
Abstract
Introduction
In a recent study of health care in the United States over an 11-year period, patients seeking primary care had lower mortality rates than those not receiving primary care. 1 Several factors may account for the beneficial impact of primary care on population health, including greater access to services, better quality of care, greater focus on prevention, early management of health problems, cumulative effect of the main primary care delivery service, and the role of primary care in reducing unnecessary and potentially harmful specialist care. 2
Choosing a primary care physician (PCP) is one of the most important health-related decisions a patient makes. Studies have demonstrated that the ability to choose one’s physician can have a positive impact on patient outcomes by way of increased adherence to prescribed treatment, satisfaction with PCP, and staying with the same physician.3-7
Identifying how patients make their selection will ultimately help PCPs understand what their potential patients view as important to their health care. To date, researchers have identified some factors that appear to influence choice of physician; these factors include the sex and race of the physician, whether the physician was recommended by a friend or family member, the interpersonal skills of the physician, and finally, the perceived competence of the physician.5,8-17
Specialty of the PCP has also been examined in previous studies. In studying which factors influence a patient’s choice of a family practitioner (family medicine [FM]) or a general internist (internal medicine [IM]) as their PCP, Cherkin et al concluded that even if family practitioners and general internists were perceived to have different practice styles, the differing styles were not associated with any differences in patient satisfaction. 18 Stewart et al found that responsiveness, immediacy of care, and personal rapport were important to patients who selected an FM physician. However, these factors were not as important when patients selected internists. Factors that were important for both specialties included the doctor’s willingness to discuss treatment alternatives, being a good listener, and being a doctor who tries to avoid hospitalization. Bernard et al studied patients from both an FM and an IM training continuity clinic located in separate buildings on campus and found that the doctor’s approach to patient care and interpersonal skills/communication were the most important considerations in patient choice of a PCP. They also found that patient knowledge of the difference between an FM and an IM physician in terms of what their training included was poor. Both studies included a predominantly Caucasian patient sample with little racial or ethnic diversity. As such, the generalizeable nature of these findings may be limited to areas with similar demographics and therefore may not be applicable to more urban settings.19,20
The primary objective of this study was to determine whether differences exist among patients in more ethnically diverse FM and IM clinics with regard to the factors reported as important when choosing a PCP. Consideration was given to the impact of various demographics on the ratings of FM versus IM patients. Additional aims included measuring how well patients knew their doctor in terms of training and clinical scope of practice.
Methods
Study Design
This was a cohort study, using self-administered, written questionnaires to obtain information from a convenience sample of primary care patients. Questionnaires were distributed at 2 training clinics (1 IM and 1 FM) over a 2-month period. The clinics were located in the same building. Participants were offered a 4-page questionnaire accompanied by an information sheet when they arrived for their appointment. Those who agreed to participate in the study completed the questionnaire while waiting to be seen for care, and they then gave the completed questionnaires to the nurse or the receptionist. This study was approved by the Institutional Research Review Board for both clinics.
Subjects
Eligible subjects included all adult patients (18 years or older) who came in to see a PCP (who may not have been their PCP) during the study period. Patients were able to refuse participation in the study by returning their blank questionnaire.
Questionnaire
The 3-part questionnaire was formulated using elements from Bernard et al and Bornstein et al,16,20 with modifications to the rating scales (discussed below). First, participants were asked to rate the importance of a variety of factors on their perceived importance in the choice of a physician. A 5-point Likert scale, with answers ranging from strongly disagree (1) to strongly agree (5), was used for each factor; this scale differed from rating scales used by Bernard et al (yes or no) and Bornstein et al (scale of 1–10).16,20 Factors that were provided as choices are listed in Table 1.
Factors or Preferences

Abbreviation: HMO, health maintenance organization.
The second part of the survey measured how well the participants knew their current PCP and whether they knew the differences between FM and IM physicians. Participants were asked whether their PCP was trained in IM or FM; they indicated their understanding of their PCP’s scope of practice by responding to a series of statements related to typical descriptors of internists versus family practitioners. The final portion of the questionnaire collected patient demographic information, including age, sex, marital status, level of education, number and ages of children under the age of 18, and type of insurance. No patient-identifiable information was obtained.
