
Abstract
Objectives:
This study tested the feasibility of integrating a virtually facilitated exercise intervention into routine RPM program for older adults to establish its acceptability and patients’ satisfaction.
Methods:
We performed a retrospective analysis of data curated from a population-based virtual exercise intervention for older adults receiving RPM in Ontario, Canada.
Results:
A total of 16 patients participated in at least 1 exercise class, 64% were females, with mean (SD) age of 76 (±10) years. Overall, 100% of participants were “very satisfied” with the program, 81.3% (13) agreed/strongly agreed that the program “motivated them to move,” while 100% (16) agreed/strongly agreed that participating in the intervention has improved their physical endurance. Attendance to the virtual classes were relatively good with patients attending more than 60% of scheduled classes per session. Comorbidity had a strong effect on attendance, with the presence of each additional chronic condition associated with a 15.8% decline in attendance rate (P = .005) over time
Conclusion:
Integrating a virtually facilitated exercise program into routine RPM program for older adults is feasible, acceptable, as well as safe. Larger studies are required to establish efficacy of the intervention in improve health outcomes.
Introduction
Remote patient monitoring (RPM) is an effective tool for managing patients with chronic conditions outside of the clinic or hospital setting, through digital collection data obtained usually in their homes and transmission to central hub for analysis and appropriate response. As RPM becomes widely adopted across health systems, covering a broad segment of the populations, it presents an opportunity for integrating additional interventions for program enrollees; services that they may otherwise not have easy access to, but which would further enhance their clinical outcomes. While layering additional interventions on an existing public health program is not a new concept, such integrated approach is lacking for RPM programs in general, but especially with regards to physical exercise.
RPM programs were originally instituted for the purpose of monitoring patients with chronic or other specific conditions beyond the traditional clinic or hospital setting using technology.1-5 Such programs usually involve remotely tracking metrics such as patient’s vital signs, blood parameters, or other measurable variables and digitally transmitting the results to a central management hub where a management team can access and action them. Over time, RPM programs have been modified to include patient education, case-management and other wrap-around services to enhance adherence and improve clinical outcomes. A Canadian study examined the effect of integrating additional digital therapeutics on regular RPM intervention for patients with heart failure, showing that it led to reduction in all-cause hospitalization compared to those who received RPM only. 6 Zaharieva et al 7 are examining the additional effect of tracking and adding physical activity metrics to algorithm for managing diabetic patients receiving remote care monitoring. Evidence related to integrated virtual exercise for older adults receiving remote monitoring intervention is scarce.
Exercise is known to be effectual in enhancing health among patients living with chronic condition and for preventing diseases among healthy individuals as well.8-17 However, less than 50% of older adults in Canada currently meet the recommended physical activity guidelines for adults aged 65 years and older. 18 There is sufficient evidence that virtually delivered exercise is both feasible and effective19-27 with the potential for supporting isolated older adults to maintain the physical activity levels. 28 Further, home-based exercise programs carried out using digit health innovation (DHI) improves physical function of lower extremity strength and functional capacity, significantly reduces incidence of falls and improves health related quality of life (HRQoL). 29 In addition, in analysis of only older adults with diseases, it also improves the balance and mobility.30,31
Toronto Grace Health Center (TGHC) began implementing an RPM program funded by Ontario Health in 2019 with over 20 000 patients served so far. The TGHC team piloted the integration of an adapted version of a standardized exercise intervention for eligible patients enrolled in the RPM program.
The primary purpose of this study was to examine how feasible it was to implement this integrated virtual exercise intervention, focusing on its acceptability, patients’ attendance rate, and understanding the factors that were associated with any observed outcome.
Methods
We performed a retrospective longitudinal analysis of patients who completed at least 1 exercise class in the integrated virtual exercise intervention for RPM clients between January and November 2024.
