
Abstract
Aging in place puts ill and frail older persons in a vulnerable situation, and relatives, especially adult children, are expected to assume caring responsibilities. Healthcare professionals, like homecare nurses, play a key role in providing care to older persons needing support to live at home. However, the quality of primary home care has been questioned. The aim of this study was to describe older persons living at home and their adult children’s lived experiences with caring responsibility assumed by healthcare professionals. We used a reflective lifeworld research approach and analyzed 23 interviews and eight diaries. The COREQ checklist was followed. The findings revealed that caring responsibility is tantamount to being professionally competent and balancing immanent power to either promote or inhibit important areas of the older persons’ and their adult children’s lifeworld. Blurred lines of caring responsibility between the participants, the healthcare professionals, and the healthcare systems occurred and indicated that there were errors of commission and omission regarding the safety of older persons in their own homes.
Introduction
Aging populations with multiple chronic conditions are an important challenge to healthcare systems worldwide. 1 , 2 In Europe, the percentage of people aged over 80 years will increase from 5% in 2016 to 13% in 2070, raising issues of great concern regarding quality of care and soaring healthcare costs. 3 In this age group, many will live with decreasing functional capacity, risk of frailty, and dependency on informal and formal care. 1 , 4 Many will also live alone, which is associated with a heightened risk of unplanned hospitalization 5 and a reduced ability to manage daily living. 6 , 7
Experiencing bodily limitations and frailty leading to loss of independence, growing old with illness has been described by older persons as frightening and evoking feelings of being burdensome. 8 Even so, many wish to remain in their own homes as long as possible. 9 , 10 For many, home is a place offering security, comfort, familiarity, continuity, and unreflective ease. 11 , 12 However, home may turn into a challenging environment, a public arena, when dependency on care and treatment occurs. This may, in turn, make older frail people feel that they have become guests in their own homes. 13
In this vulnerable situation, family, friends, and neighbors 14 , 15 often provide informal care. Adult children in particular play an important role, and due to social norms they are expected to assume caring responsibility and become a supportive resource in their older parent’s life. 16 Assuming informal caring responsibility for their older parent(s), adult children may simultaneously face competing responsibilities, e.g., balancing work, parenting, spousal relationships, or early retirement. 17
In a welfare state like Denmark, adult children could leave all care to the formal healthcare systems. However, they rarely do this because they act as advocates and managers to protect and ensure their parents’ dignity and well-being.18–22 Furthermore, adult children want to reciprocate, expressed as wanting to give back some of the help they received from their parent(s). 22 Caring for an ill older parent causes bodily strain, often referred to as a caregiver burden.23–26 Nevertheless, solidarity between generations, expressed as a willingness to help older persons in need, has gained new ground in the face of public service curtailments. 27
Throughout Europe and in other parts of the world, governments and healthcare providers are engaged in healthcare reforms aimed at improving the quality and safety of care, containing costs, and prioritizing cost-effective interventions. 28 , 29 Thus, the total number of hospital beds has been reduced significantly in many European countries in the face of increased reliance on primary healthcare. 30 Patients are therefore often discharged earlier from hospitals. Hence, the domain of primary healthcare is widening, and its tasks are becoming more complex because multiple health problems requiring advanced competencies are being dealt with simultaneously. 31 , 32 This is also the case in Denmark, where this study was conducted.
Primary healthcare professionals play a key role in assuming responsibility for treatment and care in accordance with current policies and legislation. Nevertheless, threats to the quality of formal care for older persons needing support to live at home, especially after recent hospitalization, have been reported and linked to problems in care delivery, e.g. failure of information transfer, limited skills, unmet needs, and tensions in relationships between older persons, caregivers, and healthcare professionals. 33 , 34 Tensions have also been reported when healthcare professionals thought that caregivers would assume higher levels of responsibility than they actually did because they did not check the caregivers’ willingness or capacity to be involved. 33
Fundamental to our understanding of caring responsibility as exercised by healthcare professionals is insight into elements that ill older persons – and their adult children – experience as essential to be safe and secure while staying in their own homes, and whether such caring responsibility is actually present. Such knowledge is important for healthcare professionals such as homecare nurses, nursing managers, and policymakers who play a key role in securing the optimal quality of care for older persons.
