
Abstract
Cardiovascular disease and cancer are the leading causes of death in the United States, 1 and eating at least 5 servings of fruits and vegetables per day is a recommended practice to reduce risks for these diseases.2-4 Many studies have evaluated fruits and vegetables consumption in relation to the risk of cardiovascular disease and specific cancers,2,5,6 but the fruits and vegetables consumption pattern of persons diagnosed with major chronic diseases has seldom been assessed in large cohort studies. According to Centers for Disease Control and Prevention statistics, chronic diseases account for 70% of all deaths (1.7 million each year) in the United States, and almost half of the US adult population has at least 1 chronic illness. 1 Chronic diseases such as heart disease, cancer, stroke, and arthritis are not the only leading causes of death but also the leading causes of disability. Poor nutrition is considered to be a key predictor of many chronic diseases. 7 Public health researchers have focused energy and efforts in the prevention of such conditions by examining nutrition-related factors.
Fruits and vegetables contain essential vitamins, minerals, and fiber that may help protect one from chronic diseases, and the increased consumption of fruits and vegetables has been reported by researchers as a feasible way to optimize nutrition to reduce chronic disease risks and maximize good health. The recommended amount of 5+ servings of fruits and vegetables per day has been reported to lower the risk of several chronic diseases.2-4 On the contrary, inadequate fruits and vegetables consumption has been associated with nutrient deficiency disorders and increases in the risk of developing a number of chronic diseases. 8
The Healthy People 2010 objectives aimed for at least 75% of Americans to consume the recommended 2 or more daily servings of fruits and for at least 50% of Americans to eat the recommended 3 or more servings of vegetables daily. Currently, an estimated 32.5% of US adults consume fruits 2 or more times per day, and 26.3% consume vege tables 3 or more times per day, which is far below the national objective; fruits and vegetables consumption has been reported as declining in 2009 when compared to 2000. 9 Previous studies have indicated that sociodemographic characteristics are associated with fruits and vegetables consumption8,10-12 in the United States. Other determinants of fruits and vegetables consumption include availability13,14 affordability, 10 taste preferences, 15 cultural preferences, 16 and social conditions such as social relationships and social support.17,18 However, little is known about whether the same association holds true for the people who are diagnosed by their physicians or health care providers as having 1 or more chronic disease.
Studies have noted that coupling advice to increase intake of fruits and vegetables with advice to decrease energy intake is a particularly effective strategy for weight management, 19 and consumption of fruits and vegetables is known to assist in controlling high blood pressure and type 2 diabetes among people with those conditions. 20 As a result, the guidelines for treating some chronic diseases, such as hypertension, include recommending patients to increase consumption of fruits and vegetables as part of nonpharmacological intervention.21,22 Therefore, it is expected that people with chronic diseases would increase their frequency and amount of fruits and vegetables consumption once they visit their providers and may get advice to do so. However, studies on fruits and vegetables consumption patterns among persons with doctor-diagnosed chronic diseases (DDCD) are currently limited.
This study, therefore, examined the association between sociodemographic factors and fruits and vegetables consumption pattern among persons with DDCD and those without any chronic diseases. Furthermore, we evaluated the determinants of fruits and vegetables consumption patterns among persons diagnosed with single, multiple, and any number of chronic diseases.
Methods
Study Population and Data Collection
Data obtained from a cross-sectional, random-digit-dialing (RDD) survey of health status in Houston, Texas, conducted in 2008 were used for this study. The sampling frame for the city of Houston was defined by a list of 85 zip codes, including those falling partially within the city boundaries. Telephone samples were provided by Survey Sampling International, LLC. The survey sample designed to represent all Houston households with telephones was drawn using standard list–assisted RDD methodology from telephone exchanges that serve the Houston area.
Princeton Data Source, a survey research company, was contracted to carry out the telephone interviews. Out of a total of 4064 contacts made, only 1001 surveys were completed. All interviews were conducted and completed within 2 weeks, between July 18 and 31, 2008. A maximum of 7 attempts were made to contact every sampled telephone number at different times of the day, and each number was contacted at least once during working hours. For each household contacted, interviewers asked to speak with the youngest adult male currently at home. If no youngest adult male was available, interviewers asked to speak with the youngest adult female at home. This approach reduces the selection bias of not representing the young population because the younger populations are considered as a hard to reach group. 23 The survey instrument and study protocol were reviewed by the Houston Department of Health and Human Services Internal Review Board and deemed exempt (exemption No. 5).