The TGHC exercise program including patient satisfaction survey is part of the ongoing RCM program on which the team conducts quality improvement as part of the program management. This manuscript was developed to share findings from one of the quality assurance/quality improvement initiative that sought to further understand and improve the integrated exercise component of the RCM program. For this reason, ethical approval was not specifically sought or needed consistent with Article 2.5 in the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. https://ethics.gc.ca/eng/tcps2-eptc2_2022_chapter2-chapitre2.html#a
TGHC’s RPM program is a publicly funded health program that seeks to mitigate burden on the health system by supporting enrolled patients with smart devices for monitoring as well as responding to their actual or perceived health risks, facilitating aging in place. A comprehensive description of the TGHC’s RPM program can be accessed here. Eligible community-dwelling patients enrolled in the TGHC’s RPM were targeted and encouraged to participate in the virtual exercise program.
To be eligible for the virtual exercise program, a person must be able to; walk at least 10 m independently, with or without a walking aid; follow verbal and visual instructions, and either have access to and be able to navigate the required technology or have a support person who can assist with it. Additionally, participants must be using falls or emergency alert pendant as their smart device in the RCM program. All participants are re-evaluated if they have been absent from the program for a prolonged period due to health conditions or illness, to ensure their continuing eligibility.
To recruit participants, information about the program was shared with healthcare organizations involved in the RCM program through e-blasts, newsletters, and in-person presentations to senior leadership and frontline teams. This was augmented with ongoing monthly newsletters to reinforce program awareness and updates across participating organizations at the local and provincial levels. Healthcare teams at referral organizations used the provided eligibility criteria to screen patients, and those who met the criteria, were flagged on the RCM hub referral form and or an email sent to the TGHC team via email. Received referrals were reviewed by TGHC’s RCM administrators, who then contacted clients, confirmed eligibility, and obtained consent through a waiver. Eligible patients were then enrolled in the program after and provided a technology & safety session.
Data for this study consists of program data collected from participants during the exercise intervention. Further, data from the RPM client intake form containing patient’s baseline socio-demographic and clinical information were curated and linked to the patients’ exercise participation data.
The Intervention
The exercise intervention was based on the adaptation of the Together in Movement and Exercise (TIME) program; a validated group exercise program developed for persons who have challenges with balance and mobility. Enhancements were made to original TIME program, tailoring it to the needs of the RCM population. All participants were required to be enrolled in the RCM program and additional be equipped with the “OdysseyGO” device which is a personal fall and SOS alert pendant. The falls pendant ensures that if there is a safety event, participants are directly connected to support and/emergency services. For sub-acute injuries, the healthcare partners, made up of an interdisciplinary professional team, conduct virtual consultations to facilitate care. The program is offered in a free virtual format allowing participants to engage in exercise regardless of their location within the province, reducing logistical and resources challenges such as arranging transportation to a physical site. A further adaptation of the original TIME program is the allocation of 30 min in the beginning of class for socialization among participants. The intervention is delivered in exercise sessions, each session comprising 6 weeks of twice weekly classes. A new session is started 7 days on the average after the end of the preceding one, unless interrupted by uncontrollable circumstance.
Outcomes of Interest
The primary outcome measure for this study is the rate of adherence to scheduled exercise classes per session. Adherence was operationalized as a continuous variable ranging from 0% to 100%. The program’s attendance list was used to compute the attendance rate for each 6-week session and for participation over time.
The secondary outcomes of the study were; the acceptability, as well as patients’ satisfaction with the intervention. Data used to compute the secondary outcomes was obtained through a structured online survey administered to intervention participants.
Independent Variables
Several patient level variables collected at the time of their referral to the RPM program on the intake form were included as independent variables in the study. They include socio-demographic variables such as age, gender, region of residence, living arrangement, and caregiver status. Other variables such as health diagnosis for disease conditions such as fall, diabetes, dementia, hypertension, etc. were also considered.
Statistical Analysis
We described participants’ adherence rate using percentages of schedule classes attended. Measures of central tendency mean, and median were computed as well.
