
Abstract
Adolescents seek acute care for medical, gynecological, and psychological concerns in the emergency department (ED) that can very well be addressed in a primary care setting. 1 Previous studies have shown that older age, no health insurance, no access to primary care, and rural location contribute to frequent ED utilization by adolescents.2-7 Wilson et al demonstrated that adolescents with high levels of risk behaviors, history of physical or sexual abuse, and higher depression scores were more likely to use the ED as their usual source of care. 6 In fact, these investigators also showed that if adolescents reported the ED as the usual source of health care, they were less likely to have primary care visits and more likely to miss needed care.
Adolescents receive primary care in a variety of venues including general pediatric, family medicine, internal medicine, school-based clinics, and dedicated adolescent practices. Few studies have examined whether the type of primary care setting influences adolescents’ use of the ED for episodic care. Santelli et al found that adolescents attending a school with a school health center had fewer hospitalizations and lower ED usage if they attended school for over a year. 8 A study of school-based clinics versus pediatric hospital–based clinics showed that school-based clinics were more likely to perform counseling and health care maintenance than pediatric clinics but that pediatric clinics were more likely to take care of acute and chronic illnesses. 9 That same study showed that junior and senior high school students in school-based health clinics were less likely to report hospitalizations or have ED visits than similarly aged adolescents in pediatric clinics.
Beyond these investigations, there are few studies comparing adolescent medicine practices providing primary care to general pediatric practices. To our knowledge, there have been no studies to determine whether attendance at an adolescent medicine service, a practice where only adolescents are seen by practitioners who specialize in adolescent medicine, has any influence on ED usage by teenagers. McManus et al examined what practice settings provide optimal primary, behavioral, and reproductive health care for adolescents. 10 Such practices all had availability of all those services at one site, such as school-based health centers, community health centers, special teenage clinics in a group model health maintenance organization (HMO), and hospital-based adolescent medicine clinics. 11 This finding was corroborated by Blum et al, who found that screening adolescents for health risks, both medical and psychosocial, was more likely to be done in a teenage-only clinic than other practice settings. 13 Provision of emergency care was not examined by either McManus et al or Blum et al. The purpose of our study was to compare adolescents’ subsequent health care utilization after an index pediatric emergency department (PED) visit for those receiving primary care in an adolescent medicine ambulatory practice with those receiving primary care in general pediatric settings.
Methods
Patient Recruitment
As part of a larger intervention study, individuals aged 12 to 21 years who were patients of one adolescent medicine practice or 1 of 3 pediatric practices were recruited from among all patients 21 years and younger presenting to a busy, urban PED over a 9-month period. Patients were assigned a triage level on a 1-to-5 scale (1 = most urgent, 5 = least urgent) based upon the nature of the medical complaint and evaluation of the PED triage nurse upon arrival to the PED. A comprehensive information technology system at the study hospital captured utilization data for all patients in the system so that once a patient was identified when presenting to the PED for an index visit, it was possible to track his or her utilization within the system over the succeeding 365 days. Knowledge of patients’ site of primary care was obtained by linking to the name of their identified primary care provider as well as a review of the cumulative visit history indicating attendance at a specific practice over time. The 4 participating practices were chosen because their patients preferentially sought emergency care in this PED, and they represented a variety of characteristics thought to influence the decision of when and where to seek care for episodic illness.
The characteristics of the practices and the number of adolescents seen in these pediatric practices are as follows. The adolescent medicine specialty teaching practice (AMS) is located within a children’s hospital; staffed by board-certified adolescent medicine attending physicians, postdoctoral fellows in adolescent medicine, and pediatric residents; does not have evening or weekend hours; and serves lower income adolescents. One of the pediatric practices is a large academic practice with evening and weekend appointments, situated adjacent to the hospital and serving a socioeconomically disadvantaged population. Another practice is also an academic teaching practice with evening hours available 4 nights per week, serving a population of socioeconomically disadvantaged patients, located at a federally qualified community health center 3.5 miles from the PED. The third pediatric practice is a smaller nonteaching practice with weekend and evening hours, located across the street from the PED, serving middle class families. Patients receiving care at the 3 pediatric practices comprised the non-AMS group of patients. Once all data were collected, personal identifiers were removed from the data set, and the analyses were conducted without these elements. This project was approved by the Montefiore Medical Center Institutional Review Board.