Fruits and vegetables consumption per day was the main dependent variable used for the current study and was measured with a binary response set of “yes” or “no” to the following question: “on average, do you eat at least 3 to 5 servings of fruits and vegetables per day?” The independent variables examined in the current study included age, gender, education, race/ethnicity, marital status, employment status, insurance status, and presence or absence of chronic disease(s). Fourteen chronic disease types considered in this study include heart attack, heart disease, stroke, arthritis, memory loss, asthma, cancer, high cholesterol, gum disease, swelling of joints, abnormal blood pressure, overweight or obesity, diabetes or high blood sugar, and depression. We asked the respondents if a doctor, nurse, or other health professional had ever told them that they had any of the above-mentioned chronic diseases or conditions. In this study, we use the phrase doctor-diagnosed chronic disease (or DDCD) to refer to any chronic diseases clinically diagnosed by doctor, nurse, or other health professionals.
Statistical Analysis
First, we conducted a bivariate analysis using the χ2 test and compared proportions to determine the association between the various types of chronic diseases reported in our sample, their categories (none, single, and multiple chronic diseases), and fruits and vegetables consumption. Next, we determined the independent associations between chronic diseases types and the sociodemographic characteristics of participants using the χ2 test. Also, we conducted a by-group analysis of fruits and vegetables consumption pattern and DDCD type based on selected sociodemographic characteristics identified as significant in an earlier analysis.
Subsequently, we performed a multivariate logistic regression analysis using sociodemographic characteristics identified a priori as significant in the bivariate analysis in the current study and in the previous study 12 as independent variables. The criterion used for inclusion of these independent variables in the multivariate models was statistical significance at probability level of .10 or less. However, the exception to this criterion was educational level, which although was not significant in the bivariate analysis was forced into the models because it was considered to be epidemiologically important. Using the selected sociodemographic characteristics, 3 independent models (model 1, single; model 2, multiple; model 3, all) were developed to evaluate the covariates of fruits and vegetables consumption in our study population by the different groups. Adjusted odds ratio (AOR) with corresponding 95% confidence intervals were computed for each model. All tests were 2-tailed, with probability value of .05 used as the statistical significance level. The sample sizes varied slightly across both bivariate and multivariate analysis performed due to missing cases and/or nonresponse to certain variables used in a particular analysis. We used Surveyfrequency and Surveylogistic procedures of SAS software, as applicable, in our analyses. These procedures incorporate the effect of sample survey designs, including stratification, clustering, and unequal weighting, into the analyses. All data management and statistical analyses were conducted using SAS software version 9.1.3 (SAS Institute, Cary, North Carolina).
Results
Bivariate Analysis
Table 1 presents the association of DDCD with fruits and vegetables consumption status. In general, we noted that the fruits and vegetables consumption level was low and ranged from 1.7% among those with heart disease to 21.5% among participants diagnosed as having high cholesterol. Significant differences favoring nonconsumption of fruits and vegetables were observed for participants with the following chronic diseases: heart disease (P < .01), arthritis (P < .05), cancer (P < .05), overweight or obesity (P < .05), and chronic disease group (P < .05). However, when DDCD was grouped into 3 categories of none, single, and multiple, we noted that a higher proportion of the participants with multiple diseases consumed fruits and vegetables than did those with single disease (43.0% vs 20.3%).
Fruits and Vegetables Consumption by Chronic Disease Type Among Persons With Doctor-Diagnosed Chronic Diseases

Percentages may not add up to 100% due to rounding; participants who did not respond to a question were not included in the analysis of that question.
Doctor-diagnosed chronic diseases.
Chi-square statistics are based on Rao-Scott modified statistic, which provides a design-based goodness-of-fit test for equal proportions within the group, except for the chronic disease group in which degrees of freedom = 2; all other chronic diseases have degrees of freedom = 1.
P < .01.
