
Abstract
Access to primary health care services is a growing concern in Canada and other developed nations.1-4 Media reports continue to reinforce the public’s awareness and concern regarding appropriate access to health services in a timely fashion, particularly access to emergency departments (EDs).5,6 This awareness and concern have led to new ED protocols in the province of Alberta, 6 yet recent reports suggest these new ED-based protocols are still inadequate. 7
The utilization of EDs for nonurgent medical conditions contributes to excessive burden on hospitals and can result in longer wait times for medical intervention, regardless of severity.8-10 Patients seeking care for nonacute conditions have been confirmed as an important determinant of ED overcrowding. Almost one quarter of EDs report a large volume of nonacute patients as a “major or severe” cause of ED overcrowding. 10 Additionally, the treatment of minor medical conditions in an ED setting is associated with higher costs per treatment, increased reutilization of health services, and a decrease in the continuity of care delivered.3,4,9,11 Limited access to outpatient physician services leads many individuals with nonurgent medical conditions to seek care in local EDs.8-10
There is a need for more studies focusing on interventions to reduce ED overcrowding. 12 Previous research has focused on ED-specific interventions, while little attention has been paid to the influence of services delivered outside the ED setting.12-14 However, it has been estimated that 25% to 55% of acute care provided in an ED could be provided in an outpatient, physician office–type setting.3,13 The purpose of this study was to compare the number of low-severity patients accessing a hospital ED before and after implementation of a local after-hours clinic (AHC). We hypothesized that AHC operation would be associated with a significant decrease in the number of nonurgent and semiurgent patient visits to the local ED.
Methods
Study Design and Setting
The study design was observational in nature: a natural experiment. Prior to the Leduc AHC, primary care physician services in the Leduc area (Leduc, Alberta, Canada; population ~ 20 000) were generally limited to the local hospital ED and family physician offices during their hours of operation. The AHC operated from 6
Data Collection
We obtained daily patient visits to the local hospital ED from January 2005 to February 2008. Patient ED visits were organized according to the Canadian Triage and Acuity Scale. 15 Additionally, we collected the number of patient visits to the AHC from its implementation in August 2006 until February 2008. We focused our analysis on triage level 3, 4, and 5 patient visits or urgent, semiurgent, and nonurgent visits, respectively.
Outcome
The main outcome of interest was the number of nonurgent (triage 5) and semiurgent (triage 4) patient visits to the ED during the hours of AHC operation, before and after implementation of the AHC. Examples of semiurgent patients include those with minor trauma, pain ranging from 4 to 7 on an 11-point (0-10) numerical pain rating scale (NPRS), abdominal pain with or without diarrhea and vomiting and no signs of dehydration; those with acute joint swelling, and other similarly severe health concerns. Nonurgent patients include those with nasal congestion, chronic low back pain, and those with other mild symptoms or pain <4 on a NPRS. 15 It was the intent of the AHC to target these patient groups.
Analysis
The pre-AHC data included in our primary analysis consisted of January 2005 through February 2006. Post-AHC data consisted of January 2007 through February 2008. After matching by month, the mean difference in patient visits was calculated. We used Wilcoxon signed-rank tests (a nonparametric procedure) to assess for statistical significance between patient visits to the hospital ED before and after the AHC became operational. STATA SE 9.2 (StataCorp, College Station, Texas) was used for our data analyses. 16
Permission to use these records was given by the Leduc-Beaumont-Devon Primary Care Network, the Leduc Community Hospital Emergency Department, and the Capital Health Region. Data were provided to the researchers in an aggregate fashion. We did not have access to personal, identifying information. The University of Alberta Health Research Ethics Board reviewed the study protocol.
Results
Since implementation in August 2006, there has been an average of 262 patient visits per month to the AHC. Operation of the AHC was associated with significantly fewer semiurgent patient visits and fewer ED visits overall (P < .01). There was no significant difference in the number of urgent or nonurgent patient visits to the ED before and after AHC operation. These results are summarized in Table 1.