Phenomenon and aim
The phenomenon analyzed here is caring responsibility as experienced by older persons and their adult children in the context of being cared for at home. We aim to describe insights into older persons’ and their adult children’s lived experiences with caring responsibility as exercised by healthcare professionals in primary healthcare.
Method
Research approach
We conducted a qualitative study inspired by reflective lifeworld research as outlined by Dahlberg and colleagues.35–38 This research draws on phenomenology and the hermeneutic philosophies of Edmund Husserl, Martin Heidegger, Hans-George Gadamer, and Maurice Merleau-Ponty, 35 all of which target the lifeworld, our taken-for-granted world of experience. 36 As researchers, we must question the lifeworld’s taken-for-granted assumptions and practice openness to let the phenomenon show itself more fully. 38 In reflective lifeworld research, this slow process of understanding is called ‘bridling’, and implies ongoing reflection throughout the entire research process. 39 Reflections are directed toward the phenomenon and meanings that emerge in the research process; consequently, these reflections include the researchers’ attention and perceptions. The idea is to let new meanings arise that otherwise might have been clouded by established meanings and the researchers’ preunderstandings, 35 e.g. scientific theories, being healthcare professionals and having (had) older parents ourselves. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used in this research. 40
Context
The context is primary healthcare for older persons in a Danish region with a population of 1.2 million, where primary healthcare services encompass the general practitioner (GP), home care, and homecare nursing. The healthcare systems in Denmark are publicly funded services based on free and equal access to healthcare. 41 Older persons are supposed to contact their GP with all questions related to health and illness. The GP plays an important role as a gatekeeper between the primary and the secondary healthcare systems.
Home care is offered to older persons who live at home but are unable to manage everyday life on their own. Home care is provided by registered social- and healthcare assistants and social- and healthcare helpers.a They are referred to as healthcare assistants in our study. Homecare nursing services, including aids and appliances, are provided when prescribed by a medical doctor or if deemed necessary following assessment of individual needs. Registered nursesb provide treatment and care for temporarily or chronically ill or dying older persons.
Participants
The participants were 11 (five women and six men) older persons aged 81–98 years (mean 88 years) and 12 adult children (six sons and six daughters) who were primary caregivers according to their parent. The older persons were selected at a department of geriatric medicine to which the patients were admitted with acute illness on top of their chronic illnesses. All had high care needs and were entitled to primary healthcare.
We used purposeful sampling 42 with the following inclusion criteria for older persons: 1) older persons with chronic illness, 2) aged 80+ years, 3) living alone, 4) not diagnosed with dementia, 5) had at least one adult child living nearby taking care of his/her parent.
The first author discussed with the nurse caring for the older person in the hospital whether s/he met the inclusion criteria and was well enough to be invited to participate. When the older person agreed to participate, the first author invited (via face-to-face contact or telephone) the adult child whom the parent reported was the primary caregiver.
Participant characteristics are presented in Table 1. Older persons are referred to by pseudonyms and adult children by gender and numbers. Unfortunately, one of the older persons was re-admitted to hospital and passed away before the interview was conducted, but the daughter still wanted to participate.
Participant characteristics.