Using Linear Mixed Model (LMM), we determined the longitudinal change in participants’ attendance rate over time. Both random and fixed effect models were performed to account for potential clustering of adherence rates within an individual as well as within sessions. An initial unconditional means model (UMM) was fit to the data to establish whether a growth model is warranted. From this, an Intra-class Correlation Coefficient (ICC) value >.10 was obtained implying that a Growth model was warranted.
A multivariable LMM was then performed with patients’ adherence rate as the continuous outcome variable. The model converged with only 4 variables included; therefore, we excluded most of the independent variables and retained session ID, comorbidity, age, and gender. Age and gender were retained so they could be adjusted for, comorbidity count because it ranked the highest in effect of all variables for unadjusted model, while session ID was required as a variable in our longitudinal analysis.
Results
A total of 174 potentially eligible RPM patients were referred to receive the exercise intervention, of which only 21 (12%) were successfully enrolled. Only 16 of those enrolled participated in at least 1 exercise session, 64% were females, with mean (SD) age of 76 (±10) years.
Seven virtual exercise sessions were conducted between January and November 2024, each lasting 6 weeks and comprising of twice weekly classes. The total number of sessions attended by each patient were uneven due to the rolling enrollment nature of the program (see chart below). There were no records of dropout from a session associated with inability to tolerate the exercise regimen.

Patient’s Satisfaction
Overall, 100% of 16 surveyed study participants were “very satisfied” with the program and would recommend it to a friend or family. On whether they found the technology for engaging in the virtual exercise easy to use, 43.8% (7) of respondents said that they had no problem, 56.2% (9) said they had initial learning challenge, but which was resolved, and they were able to participate smoothly. On safety concerns, 81.3% (13) strongly agreed that “they felt safer having the RPM
Participation Rate
Attendance to the virtual classes was relatively good with patients attending more than 60% of scheduled classes per session (Figure 1), but notably, individual attendance varied substantially.

Box and whiskers plot showing exercise class attendance rate per session.
The box and whiskers plot above displays overall participation rate for the different exercise sessions showing that there were wide distributions in attendance rate among patients for each session. Table 1 displays the median and mean attendance rate according to sessions attended.
Mean And Median Attendance Rates Per Successive Exercise Class.

We performed an empirical plot of attendance rate as well as its change over time at the individual level to further explore the attendance characteristics (Figure 2).

Empirical plot of change in attendance rate over time for each participant.
The plot showed substantial variations in the baseline as well as trajectory of participation rate between patients.
Trend in participation rates was curvilinear for all evaluated patients, most starting with a high rate (above 60%) and subsequently decreased after 4 to 5 sessions on the average (Figure 2). Only 1 patient started at a lower participation rate and then improved thereafter. Some patients, however, displayed a quick reduction in their participation rate after the first session (Figure 2). The plot of individual trend overlaid on the mean trajectory confirm that most patients start with high attendance rate above the mean and over time maintain this rate (Figure 3).
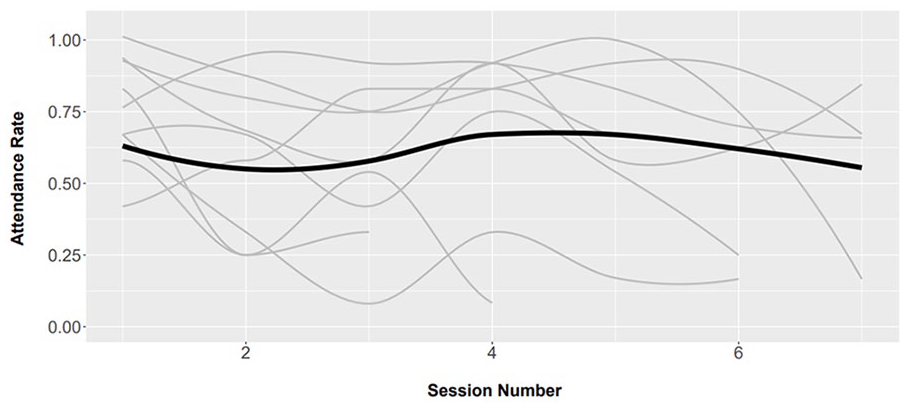
Smoothed individual and mean trajectories of change in exercise class attendance over time.