Emergency Department (ED) Visits per Month During After-Hours Clinic (AHC) Hours of Operation (6 PM-10
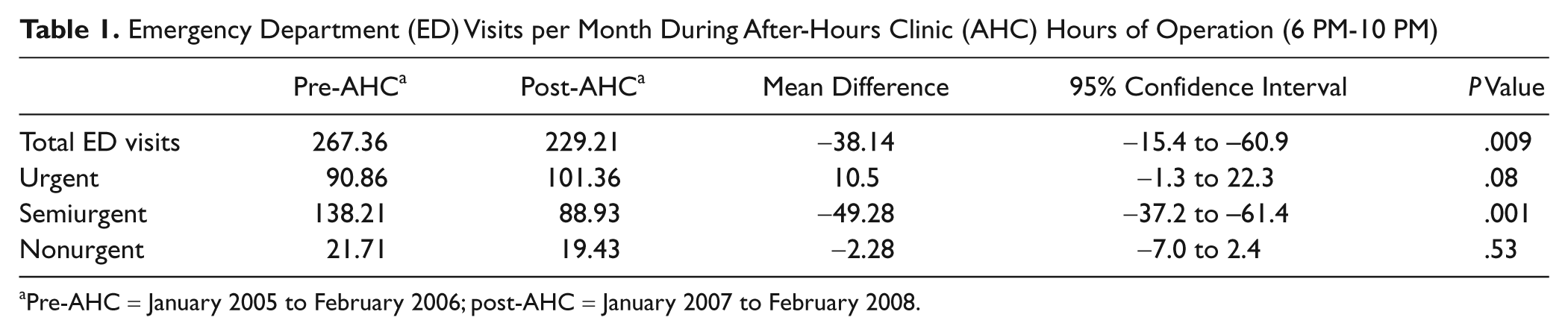
Pre-AHC = January 2005 to February 2006; post-AHC = January 2007 to February 2008.
The significant decrease in semiurgent (triage 4) patient visits per month to the ED, during AHC operating hours, was consistent throughout the follow-up period (Figure 1). Using the Leduc area annual populations, we calculated semiurgent patient visits to the ED during AHC operating hours per 1000 people, before and after implementation of the AHC. Prior to AHC operation, there was an average of 7.9 semiurgent patient visits per month per 1000 people to the ED from 6

Emergency department (ED) semiurgent patient visits by month: pre– and post–after-hours clinic (AHC) operation.
In addition to the reduction in semiurgent patient visits during AHC operating hours, the ED also saw a significant reduction in semiurgent patient visits during the day (Table 2). Again, there was not a significant change in the number of urgent or nonurgent patient visits to the ED subsequent to AHC operation.
Emergency Department (ED) Visits per Month During Daytime Hours (6

Pre–after-hours clinic (AHC) = January 2005 to February 2006; post-AHC = January 2007 to February 2008.
Data for the months of March 2006 to December 2006 were not included in our primary analysis. The exclusion of these months was to permit matching by calendar month pre- and post-AHC operation. It should, however, be noted that inclusion of these months in a secondary analysis yielded almost identical results.
Discussion
This study demonstrated that the addition of after-hours care significantly decreased the number of semiurgent (triage 4) patient visits to the ED in a small Canadian city of approximately 20 000 people. Not only was the crude number of patient visits in this group reduced, but the addition of after-hours physician care services was also associated with a 40% reduction in patient visits per 1000 people in the Leduc area. These findings are consistent with prior research in non-Canadian settings17,18; however, from our review, this appears to be the first study to evaluate the quantitative impact of community physician, primary care interventions aimed at reducing ED access by care seekers in the Canadian context.
In a systematic review of interventions to reduce attendances and waits in EDs, Cooke et al identified poor access to primary care as a major reason patients choose to seek care in an ED. 13 Other recent North American studies confirm no after-hours care, limited availability of walk-in clinics, and limited physician schedules as major drivers for ED care sought by individuals with low-severity conditions.4,10,19 In a qualitative study by DeSalvo et al, 8 almost 40% of individuals surveyed indicated that the lack of clinic services on evenings and weekends was their reason for seeking care in an ED. In line with these findings, an internal audit of patients attending the Leduc AHC found that 84% of respondents reported poor access to primary care services as a major reason for using the AHC. Additionally, over 40% of individuals at the AHC reported that they would have accessed the local ED had the option of attending the AHC not been available. 20
The present study demonstrates that after-hours physician services, outside the ED setting, are highly demanded and likely undersupplied. By providing after-hours care, the Leduc Primary Care Network has provided additional primary care services outside of traditional physician clinic hours and thus addressed many of the primary care access barriers that have been identified in the literature.