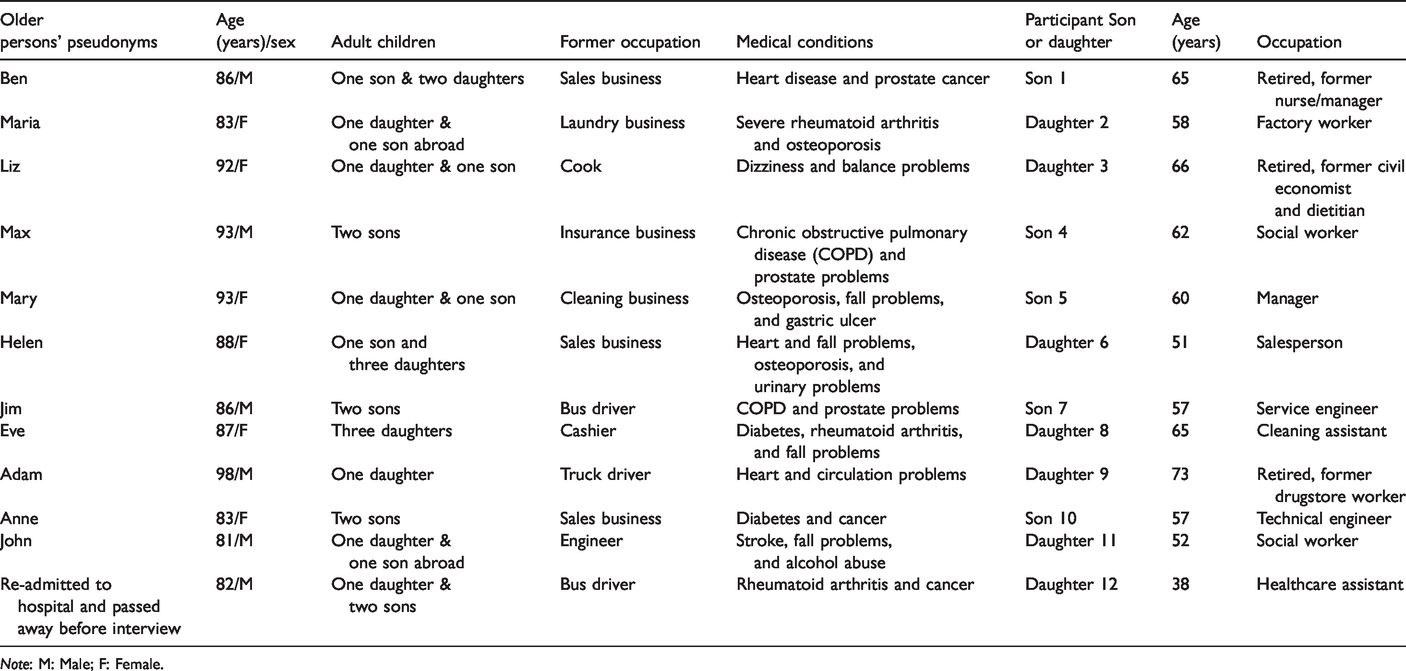
Note: M: Male; F: Female.
Data collection
Data were generated by the first author from January to September 2018. An individual in-depth interview with each of the 11 older persons was conducted 2–3 weeks post discharge, nine in the participant’s home, two in a short-term rehabilitation home. The interviews lasted from 35 to 83 minutes.
Individual in-depth interviews with the 12 adult children were conducted 5–6 weeks after their parent’s discharge. The time and location of the interview were at the adult child’s convenience, resulting in two face-to-face interviews being conducted in the participant’s home and 10 telephone interviews being conducted in the evenings. Interviews lasted 40 to 75 minutes.
Before being interviewed, the adult children completed a two-week diary, allowing them to focus their minds on caring responsibility in different contexts and to report their experiences approximately two to three times a week or shortly after they occurred and undisturbed by the researcher. 35 , 43 , 44 Eight participants completed the diary. The diary length varied, most being a couple of pages long (range 1–20 pages). Four participants did not complete the diary due to a lack of time and because they were distressed.
Interviews were conducted with open-ended questions and a bridled attitude. In the opening phase of the interviews, in an opening question 35 the older persons were asked to describe an ordinary day at home. Both older persons and their adult children were asked to describe their experiences with home care and homecare nursing. To deepen their descriptions and reflections, suggested prompts were asked such as: ‘What happened…?’ ‘What do you mean by…?’ ‘What does it mean to you…?’ 35 , 45 Eight interviews were conducted with the diary notes as starting points. Interviews were audio-recorded and transcribed verbatim by the first author (except two which were transcribed by a secretary). Transcripts included the diary notes.