Multivariable Analysis
The unconditional means model (UMM) generated an ICC of .496 confirming that a mixed model is warranted. However, we fit a random-intercept only UGM next because of the small sample size, which did not allow a random-intercept and slope UGM to be fit to the study data. The UGM generated an intercept of .64 (P < .0001) and an estimate for the session number of −.037 (P = .009), translated to an average baseline participation rate of 64% and a statistically significant negative change in attendance rate over time. The model also showed that the baseline attendance rate (Session 1) is negatively correlated with rate of change over time with the value of −.478.
We fit a multivariable linear mixed model with attendance rate as the outcome, including the maximum number of predictors that allowed reliable convergence given the small sample (n = 16). The final model, selected based on the lowest AIC, included age (centered at 60 years), gender, session number, and comorbidity, chosen for their effect sizes in initial univariate models.
From the results, a 60-year old female patient in the intervention with no comorbidity had an initial attendance rate of 83.6%, P = .000 which subsequently declined on the average by 3.6%, P = .01, after each successive session (Table 2). Comorbidity had the strongest impact on attendance, with the presence of each additional condition associated with a 15.8% decline in attendance rate (P = .005) over time, Figure 4. Among 60-year-old participants with no comorbidity, only age showed a positive association with exercise engagement over time; each additional year of age was linked to a 0.9% increase in attendance over time (P = .11; see Table 2, Figure 4).
Fixed Effects Estimates From Mixed-Effects Model.


Plot of adjusted fixed-effects estimate of selected variables on exercise class attendance.
Discussion
This study examined the feasibility of integrating a standardized virtual exercise program into existing RPM program, looking at acceptability, adherence rate, and understanding patient level factors associated with observed outcomes. Enrolled RPM patients found the virtual exercise intervention very useful, expressed their willingness to continue to participate and to recommend it to others. Adherence to the scheduled exercise classes was good, with an average initial participation rate of 83% for an average 60-year old female with no comorbidity. Adherence rate declined over time by 3.6% per successive sessions, strongly influenced by the presence of comorbidities, and less significantly by age and gender (Table 1).
A major strength of this study is that the analyzed program data was longitudinal which allowed us to examine both baseline engagement rates as well as change in participation rates over time. Applying multi-level modeling analytic method enabled the estimation of how much differences in patients’ characteristics were responsible for the differences in the level of exercise engagement observed at baseline and over time. Collecting and analyzing longitudinal data for this study was important because, future population-based implementation of such intervention will be longitudinal in nature. Therefore, any evidence that supports its scale-up need to reflect this reality.
For many older adults, remaining physical active is a daunting task for many reasons, but chief among which is their inability to physically access an exercise venue. This study illustrates how this barrier may be effectively addressed for an expanding population of older adults receiving remote care monitoring. The findings suggests that it is feasible to provide virtually facilitated exercise for this group, which can be tailored based on patient baseline characteristics. The observed association between patients’ baseline characteristics and adherence rates, as well as the finding that 49.6% of the observed variation in the observed attendance rate was due to difference in person-level characteristics between patients further strengthens the need to tailor exercise intervention. Similarly, the finding of negative correlation between patients’ baseline attendance rate (first session) and their rate of change over time shows that the higher the starting participation rate, the higher the rate of decline in participation rate over time.