Data Analysis
Data were analyzed using SAS, version 9.1 SAS; Cary, NC; Version 9.1. Comparison of mean scores was conducted using Student t test; chi-square analyses were used to assess associations between categorical variables. Multivariate logistic regression was used to determine what variables were associated with participants’ responses regarding the most important factor affecting their choice of PCP. Results were considered to be statistically significant if P < .05.
Results
There were approximately 3200 patient encounters during the time of this study; 857 patients agreed to participate in the study and completed the questionnaire. Analyses were performed on all measures for which data were available, and n values are reported accordingly. Table 2 summarizes the demographics of the sample population. The majority of participants were female (73.16%) with a significantly higher percentage of females in the FM clinic than the IM clinic (P = .02). The majority of participants were Caucasian, with a substantial number of African American participants (32.17%) represented; the racial distribution for both clinics was similar. In terms of age, the IM clinic participants were generally older; 17.62% were over 70 years old. The IM clinic also had significantly more Medicaid participants and participants with no insurance (P < .001). The majority of the participants in the FM clinic had private insurance (65.96%), whereas 37.67% of IM clinic participants had private insurance. The IM clinic participants generally had fewer years of education; 19.11% of these participants had less than a high school education. The demographic distribution may be related to the fact that the referring hospital directs most of its indigent adult population to the IM clinic for follow-up services. Finally, there were more married participants and participants with children from the FM clinic.
Sample Characteristics

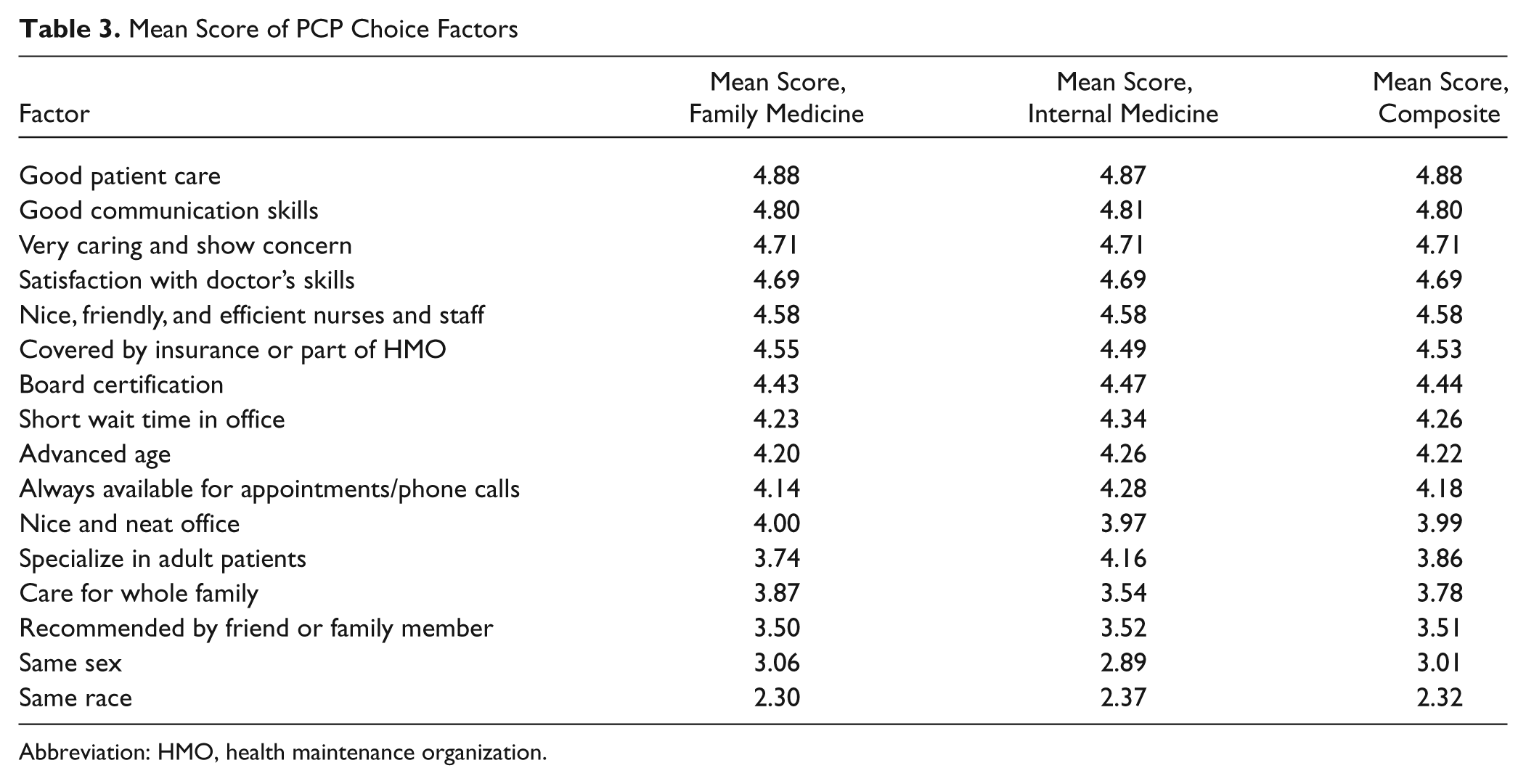