P < .05.
The fruits and vegetables consumption pattern of the current study population by sociodemographic characteristics and the response rates have been described in a previous article. 12 The association between sociodemographic characteristics and DDCD in the study population is given in Table 2. There was a tendency for the proportions of DDCD to increase significantly (P < .001) with age until age 65 years and older, especially among participants with multiple diseases. Participants who were 45 to 64 years had the highest proportion of single and multiple DDCD (26.3% vs 43.8%). A comparatively high prevalence of DDCD (P < .0001) was, however, noted among participants who were 18 to 34 years, being 39.2% and 18.4% for single and multiple DDCD, respectively. The DDCD was also significantly (P < .05) associated with race/ethnicity. Whites recorded the highest proportion of DDCD in both the single (37.4%) and multiple (36.7%) disease categories. Participants of Hispanic origin recorded 32.6% and were ranked second to whites for single DDCD, whereas blacks were ranked second to whites for multiple DDCD (Table 2). An assessment of the insurance status of participants indicates that only 17.5% and 5.3% of those with single and multiple DDCD, respectively, had insurance. There was a significant difference (P < .0001) in the employment status of participants by disease category, with 64.7%, 56.8%, and 81.0% of them having single, multiple, and no DDCD, respectively. There were no significant associations found between gender, educational qualification, and marital status and DDCD in our study population.
Distribution of Sociodemographic Characteristics of Participants by Chronic Disease Category

Percentages may not add up to 100% due to rounding; participants who did not respond to a question were not included in the analysis of that question.
Chi-square statistics are based on Rao-Scott modified statistic, which provides a design-based goodness-of-fit test for equal proportions within the group.
P < .0001.
P < .05.
P < .01.
Table 3 presents the results of the association between fruits and vegetables consumption and number of DDCD by selected sociodemographic characteristics. Results indicate that fruits and vegetables consumption patterns in relation to DDCD were inconsistent and varied greatly by the independent variables. Specifically, we noted significant difference in fruits and vegetables consumption pattern only among participants who were 65 years and older (P < .01) and those who were of Hispanic race/ethnicity (P < .05). Fruits and vegetables consumption pattern among people who were 65 years and older was significantly associated with their DDCD status: participants with no, single, and multiple DDCD who consumed fruits and vegetables represented 16.2%, 17.1%, and 66.6%, respectively. Among Hispanics who consumed fruits and vegetables, 17.7% and 25.0% had single and multiple DDCD, respectively, compared to 24.7% and 39.4% who had single and multiple DDCD, respectively, but did not consume fruits and vegetables.