Ethical considerations
The study was approved by the Danish Data Protection Agency (reference number 2015-57-0066) and designed in accordance with the ethical guidelines for nursing research in the Nordic countries. 46 The participants were informed verbally and in writing and had time to discuss participation before written consent was obtained. Confidentiality and anonymity were secured, specifying the option to withdraw from further participation at any time without consequences for care and treatment. 46
Data analysis
We followed the methodological principles of reflective lifeworld research for descriptive data analysis. 35 , 47 As a part of practicing bridling, we emphasized openness and reflection as a circular process between the whole and the parts, keeping at all times the phenomenon in mind and being careful not to conclude too quickly or too carelessly. In this ongoing bridling process, we asked questions such as: What is it that we understand? Why do we understand it this way? This circular process contained the following phases: 1) All transcripts were read several times to obtain an understanding of the whole. 2) Significant pieces of text, called meaning units, were highlighted and initial thoughts and revelations about the phenomenon were written down. 3) Meaning units that appeared to be related to one another were gathered into ‘clusters’. 4) The clusters were related to each other to find a pattern describing the essential meaning of the phenomenon followed by descriptions of meaning that further constitute the phenomenon. 35 The first author carried out phases 1 and 2 and then discussed phases 3 and 4 with all authors.c
Findings
In accordance with reflective lifeworld research, 35 we first present the essential meaning of the phenomenon of caring responsibility as exercised by healthcare professionals and experienced by older persons and their adult children as ‘a question of being professionally competent’. The phenomenon is further described by four intertwined constituents, allowing more contextual nuances and individual meanings of the phenomenon to surface. The constituents are 1) despite enthusiastic souls – basic human care is not enough, 2) errors of commission in care, 3) errors of omission in care, 4) caught in the Bermuda triangle of healthcare systems.
A question of being professionally competent
Older persons and their adult children appreciate the fact that primary healthcare cares for and to some extent protects the older person from the threats accompanying illness and frailty. The participants feel strongly about the importance of healthcare professionals assuming caring responsibility. In fact, responsibility seems to be the very essence of caring. Caring responsibility is experienced when healthcare professionals act as decent, trustworthy, and committed people who are able to read and acknowledge the older person as an individual in a vulnerable life context with illness and frailty. What is meant here is that caring responsibility is tantamount to being professionally competent and making good judgments, balancing immanent power to either promote or inhibit important areas of the older person’s and their adult children’s lifeworlds. Expectations regarding caring responsibility also involve being able to trust that the agreed-upon care at a system level is provided as professional care and not just as good service.
Nevertheless, blurred lines of caring responsibility appear at both individual and system levels. At the individual level, blurred lines appear between the participants and healthcare professionals when the older person’s expectations and needs are not met and when errors of commission and omission occur. At the individual level, blurred lines also seem to appear between the older persons’ and their adult children’s expectations. Some older persons hesitate to criticize healthcare professionals and seem to accept the situation, relying on further support from their children, while the adult children assume that professional care and responsibility can be improved.
At a system level, blurred lines of caring responsibility appear between the participants and the healthcare systems. Early discharge combined with worries about service levels, lack of competencies and continuity in primary healthcare cause insecurity and uncertainty. Caring responsibility needs to be experienced as being more than basic human care and good service to ensure a feeling of safety and well-being for the ill and frail older person living unattended in her or his home most of the day. The older persons are at the mercy of healthcare professionals and the healthcare systems for care and sustenance. Adult children feel that they have to advocate for the interests of their older parent and be proactive to ensure that their parent receives adequate care and treatment.
Despite enthusiastic souls, basic human care is not enough
The participants described that the majority of healthcare assistants are responsible people capable of providing basic human care, perceived as universal human characteristics such as kindness, warmth, and being positive and interested in the older person’s well-being. It is nice when you are greeted with laughter and ‘How are you?’ You feel a warmth because you are sure it is not something they pretend. (Ben) I do not think they are good enough at observing and interpreting things. Several times, I had to either drive my father to the GP or get the GP to visit him, 10 minutes after home care left the house. That is not very safe. Days when my father is OK, everything goes smoothly and that is super; but when a sudden turn in the road appears and something unforeseen happens, they are not skilled enough to take action. (Son 4)
Errors of commission in care
Both older persons and their adult children experience major quality differences in the care provided by individual caregivers; sometimes resulting in errors of commission, understood as doing something wrong. In general, healthcare professionals are perceived as trustworthy and competent people. Nevertheless, the participants also describe experiences with, e.g. healthcare assistants who do not know what kind of care they are supposed to provide. The older persons describe how this is frustrating and how they sometimes try to train and advise the staff. A daughter explains her experiences with a healthcare assistant who was supposed to empty her father’s catheter bag but did not know what a catheter was. This healthcare assistant was just a temporary worker ‘coming right off the streets’. The same daughter explains how a healthcare assistant was going to give her father tube feeding without knowing the procedure. The daughter asked if she had tried this before. No, but it could not be that difficult to pour something into a bottle and then give it to him in his tube. (Daughter 11)
Medication is another issue of great concern where errors of commission are experienced, especially in the discharge process because of failure to transfer information. At least twice my father has been discharged with an antibiotic for his pneumonia, but didn’t get it, and the homecare nurse first noticed this 4 days later. (Daughter 9)
Errors of commission due to lack of competence in providing basic and complex care contribute to mistrust. Adult children try to compensate and assume responsibility in situations if they become aware of such errors of commission, even if it is an obvious professional responsibility to handle tube feeding or dispense the right medication, for instance. These experiences with errors of commission cause blurred lines of responsibility and raise concerns, especially among adult children, about their parents’ safety and security.