Statistical Analysis
χ2 methods were used to conduct unadjusted comparisons for categorical variables between AMS and non-AMS patients as, for example, in comparing the unadjusted percentage of patients returning within 1 year for a PED, primary care, pediatric subspecialty visit, or hospitalization between the 2 groups. Minimums, maximums, and standard deviations were calculated for all visit types. To estimate odds ratios for fully adjusted multivariate comparisons, we used logit specifications that controlled for age, race, ethnicity, payer status, sex, distance of the primary care practice from the PED, teaching status of the practice, and availability of weekend and after-hour appointments. To test whether the skewness of the visit distributions influenced the findings, we conducted a separate set of regressions dichotomizing the outcome variables to represent the top 5% to 8% of the distribution. Because this specification gave identical results, we elected to present the standard specification for the sake of ease of interpretation. A P value ≤.05 was considered statistically significant. No sample size calculations were conducted, as the investigation included the entire universe of patients from the 4 participating practices who had visited the PED during the study period.
Demographics
Our sample was comprised of 1023 patients between the ages of 12 to 21 years who presented to the PED for inclusion in the larger study. Of these adolescents, 12% were AMS, and 88% received primary care from a non-AMS. There were 77% of AMS patients who were middle or older adolescents (ages 14-21 years) as opposed to the non-AMS group in which 57% of the patients were in that age group.
Table 1 compares the characteristics of adolescent medicine service (AMS) and non-AMS patients. There was a significant difference in gender between the AMS and non-AMS groups, with AMS patients more likely to be female (P < .001). In addition, a greater percentage of AMS patients tended to have public insurance compared with non-AMS patients (52% vs 40%, P = .017). A greater percentage of non-AMS patients had commercial insurance compared to AMS patients (43% vs 31%, P = .010). There was a significant difference in the number of patients who self-identified as white, with 7% AMS and 3% non-AMS (P = .033). There were no other differences in ethnicity between the groups.
Characteristics of Adolescent Patients by Site of Primary Care

Results
In Tables 2 and 3, we summarize unadjusted and adjusted outcomes of different visit types for AMS and non-AMS patients. Table 2 displays proportions of the 2 groups experiencing different visit types as well as mean numbers of visits by group. Table 3 shows adjusted odds ratios of different visit types for AMS compared with non-AMS patients and also indicates the incremental number of visits associated with being an AMS patient controlling for a series of covariates.
Follow-up Visits for Adolescent Medicine Subspecialty Practice (AMS) and Adolescent Patients Seen in Pediatric Practices (non-AMS)

Adjusted Probabilities of Follow-up Visits After Index Pediatric Emergency Department (PED) Visit and Adjusted Incremental Numbers of Visits by Follow-up Visit Type a