Association Between Fruits and Vegetables Consumption and Number of Chronic Disease Among Persons With Doctor-Diagnosed Chronic Diseases by Selected Sociodemographic Characteristics
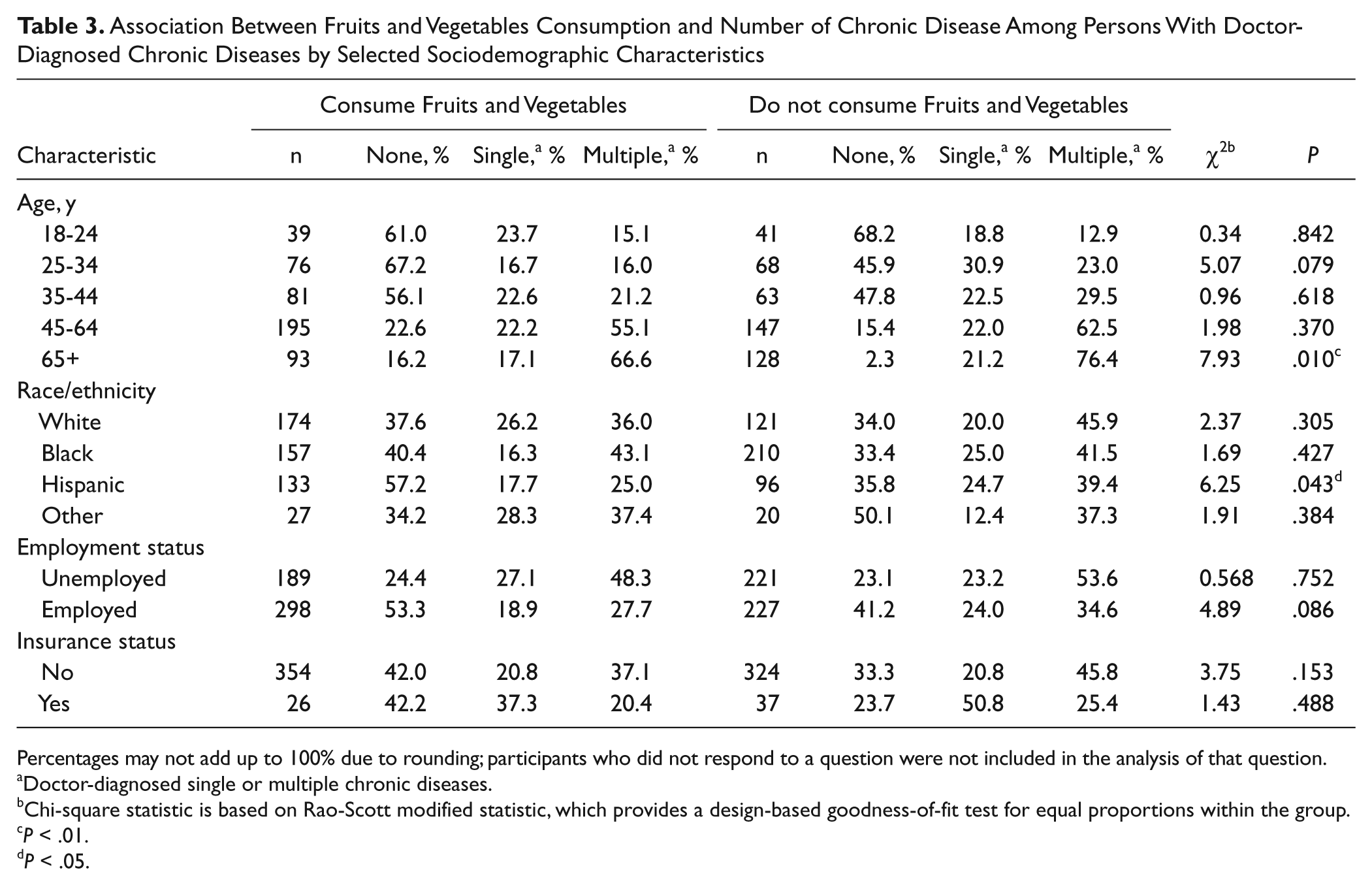
Percentages may not add up to 100% due to rounding; participants who did not respond to a question were not included in the analysis of that question.
Doctor-diagnosed single or multiple chronic diseases.
Chi-square statistic is based on Rao-Scott modified statistic, which provides a design-based goodness-of-fit test for equal proportions within the group.
P < .01.
P < .05.
Multivariate Analysis
The determinants of fruits and vegetables consumption among persons with DDCD are presented in Table 4. Three different multivariate logistic regression models (1-3) were developed based on the predictor variables that met the inclusion criteria by the number of chronic diseases (single, multiple, and all). Findings from our analysis indicate that fruits and vegetables consumption for persons with single chronic disease was significantly predicted (R2 = 0.83) by participants’ age, educational level, and their insurance status, after adjusting for all variables in the model (model 1). Although the consumption levels were generally low comparatively, it was noted that persons with single chronic disease who were aged 35 to 44 years and 45 to 64 years were 94% and 89% less likely, respectively, than was the referent age group to consume fruits and vegetables. Also, persons with the disease who had some college education were similarly 85% less likely to consume fruits and vegetables (P < .05) compared to those who had less than high school education. The results further indicated that those with health insurance were equally less likely to consume fruits and vegetables when compared to those without insurance coverage (AOR, 0.13; P < .01). None of the covariates considered in our current study were significant predictors of fruits and vegetables consumption pattern among persons who had multiple chronic diseases (model 2). However, when the subpopulation with any number and types of chronic diseases was considered (model 3), only gender (P < .05) and marital status (P < .001) were noted as significant predictors of fruits and vegetables consumption (R2 =0.34), after adjusting for all independent variables in the model (model 3). Based on model 3 outcome, participants who were females and married were about twice more likely than were the males and unmarried individuals, respectively, to consume fruits and vegetables (AOR, 1.69; P < .05 vs 2.23; P < .001).