Errors of omission in care
Concerns are expressed, primarily by adult children, about whether primary healthcare provides sufficient professional care to their ill, older parent. Our data show that caregivers have experienced healthcare assistants offering food and beverages and then hurrying out the door without noticing whether the older person consumes what is being served. Adult children wonder why no effort is being made in regard to providing sufficient nutrition. Some try to compensate for this by preparing small meals and buying food they know their parent prefers. Adult children wonder why rejections are often accepted by healthcare assistants. This is experienced as a non-holistic approach, as the opposite of responsible care; indeed, as errors of omission by failing to do what is right and necessary in such situations. The immanent power is not balanced in the older person’s favor. I have told them that it is very good that they are responsive and listen to what the older persons want. However, if, as professionals, they just listen to what my father verbally expresses, e.g. that he will move from there to there but what he does is nothing, then they must push him a little. That is to be a professional, I would think. (Son 1) I have talked with the homecare nurse a few times, but she does not take the role of observing; she is only there for dosing medicine and ordering the medication for which my father is in short supply. (Son 4) We do not talk about anything at all. (Maria) They do not read the situation. This is misunderstood rehabilitation. (Son 7)
Caught in the Bermuda triangle of healthcare systems
The older persons and their adult children also experience blurred lines of responsibility and accountability within the healthcare systems because of the way they are organized. Metaphorically, some experience this is as being caught in a ‘Bermuda triangle’: between their GP, the hospital, and the municipality. The healthcare systems’ directives and service levels seem to be provider-centered, which leaves little room for consideration of the older person’s well-being and sense of continuity. Feelings of being let down by the healthcare systems produce uncertainty about the decision of the older person regarding staying alone in their own home.
At times, the older person and their adult child may attend a productive discharge meeting with a representative from the municipality at the hospital where future home care and homecare nursing are agreed upon. However, some participants expressed concerns because, in their view, the older person was discharged too early and they fear that home care and homecare nursing cannot handle the caring responsibility. My mother was entitled to a temporary rehabilitation home, but the municipality had no vacancies. Therefore, I think she should have stayed a few more days in the hospital. This discharge was too early. (Daughter 3) In a way, I think I was discharged too early. Just because I can manage things at the hospital, they also think I can do it at home. However, everything is more troublesome when I am home and have to do it myself. (Maria) Sometimes you just have to make a special effort before older persons are discharged because they cannot handle it themselves. Communication is poor. You should not say about people that they do not care, but it is as if they have so much distance. (Son 1) If it were possible that the same healthcare professionals visited my dad, that they knew my dad, then they would also be able to observe that my father is much worse off than yesterday, that something is wrong. If a new employee visits him, s/he will just think that this is probably the way he is and then s/he is out the door again. (Son 4) I think they are very busy, I think so. (Liz) I have been re-admitted to the hospital several times; therefore, my sons and I agreed that home care cannot take care of me … My sons do not think that I can manage at home anymore, and maybe they are right. (Max) Home care cannot deliver the necessary care despite the fine principles of aging in place. My father formulated it quite well … I am not afraid to die, I am afraid of not living, having a life. (Son 1)
Discussion
Caring responsibility appears to be a very complex phenomenon that captures the very essence of care provision. Caring and responsibility have previously been described as two sides of the same coin, highlighting the embedded duty to act in specific ways within a certain area of responsibility. 48
In our study, caring responsibility as exercised by healthcare professionals was described by participants in terms of personal characteristics such as decency, trustworthiness, commitment, and professional competencies, including the ability to read the older person and the situation and make good decisions accordingly. These lived descriptions are in line with previous studies focusing on quality in care.49–52 However, in our study, we also found expressions of the opposite, which blurred the lines of caring responsibility between the participants and healthcare professionals in primary healthcare and between the participants and the healthcare systems. These blurred lines of caring responsibility are incongruent with the commonly shared understanding of quality of care as being safe, effective, patient-centered, timely, equitable, integrated, and efficient. 53
Caring responsibility assumed by healthcare professionals and adult children is evident in many ways, and the older person depends on this. Overall, the participants appreciated the care provided in primary healthcare; however, the responsibility inherent in care became blurred when it did not match the participants’ needs and expectations of professional care; for example, when the older persons tried to train the staff or when the adult children compensated and advocated for the interests of their parent in areas of both basic and complex care.