The study further highlighted the effect that patients’ characteristics may have on exercise adherence rate, with results suggesting that participation rate is negatively affected by the presence of comorbidity, each additional comorbid condition associated with a 15% decline in participation rate after each successive session (Table 2). This finding aligns with other studies that have reported a substantial reduction in physical activity or exercise with the presence of comorbidity.32,33 Association between comorbidity and lower adherence rate for “synchronous” exercise program is somewhat to be expected since patients living with multiple chronic conditions are more likely be readmitted to hospital, therefore will be more likely to miss scheduled exercise classes while attending clinic appointments or experiencing acute exacerbation of their chronic condition, both of which are likely to prevent consistent participation. Program developers will benefit from utilizing such information to accommodate patients living with multiple morbidities including for instance developing asynchronous exercise classes where possible to allow affected patients to participate at their own time.
Further, exercise class attendance rate was influenced by age, each additional year of life after 60 years associated with 0.9% increase in attendance rate in successive sessions (Table 2). The reason for this surprising finding was not immediately clear but could be due to confounding by variables not included in the model, considering that only 4 variables were included in our analytic model. The finding deviates from current literature showing that exercise participation rate declines with increasing age.34-36 It is worth noting, however, that none of the existing studies examined this trend by integrating virtual exercise into existing RPM program. More studies with larger sample of patients which will allow more variables to be accounted for are therefore required to investigate this finding further.
While the study examined questions related to the feasibility of integrating virtual exercise into RPM program, other questions will require examination. For example, the study did not determine whether such integrated exercise intervention led to any meaningful benefits to the participants and whether, if any, such benefits are affected by the patients’ characteristics. Conducting such study will help policy makers to determine the health and cost benefit of virtual exercise integration within RPM programs and for whom such integration will be most beneficial.
Despite the successful implementation of this pilot study, there were a few challenges with implementing the intervention that are worth mentioning. Although there were over 20 000 RPM program patients to recruit from, only 21 individuals were successfully enrolled in the exercise intervention. The disappointing successful enrollment even among those who were referred (174) was ascribed to factors such as inappropriate referrals, and low awareness about the program. Further, some patients were referred but lost to follow-up before they could be reached by program managers. Enhancing communication with referral site to improve screening and referral practice should be among top priorities for the TGHC’s intervention managers. Demand creation activities should also be integrated into the RPM onboarding process to increase awareness about the program.
Further, aspects of the virtual exercise interventions should be further examined and possibly revised before it can be deployed widely. First, it was not clear how the spacing between successive exercise sessions affected attendance rate. In this study, a session usually began about 7 days after the end of the preceding one. Future studies should examine whether shortening or increasing this interval would improve participation rate. We recommend that a purposefully designed robust trial of this integrated virtual exercise intervention with a larger sample of RPM clients be conducted to generate generalizable evidence of its implementability as well as scalability.
Limitations
One limitation of this study is the very small sample size of the intervention. Only about 16 patients were successfully enrolled in the intervention with only 14 contributing data to the analysis. Therefore, the study lacked power for any meaningful interpretation of the finding beyond the cohort. However, since the objective was to examine feasibility, we are confident that the findings of the study are valid and serves the purpose for which it was designed. Further, only 3 covariates were included in the multivariable analysis, therefore, it is possible that other variables associated with participation in exercise but missing in the model may have influenced the results obtained.
Conclusion
This pilot study demonstrated that a virtually facilitated exercise program is acceptable, as well as safe to be integrated into RPM programs. Most notable among the finding is that participants maintained a reasonable rate of adherence over multiple repeated sessions, suggesting both acceptability and potential for long-term sustainability. Also, with patient characteristics such as the age, gender, and the presence of comorbid conditions shown by the study to influence adherence to exercise intervention, program managers could use such information to tailor their intervention for maximum benefit. A sufficiently powered study will however be required to expand or validate findings of this study, and to establish whether the intervention could lead to significant clinical benefits for recipients.
Footnotes
Acknowledgements
The authors acknowledge Nancy Salbach, PT PhD for her role in creating the TIME at Home pre-recorded videos and Alexandra Chen, MScPT for her role in originating the initial concept that informed the direction of the virtual exercise program at TGHC.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.