Multivariate Analysis of Determinants of Fruits and Vegetables Consumption Among Persons With Doctor-Diagnosed Chronic Diseases
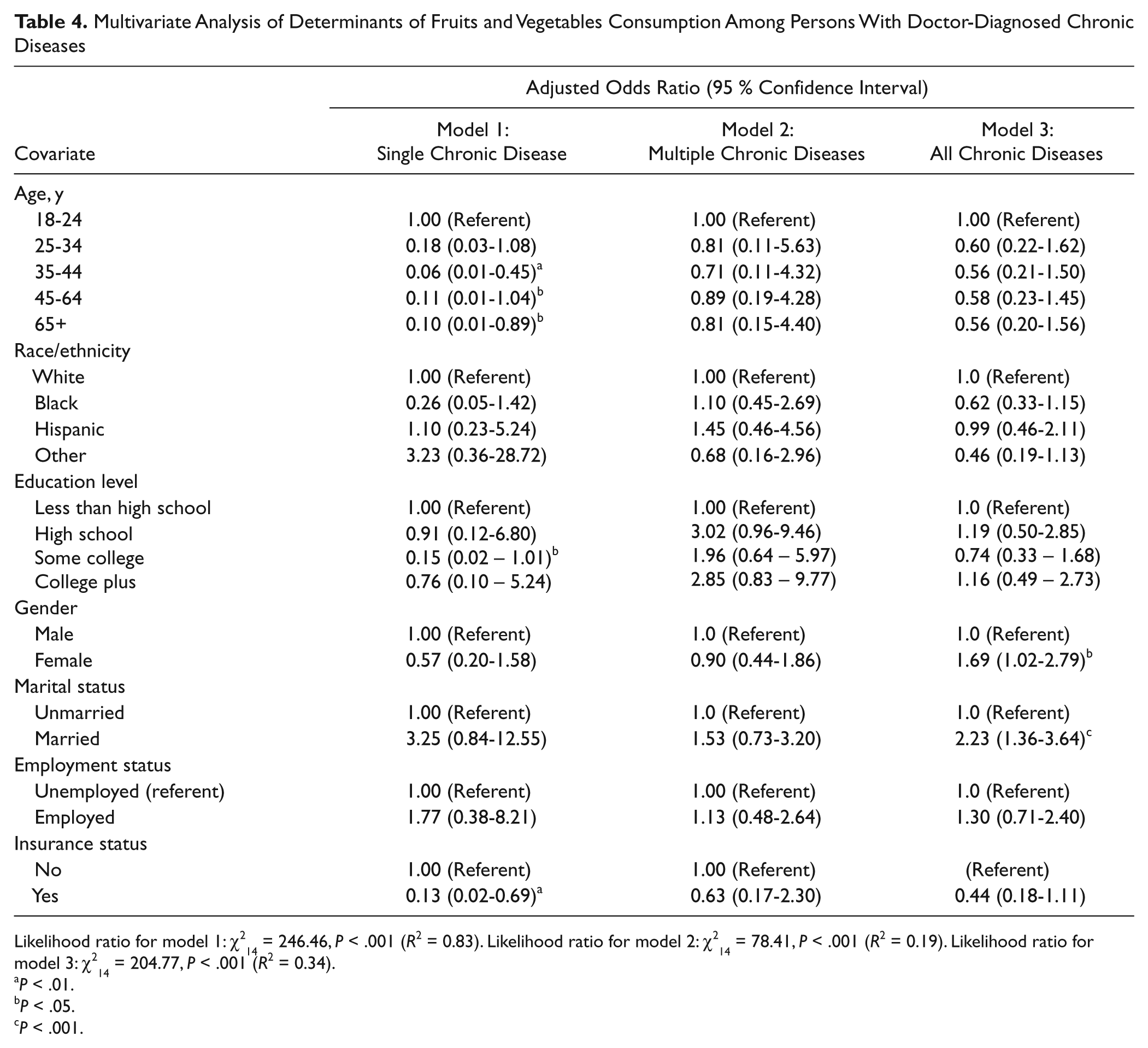
Likelihood ratio for model 1:
P < .01.