Caring responsibility for an older parent has previously been described as a ‘condition of life filled with uncertainty’ 22 and is often associated with the concept of ‘caregiver burden’;23–26 however, it is also perceived as meaningful and worthwhile. 54 , 55 In our study, the participants shared responsibility with the healthcare professionals, but concerns were foregrounded, especially in situations where basic care and good service were not enough to secure the well-being and safety of the older person in his or her own home.
The participants pointed to major individual differences in the quality of provided care that sometimes resulted in errors of commission and omission because of limited competencies or failure of information transfer. Errors of commission and omission are often referred to with synonyms such as missed care, care left undone, task incompletion, unmet nursing care needs, and implicit rationing of nursing care. 56 Several studies confirm errors in both hospital settings57–59 and primary healthcare. 33 , 60
The participants (especially the adult children) experienced errors in essential clinical procedures such as tube feeding, monitoring/observation, and medication dispensing, threatening the safety of the older person. These experiences are congruent with those reported in a Norwegian study measuring the competence necessary to provide safe care to frail, older patients among nursing staff in nursing homes and homecare services. This study reveals a large gap between the maximum score and the achieved mean score in areas such as patient observations, advanced procedures, and documentation; the study also indicates that nursing staff as a group do not have sufficient competence to ensure the required care to older patients living with comorbidity and polypharmacy. 60 Medication errors seem to occur frequently in primary healthcare according to the experiences of registered nurses. 61
The relationship with healthcare professionals is another important aspect of caring responsibility. In line with the literature62–65 and policies 53 , 66 emphasizing the importance of person-centered care, the participants in our study appreciated when healthcare professionals acknowledged the older person as an individual in a vulnerable life context. Unfortunately, the opposite was also evident, as reflected in experiences with disinterested healthcare professionals displaying no mindful attention to the situation. Hasty and task-oriented healthcare professionals foster feelings that caring responsibility is exercised as a standard package where the older person is objectified, as a kind of minimum service instead of professional holistic care.
The participants linked caring responsibility with continuity and saw this as a way to strengthen familiarity with the older person and his/her situation. Adult children particularly problematized the fact that lack of continuity made it difficult to observe and intervene adequately in regard to the older person’s health situation. These findings are partly consistent with those reported in a study by Gjevjon et al., 67 stating that older persons did not consider a high number of healthcare professionals to be a problem if they were informed and skilled. However, relatives were more critical of the number of healthcare professionals; still, the overall quality of care was more important.
Being discharged too early was another concern and blurred lines of responsibility as did also the municipalities’ lack of temporary rehabilitation homes. The participants’ fear that home care and homecare nursing could not handle the caring responsibility echoes previous findings, and underpins arguments that discharge and integrated care can be improved if interventions address family inclusion, interdisciplinary communication, and ongoing support after discharge, among others. 68 , 69 Nevertheless, congruent with research by Kristensson et al., 70 our findings show that participants had feelings of being ‘in the hands of the organizations’, which was metaphorically expressed as being caught in a Bermuda triangle between the GP, the hospital, and the municipality. The metaphor of the Bermuda triangle characterized by absence of a holistic view and coordination is well known, 28 and this problem challenges many healthcare systems.