Table 3 shows the mean score for each factor perceived to influence choice of physician. A score of 5 would indicate strong agreement with the item as being important when choosing a PCP; conversely, a score of 1 indicated strong disagreement. Mean scores for each of the factors listed by FM and IM participants were nearly identical; “Good patient care” had the highest average score, followed by “Good communication skills,” and “The doctor’s caring and concern.” The mean scores for the remaining 6 factors, although slightly variable between the groups, are substantively the same for both IM and FM participants. Having a PCP who is the same sex or the same race as the participant received the lowest mean score, indicating that on average, more people felt that these factors were unimportant.
Mean Score of PCP Choice Factors
Abbreviation: HMO, health maintenance organization.
When participants were asked to select the single most important factor among the 16 choices, FM participants most often selected good patient care (19.85%), followed by board certification (17.46%). Among IM participants board certification (21.05%) was selected more frequently compared to good patient care (18.42%). The least important factor for FM and IM participants was the doctor’s race.
In order to determine which, if any, of the demographic variables played a significant role in the perceived importance of factors used when selecting a PCP, a multiple logistic regression was performed for the 3 physician attributes with the highest mean score: good patient care, good communication skills, and very caring and shows concern (Table 4). The regression model included the following demographic variables: age, sex, marital status, presence of children under age 18 in the home, education, health insurance status, and race. The outcome or dependent variable was whether or not the participant had indicated that the physician attribute was the most important factor for them in choosing a PCP.