P < .05.
P < .001.
Discussion
Despite the growing body of evidence highlighting the protective effects of fruits and vegetables consumption against chronic diseases, their intake is still grossly inadequate in both developed and developing countries. Our study finding that only a small proportion of those with certain chronic diseases (heart disease, arthritis, cancer, and overweight or obesity) consumed fruits and vegetables is important from the public health perspective. This suggests that health education programs may need to pay more attention to the persons with those specific chronic diseases. One of the explanations of such difference could be the functional limitations that the persons with certain chronic diseases experience. Studies have documented functional limitation among persons with multiple chronic diseases.24,25 For example, when an individual is sick with a chronic illness such as arthritis, the person may experience mobility problems, which in turn may affect the fruits and vegetables purchase and consumption. Dependence on others for help with food-related activities of daily living such as grocery shopping and meal preparation can also influence the types of foods consumed by people, 26 including fruits and vegetables.
We also noted that sociodemographic factors, particularly age, race/ethnicity, employment status, and insurance status, were significantly associated with the chronic disease status in the study population. This would suggest that any intervention programs targeted at chronic disease patients should take into consideration these sociodemographic factors.
The finding that the consumption of fruits and vegetables among those who have chronic diseases is lower than for those who do not have diseases presents a unique challenge to the clinicians and public health professionals to effectively address the problem, especially considering that the consumption of fruits and vegetables is associated with decreased risk of obesity and certain chronic diseases. It is also important that any educational approaches that encourage the consumption of fruits and vegetables need to be coupled with a low caloric intake. 19
In the bivariate analysis, we also recorded a low consumption of fruits and vegetables among people who have multiple chronic diseases who were 65 years and older and those who were of Hispanic race/ethnicity. In general, older people have a low perceived benefit and low self-efficacy of consuming fruits and vegetables, 26 which along with several identified barriers may lead to lower consumption of fruits and vegetables, as noted in the present study. Likewise, poor chewing ability, which is common among elderly people, is associated with lower consumption of a range of fruits and vegetables.27,28 The disparity in fruit and vegetable consumption noted among Hispanics who have chronic disease(s) and those without chronic disease would need further investigation to explore the reasons.
When all persons with DDCD were considered (single and multiple DDCD), it was found that marital status and gender were the only predictors of fruits and vegetables consumption. It is believed that when people are living alone, there could be several mechanisms by which the fruits and vegetables consumption patterns can be affected. Researchers have noted that those who cohabit and eat meals with someone at home eat more fruits and vegetables compared to those who eat their meals alone. 29 In addition, persons with DDCD, living alone, may experience more obstacles to purchase and eat fruits and vegetables. Similarly, our finding that more proportions of women consume more fruits and vegetables than do men is in conformity with previous studies.10,30 Donkin et al reported that single men found it more difficult to cook and eat at home than did single women. 31 In general, more women than men perceive fruits and vegetables as healthy foods. 32 This may explain the higher consumption of fruits and vegetables among women than men noted in our study.
Limitations of Study
The findings of this study should be interpreted in the context of a set of potential limitations that we identified. This RDD survey did not include persons without landline telephones or those residing in institutions, so the results might not be representative of certain Houston subpopulations. Generally, the RDD surveys do not have very good response rate, which might result in an overestimation or underestimation of the outcome variable; this study was no exception, as we recorded a response rate of 24.6%. Likewise, it was not possible to include the household income, a key determinant of expenditure level, in our study because of a low response rate. Not including this variable may have had some effect on our findings because demand for fruits and vegetables has been reported to increase with income.10,11,33 Similarly, the availability and accessibility of fruits and vegetables in the study population were not evaluated in this study, which are considered crucial factors of consumption of fruits and vegetables.34-37 Finally, our measure of fruit and vegetable consumption was based on a dichotomous variable, in which we asked whether participants ate 3 to 5 servings of fruits and vegetables per day or not, whereas Healthy People 2010 objectives are based on number of servings per day. In addition, we assume that those who may have consumed more than 5 servings of fruits and vegetables a day have also responded to the question saying “yes.” This difference in intake measurement might lead to misclassification of some participants, resulting in either overestimation or underestimation of persons meeting national fruits and vegetables consumption guidelines. Finally, we examined the fruits and vegetables consumption pattern among persons with DDCD. Consequently, those who may have chronic disease(s) that they are not yet aware of or have not been diagnosed by a doctor or other health professionals were not considered. This may lead to underestimation of the outcome variable.