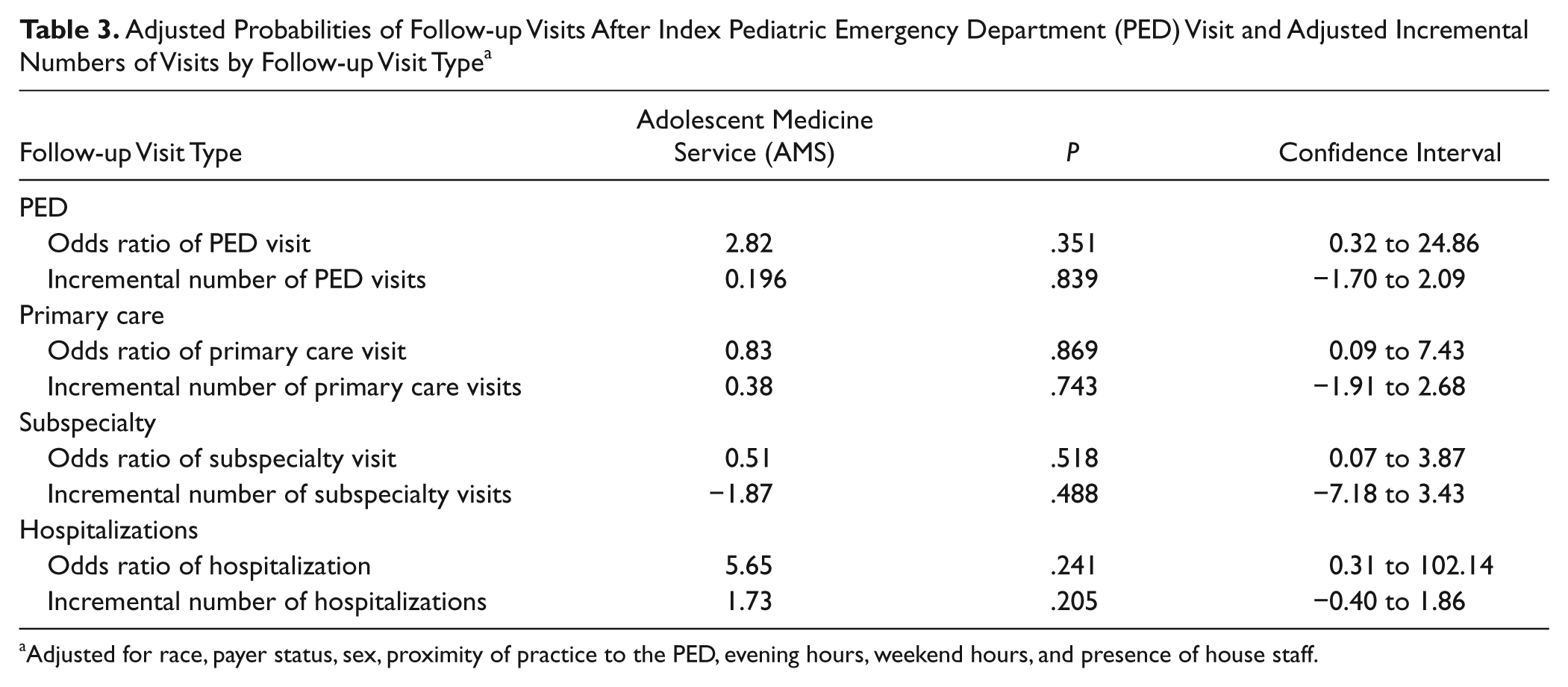
Adjusted for race, payer status, sex, proximity of practice to the PED, evening hours, weekend hours, and presence of house staff.
Follow-up Visits After Index PED Visit
To the PED
Table 2 shows that 46% of AMS and 37% of non-AMS patients registered a return visit to the PED within 1 year of the index visit, a difference that bordered on statistical significance (P = .052). The mean number of return PED visits among the AMS group was 1.35 compared to 0.93 among the non-AMS group, a difference that was significant (P = .026). Multivariate analyses adjusted for race, payer status, sex, proximity of the practice to the PED, presence of residents in the practice, and whether the practice was open on weekends or evenings appear in Table 3. The adjusted odds ratio of having any PED follow-up visit for AMS patients was not significantly different than for non-AMS patients. Similarly, the adjusted odds ratio for incremental number of PED visits also was not statistically significant for AMS compared with non-AMS patients. Analysis revealed that level of triage at the index PED visit and age did not affect the likelihood of a follow-up PED visit for either AMS or non-AMS patients.
To the primary care provider
We found no difference in the experience of AMS and non-AMS patients with respect to frequency or number of follow-up primary care visits in the year following a PED visit. Level of triage at the initial PED visit and age did not affect the likelihood of a follow-up to a primary care provider.
When determining the interval, in days, from the index PED visit to the first follow-up primary care visit, we demonstrated that the mean number of days (adjusted for all the covariates) was 99 days from the index PED visit to a primary care visit. AMS patients returned to the AMS after the index PED visit 24.6 days earlier than other adolescents controlling for covariates (P = .026). Therefore, adolescents who were patients of the AMS were more likely to return sooner for a primary care visit after a PED visit than adolescents cared for in other pediatric practices.
To the pediatric subspecialty clinic
There was no difference between AMS and non-AMS patients with respect to subspecialty utilization in either the unadjusted or the adjusted analyses. Approximately one third of each group returned for a subsequent visit to a pediatric subspecialty practice after an initial PED visit. Level of triage at the initial PED visit and age did not affect the likelihood of a follow-up to a pediatric subspecialty clinic.
Hospitalization
AMS patients were more likely to be hospitalized over the course of the year after the index PED visit compared to non-AMS patients (15% vs 7%, P = .006). Additionally, the mean number of admissions for AMS patients over that year was 0.41, and for non-AMS patients, the mean number was 0.19, a significant difference (P = .048), indicating that the AMS patients were a sicker cohort. These unadjusted results were not supported by the multivariate results. Level of triage at the initial PED visit and age did not affect the likelihood of subsequent hospitalization.