Regression Modeling for the 3 Physician Attributes with the Highest Mean Score
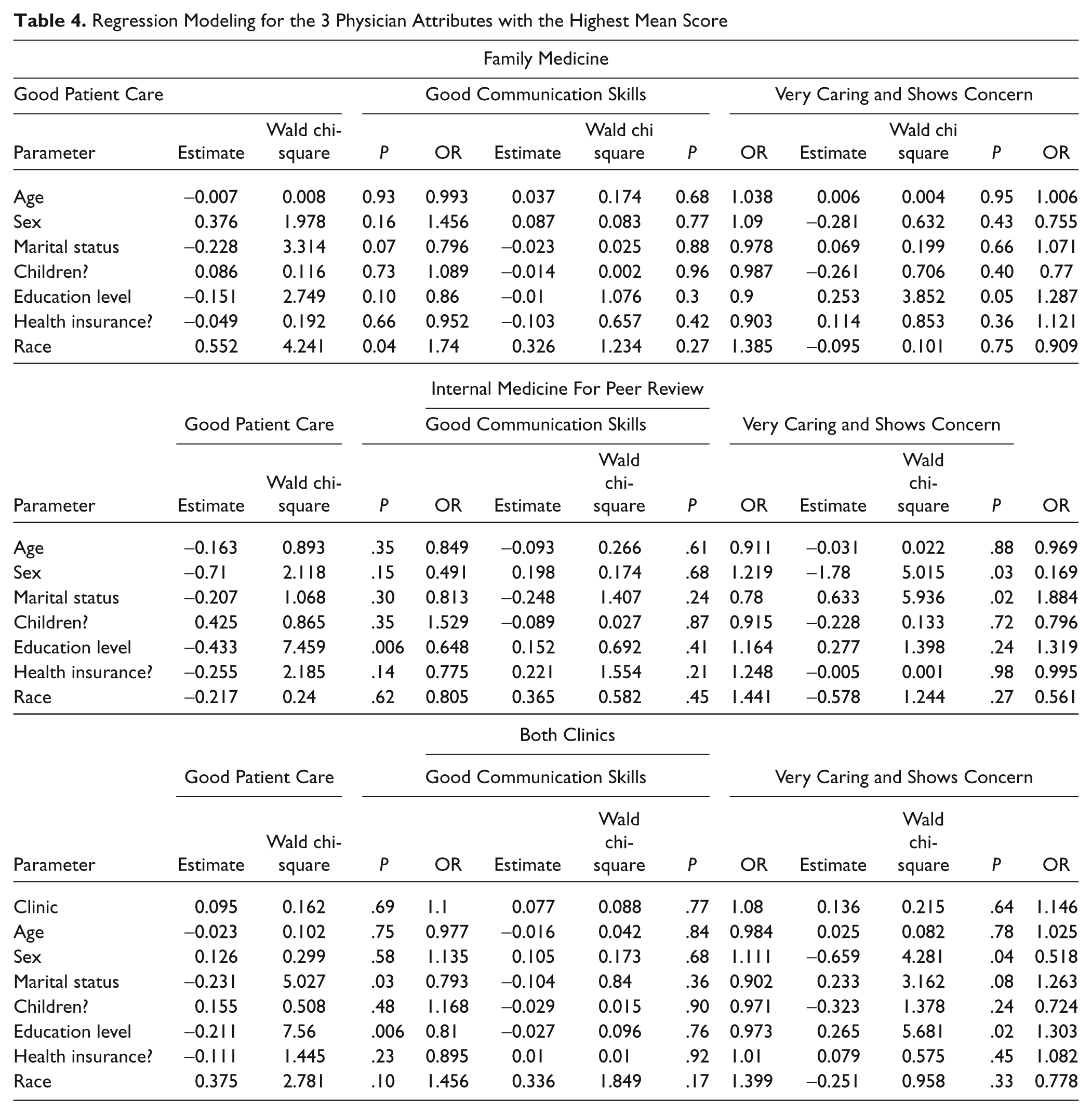
For participants in the FM clinic, race was significantly related to one’s likelihood of ranking good patient care as the most important factor in choosing a PCP. White participants were 74% more likely than nonwhite participants to indicate good patient care as being most important (odds ratio [OR] 1.74, P = .04). No other demographic variables were significantly associated with a greater likelihood of choosing 1 of these top factors as being most important.
Race was not associated with the ranking of 1 of these top 3 factors among IM clinic participants. However, in this group, as years of education decreased, participants were more likely to choose good patient care as the most important factor. For example, participants with a high school diploma were 36% less likely to choose good patient care, compared to those with less than a high school education (OR = 0.648, P = .006). Marital status and sex were associated with the likelihood of participants answering that a physician who is “Very caring and shows concern” was most important to them. Participants who were married were nearly twice as likely to choose this attribute as their top factor for consideration (OR = 1.884, P = .02), compared to those who were not married. Males were over 80% less likely to choose this attribute as their most important consideration, compared to women (OR = 0.169, P = .03).
