help to reduce doctor visits.
Our study has at least 3 limitations that deserve mention. First, we did not have, as part of our study, access to a variable that measured patients’ general propensity to use physician services or any health care service in general. Some studies have shown that psychological distress, 43 somatization, 43 and patient personality traits may play significant roles in the use of health care services. 44
Second, our sample of PCPs and patients were drawn from southwestern Pennsylvania and may not be generalizable to other regions, especially given the documented geographical variation in care. 45 Third, the study did not determine the use of specialty care physicians. The data for our analyses were from a larger randomized trial in which all clinical information was collected from the outpatient chart, which does not consistently note care provided by specialists. Our study was a secondary data analysis of data from a larger trial were not ideally powered, although power calculations revealed that we did have a high probability of observing significant differences between our group with cognitive decline and those without decline. Future work should be directed at teasing out the reasons for visits of the older population who experience a decline to PCPs as well as specialists.
In summary, our study indicates that there is an association between a number of factors and the use of PCP services among older adults: rural practices, certain medical comorbidities, depression, and cognitive decline. Given the demographic trends, more PCPs are likely to be needed to meet the increasing demands of the older population.
Footnotes
Acknowledgements
All authors were responsible for the study concept, design, acquisition of data, analysis and interpretation of data, and preparation of the manuscript. The authors thank Amber E. Barnato, MD, MPH, MS, for her thoughtful reviews of drafts of this manuscript.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant R01 AG023129 from the National Institute on Aging and Eisai Investigator Initiated Study (562-2006). In addition, Dr. Fowler was supported by Grant K12HS019461-01 provided by the Agency for Healthcare Research and Quality to the University of Pittsburgh.