Discussion
This study of adolescents seen in a PED at a children’s hospital demonstrates that patients who attended an AMS appear to be more vulnerable to hospitalization, whether it be due to underlying medical conditions, mental health issues, or gynecological problems as reflected by their greater likelihood of being hospitalized within a year of visiting the PED. This held true even for AMS patients presenting to the initial PED visit with nonemergent triage levels. Additionally, AMS patients were found to return for follow-up to their primary care site sooner than those adolescents attending pediatric practices. These results may be related to the adolescents’ access to their primary care provider. Ryan et al showed that for rural, middle/high school students, having the same provider for preventive and sick care is the most significant predictor of receipt of consistent ambulatory services, rather than episodic health care, provided in an ED. 14 The medical providers of the adolescent medicine practice at our children’s hospital are available to patients every day, 24 hours a day, which is similar to the pediatric practices. However, for the adolescent medicine practice, there is a limited pool of 3 physician providers addressing the emergency concerns of patients after regular practice hours. Patients and families generally know the provider they are speaking to as well as that the provider is an adolescent medicine specialist. Of note, none of the providers in any of the practices involved were aware of the outcome examined, so this would not alter any results. Perhaps the AMS patients feel that they are likely to talk to their usual provider when calling on off hours as well as to have full access to their provider. This possibility is supported by a Kaiser study that compared adolescent patient satisfaction in a teenage clinic versus a general pediatric practice. Teenagers seen in an adolescent clinic were more comfortable discussing sensitive issues with providers than those seen in pediatric clinics. 11
Another possible explanation for the quicker return to primary care for AMS patients is that in the AMS practice, it is generally the patients themselves who present for medical care and speak directly to the provider, not a parent. 10 This is in contrast to the pediatric practices in which adolescents may present for care themselves, as opposed to a pediatric patient who has been followed since birth and has always presented with a parent to rely on to arrange follow-up and attend visits with the teenager. The parent may work or have other daytime responsibilities, making timely follow-up of the adolescent in the general pediatric practice harder to arrange. This is supported in our study by the fact that over three quarters of AMS patients were 15 years or older, as opposed to non-AMS patients in which half were under 15 years. There were 51% of AMS patients who were over the age of 18 years, whereas only 21% of non-AMS patients were over 18 years. Elements of the provision of care to adolescents in a setting with adolescent medicine–trained providers should be examined further, as our data illustrate that this type of practice setting results in quicker follow-up to primary care after a PED visit.
Our findings also showed that attending an AMS predicted increased likelihood of a future PED visit. The fact that adolescents were more likely to return to the PED after the index visit if they were followed in an AMS may be because AMS patients were more likely to be hospitalized and have a greater number of admissions than non-AMS patients. Perhaps AMS patients needed to return to the PED, as hospitalization was necessary, even though, as our data illustrate, the adolescents may have been assigned a nonurgent triage level at the initial PED visit that led to the hospitalization. based in children’s hospitals generally see a sicker cohort of patients, as does the practice in this study, because many patients are referred to the AMS for their primary and gynecological care by subspecialists who care for adolescents with chronic illnesses. This study suggests that having an adolescent medicine practice in a children’s hospital that provides primary care for adolescents with chronic illnesses served by the subspecialty practices within that hospital is very important, as adolescents seen in the adolescent medicine practice are well connected to primary care and return to their primary care provider in a timely fashion.
This study suggests that attending an adolescent medicine practice generally translates to an earlier return to the primary care site after the initial ED visit. However, the number of AMS practices in this country is small. Most practices that focus on adolescent care exclusively are generally available to adolescent patients who receive care in academic pediatric or family medicine centers, school-based health centers, or community health centers. 10
Although our study did not examine the diagnoses for the adolescent patients who had a PED visit, adolescents generally visit the ED for reasons related to risk behaviors such as injuries and gynecological problems.1,4,7 This could also explain why adolescents in our study returned more quickly to their primary care provider if they were AMS patients in which such health challenges are addressed at every visit. 12 A limitation of this study is that it took place at a specific urban children’s hospital PED. Patients who attended the 4 practices who had emergent medical problems may have been taken to an ED closer to home in which case we would not have captured that visit, leading to a potential undercounting of follow-up PED visits by the patients in this study.
Adolescents attending an adolescent medicine practice for primary care had a shorter interval between the PED visit and return to follow-up for primary care. This study cohort was more likely to be hospitalized after initial PED visits. Studies that examine a greater number of adolescent patients, in a wider array of primary care settings, are warranted to determine whether adolescent medicine practices have unique qualities that promote such patient behavior.
Footnotes
This information was presented, in part, at the Pediatric Academic Society Meetings, May, 2007, Toronto Canada.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article. The study was supported, in part, by the Commonwealth Foundation, NYC, Grant #20040852.