For the 3 physician attributes with the highest mean score (good patient care, good communication skills, and very caring and shows concern), a regression model that also included clinic yielded significant results for sex, marital status, and education level only; clinic type was not significantly associated with the ranking of the 3 attributes (OR = 1.1, P = .69; OR = 1.08, P = .77; OR = 1.146, P = .64, respectively). Race was no longer related to one’s likelihood of ranking good patient care as the most important factor in choosing a PCP. However, educational level continued to be significantly related to selecting good patient care as an important factor, as it did for IM participants, and marital status was now significantly related to ranking this factor as important when the variable “clinic” was entered into the regression analysis (OR = 0.81, P = .006; OR = 0.793, P = .03, respectively). Further, when the variable “clinic” was considered in the regression analysis, age no longer indicated one’s likelihood of selecting a physician who is very caring or shows concern. Alternately, patient’s sex continued to be related to selecting this factor as important, as it did for IM participants, and educational level was now related to highly ranking a physician who is very caring or shows concern (OR = 0.518, P = .04; OR 1.303, P = .02, respectively).
When participants were asked to identify the specialty of their primary care physician, 48.60% of FM participants did not know whether their doctor trained in FM or IM, and 4.27% answered that they were seeing an internist. Among IM participants, 35.27% did not know whether their doctor was an IM or FM practitioner, and 2.68% answered incorrectly (ie, that their doctor was trained in FM). Similarly, when asked a series of questions about the scope of their PCP’s practice, 50% or more of respondents from each clinic responded that they did not know whether the task listed was something that their PCP was trained to perform. For example, when asked whether their physician could perform minor surgical procedures, more than 90% of respondents replied that they did not know.
Discussion
Overall, results from this study were consistent with past studies reporting factors influencing patient selection of their physician. Good patient care and communication received the highest mean scores in a list of factors that patients may consider in the selection of a PCP.17,19,20 Another factor influencing PCP choice in past studies was board certification. 16 In the current study, board certification was reported as being important to participants, with a mean score of 4.44 (on a scale of 1–5) overall.
When comparing results from FM and IM participants, no significant differences in mean scores assigned to each physician choice factor was observed. That is, the factors with the highest mean scores for participants from both clinics independently were good patient care and communication, which is consistent with previous studies. Family medicine participants most often selected good patient care as the single most important factor irrespective of the list, whereas IM participants selected board certification. This finding was consistent with Bornstein’s study of 636 community participants, in which board certification was also ranked highest.
It was discussed by previous investigators that a more diverse population may have generated a different outcome in factor ranking. This study had a more heterogeneous population with 32% reported as African American (AA), compared to recent studies (15% AA 16 and 2%−3% AA 20 ). However, although our results showed that race, educational status, marital status, and sex each played a significant role in the ranking of an individual factor by FM or IM participants, no significant trends were identified indicating that these demographic factors influence participants’ choices in a consistent manner. This finding lends weight to the conclusion that patients’ perspectives on important factors in choosing a PCP are persistent and consistent across various sectors of the population.
This study demonstrated that a large percentage of participants from both clinics was unaware of whether their PCP was trained in FM or IM. This result was similar to the findings reported in Bernard’s study. 20 This finding was reinforced by the fact that a majority of the participants did not know the scope of practice of their primary care physician.
Our study was limited to adults within 1 health system during a 2-month period who agreed to participate. Although just over 850 surveys from a fairly diverse convenience sample of patients were returned, this number was only 27% of those eligible to respond and may have subsequently skewed the true nature of the parameters studied here. Additionally, a subgroup of the participants in this study may have been assigned to their doctor, which may have influenced the rankings; however, our questionnaire did not capture this information, and therefore it is not possible to quantify this potential confounder.
In summary, despite having a racially diverse population and good patient care, good communication skills and showing concern were still perceived to be important factors to FM and IM patients when selecting an internist or a family physician. Additionally, participants were unable to consistently discriminate the differences between FM and IM. We recommend that PCPs increase their patients’ awareness of their training background and the scope of their practice. Primary care physicians should also be aware of the most important factors that affect patient choice and modify their practices accordingly. Finally, the findings reported here may assist managed care organizations in deciding which provider information should be made available to consumers.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.