This study also provides important information regarding the size of intervention that may be needed per capita in order to have a meaningful influence on ED use. For example, the AHC in our study consisted of one family physician and one medical office assistant providing services to a population of approximately 20 000 people. This type of intervention was associated with a 40% reduction in semiurgent patient visits to the ED. This same intervention in a population of 100 000 people may not be adequate; thus, additional primary care services would be seen as insufficient or would not be considered for reducing ED use. A small intervention within a large population may account for the lack of effect of AHC care on ED use reported by others.21,22
Overcrowding of the ED is a significant concern in Canadian EDs, and the majority of interventions have been applied in the ED setting.10,12 Our study addresses this gap in the literature by providing information on the impact of an AHC, an intervention external to the ED and in the Canadian context. Considering the provincial delivery and design of health care services in Canada, we believe these results may be generalized to other Albertan cities of similar size and, to some extent, to similar cities across Canada.
Strengths and Limitations
For this investigation, we were unable to include the frequency of patient visits to other physician offices in the Leduc area. For this reason, it is difficult to attribute the changes in ED use solely to the provision of after-hours care. However, there was a significant decrease in semiurgent patient visits to the ED, while urgent patient visits tended to increase slightly (although not statistically significant). The decrease in semiurgent patient visits to the ED occurred in the face of significant population growth, and our analysis controlled for time of day, time of year, and day of the week.
Secondly, the Leduc ED was newly renovated in 2006. 23 The specific impact of this on primary care utilization may be unclear. However, as the ED increased its capacity with its renovations, 23 one would expect patient visits to increase as a result. Conversely, we clearly demonstrated that ED visits for the largest population of patients, semiurgent patients, significantly decreased in the presence of the AHC.
Other limitations include variables for which it would be very difficult to control. For example, Leduc, a city of 20 000 people, is approximately 30 minutes from Edmonton, Alberta, a city of almost 1 million people. The extent to which individuals in Leduc utilize services in Edmonton, or vice versa, is not specifically known. The actual impact of the AHC may be overestimated or underestimated depending on geographical patient-service utilization patterns. Also, the true impact of the AHC may depend on individual patient characteristics. Those who are frequent users of the health care system may use the ED and subsequently seek care at the AHC. Still, our findings suggest that regardless of patient usage patterns, the addition of a family physician AHC significantly reduces ED use for low-severity conditions. The reduction in ED use for this population is consistent and observationally (Figure 1) and statistically significant (P < .01).
Conclusions
When viewed in the context of prior Canadian research,9-12 our findings suggest that the provision of after-hours care in a physician office setting provides additional primary care services in an appropriate and cost-effective manner. In fact, AHC care may reduce inappropriate ED use, decrease reutilization rates, and ultimately promote greater satisfaction with care for care seekers. Physician office wait times have consistently been identified as a barrier to primary care access and may drive individuals to seek care in an ED setting. Future research should aim to identify and describe the individuals who utilize after-hours care services as well as evaluate potential barriers to utilization of after-hours care (such as wait times to see a physician).
Health care sustainability is a frequent topic of discussion and a necessary consideration. Future studies should continue to re-evaluate the cost-benefit of providing AHC care. Attempts should be made to evaluate the impact on overall population health when these initiatives (ie, AHC care) are put in place. Finally, further studies may want to focus on larger urban settings, as these are the areas most likely to suffer ED overcrowding and possibly inappropriate ED use.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
David Jones’s participation was made possible by scholarship from the Western Regional Training Centre for Health Services Research (WRTC) and Linda Carroll’s participation was made possible by a salary award from the Alberta Heritage Foundation for Medical Research. Partial financial support for the study came from the Leduc Beaumont Devon Primary Care Network.