In a welfare state, like Denmark, expectations of professional care and system responsibility may be high; however, in line with a study by Lilleheie et al., 64 the participants also expressed an understanding that healthcare systems were subject to pressure and needed more resources and competencies. The older persons and their adult children seemed to accept living with the consequences of more extensive and complex care and treatment being transferred from hospitals to primary healthcare. Experiences with errors of commission and omission in primary healthcare raise particular concerns about safety and security when being old, ill, and living with frailty in one’s own home.
Strengths and limitations
The strength of our study is that we give a rare voice to a vulnerable group of 80+-year-old persons living alone with illness and frailty and a specific group of relatives: their adult children. Their lifeworld experiences with caring responsibility, as exercised by healthcare professionals, are important because healthcare reforms introduce more extensive and complex care and treatment in primary healthcare. The use of in-depth interviews allowed us to obtain rich lifeworld descriptions, which is a key strength in our study. The variation in the participants’ medical conditions, background, gender, and age increased the richness of our data, which is important in a phenomenological-hermeneutic study.
The limitations are that the participants lacked ethnic and racial diversity, and our study did not include even more vulnerable groups of older persons, namely those without relatives and those diagnosed with dementia. Furthermore, using the diary method to allow adult children to describe their experiences shortly after they occurred was challenged by adult children’s distress and lack of time. Therefore, the diary method should be considered in combination with other methods, such as in-depth interviews.
The majority of adult children preferred a telephone interview in the evening, which prevented use of visual cues. Telephone interviews are often described as being less effective than face-to-face interviews for this reason. 42 However, in our study, telephone interview was chosen by the adult children themselves, presumably because it allowed them to feel relaxed and able to disclose sensitive information such as feelings of appreciation, sadness, and anger. 71 Another limitation is that we did not include the healthcare professionals’ perspectives on caring responsibility. Further investigation is needed to explore their experiences.
Conclusions
Caring responsibility, as exercised by healthcare professionals in primary healthcare and reflected in older persons’ and their adult children’s perspectives, is a phenomenon that carries both positive and negative meanings. Positive aspects are experienced when healthcare professionals act as decent, trustworthy, committed, and competent people able to provide professional care, thus acknowledging the older person as an individual in a vulnerable life context with illness and frailty. Another positive aspect relates to trust in the sense that the agreed-upon care at a system level is provided in the form of professional, qualified care and not just good service.
Negative aspects of caring responsibility surface in the form of problems with insufficient care, sometimes resulting in errors of commission and omission. In such situations, responsibility becomes blurred and the adult children have to compensate to ensure their older parent’s well-being and safety in their own home. Lack of continuity, lack of holistic care, and feelings of being caught in a Bermuda triangle between the GP, the hospital, and the municipality also create blurred lines of responsibility. The older persons have to relate to these blurred lines of responsibility, navigating being dependent on both the healthcare systems, healthcare professionals, and their adult children’s ways of assuming caring responsibility.
Implications
The insights obtained from older persons and their adult children into what is encompassed in the phenomenon of caring responsibility as exercised by healthcare professionals in primary healthcare represent important knowledge for healthcare professionals, nursing managers, and policymakers. After early discharge from the hospital, older persons as well as their adult children want to be able to trust that primary healthcare can handle the caring responsibility and provide safe and secure care. Our study has several implications:
There is a need for education, increased competencies, and more resources in primary healthcare. It is necessary to align expectations in relation to the division of caring responsibility for older persons between their adult children, healthcare professionals, and healthcare systems. We suggest that a caring responsibility agreement be made at the beginning of a care trajectory and as an ongoing process involving those responsible for care to prevent blurred lines. A healthcare professional who knows the older person and his/her situation must be appointed as a proactive contact person.
Footnotes
Acknowledgments
We kindly thank the participants for sharing their experiences, and we extend our gratitude to the staff at the Department of Geriatric Medicine, Odense University Hospital, Denmark, for helping with the recruitment.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.