Implications
Our current study findings, include an earlier one, 12 clearly indicate that consumption of fruits and vegetables is poor among Houstonians with or without chronic diseases. This situation seems to raise some questions, such as why is the consumption of fruits and vegetables so far from ideal levels among Houstonians, and what can be done to improve this situation? What are the factors that shape fruit and vegetable consumption behaviors in the different subpopulation? Although some of these questions may have been addressed partially in the current study, more research is needed to address others.
Given the current understanding that the consumption of recommended amounts of fruits and vegetables helps the chronic disease patients in curbing the progression of illness, 20 it is therefore important that public health practitioners and clinicians, especially those who are working in the chronic disease management field, should emphasize the need for fruits and vegetables consumption among patients with chronic diseases. Although availability and affordability of fruits and vegetables have been reported as key determinants of fruits and vegetables consumption,34-38 improvement in the food environment in certain communities in the Houston metropolitan area may be an effective way to improve access, through which people will make healthful dietary choices that could increase the consumption of fruits and vegetables. Because households that are able to achieve an adequate energy intake are more likely to respond favorably to promotional efforts to encourage and facilitate greater consumption of fruits and vegetables, parallel programs may need to be implemented to alleviate income, price, and availability constraints, which may prevent low-income households from achieving recommended levels of fruits and vegetables consumption. Thus, enactment of policies that can help reduce the market price of fruits and vegetables will have a significant effect on consumption, particularly for low-income households.
However, we cannot ignore the role of access with regard to consumption of fruits and vegetables among people with chronic diseases. This is because people with chronic disease(s) may not be able to access the fruits and vegetables from their neighborhood grocery stores, even if there exists one in close proximity, because of their limitations on daily activities, especially for those who are homebound. Also, considering that about two thirds of the US adult population are overweight or obese, the implications of a diet low in fruits and vegetables are extensive. Convincing evidence already exists for associations between high intake of energy-dense foods, as well as low intake of fruits and vegetables, and obesity and cardiovascular diseases. Consequently, new strategies, in addition to existing campaigns are necessary to help Houstonians, and indeed Americans, make desirable behavioral changes to consume a healthy diet that includes a variety of fruits and vegetables.
Awareness and motivation are equally important determinants of fruits and vegetables consumption. 39 The vast majority of consumers, however, are unaware of the health benefits of consuming fruits and vegetables as a relatively cheap source of essential micronutrients and their protective properties against chronic diseases. Thus, it is imperative that the public health agencies focus on raising awareness and improving perceptions of benefits of consuming fruits and vegetables. Self-efficacy to consume fruits and vegetables is considered as another concern that can be addressed with specific awareness and training among chronic disease patients. Clinicians can play a crucial role in educating their chronic disease patients about the need and importance of consuming fruits and vegetables; however, overburdened schedules may prevent them from fulfilling this role. Home care service providers can also play a vital role in affecting the fruits and vegetables intake of homebound populations with chronic disease(s), if they are provided with the right tools and techniques, by educating their patients about the need of fruits and vegetables consumption. Policy initiatives such as incentivizing larger grocery stores and chain supermarkets to provide their services in low-income neighborhoods can help ensure availability of fruits and vegetables. Furthermore, the food environments could be improved through policy strategies that will encourage local citizens to grow fruits and vegetables at home and the establishment of farmers markets at strategic locations within the city. These public health initiatives could encourage the production and consumption of fruits and vegetables among Houstonians, thereby enhancing the nutritional health benefits of the populace, especially among individuals with chronic diseases. But in general, the success of any of these initiatives will depend on how effectively the main constraints to fruits and vegetables consumption can be addressed.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.