
Abstract
Many veterans who receive primary care from the Veterans Administration (VA) also use private sector primary care. Previous studies using administrative files estimate 10% to 54% of elderly veterans eligible for both VA and Medicare choose to do so.1-5 In a patient-level survey from the Minneapolis VA, Borowsky et al reported 28% of veterans reported non-VA primary care visits. 1 This “dual use” for primary care, also known as “dual-management,” may have positive or negative consequences. Prior work suggests that dual-management may offer better access, convenience, and flexibility to primary care.1,3,6-7 However, when veterans, likely older with multiple chronic health conditions, receive primary care from multiple providers, there is risk for poor communication, discontinuity, and duplication of services, which may be harmful or at least wasteful of resources.5,8
Several studies have examined factors associated with dual use. Studies of dual VA-Medicare eligible veterans have found that veterans who were Caucasian, older, married, college graduates, have higher incomes, lower VA priority level, live relatively far from VA hospitals or in urban areas with more health care resources, and have higher levels of illness burdens are more likely to be dual users.2-3,9-12 Studies including veterans less than 65 years have found similar associations, along with having private insurance.8,13
Other studies have evaluated adverse outcomes among dual-users in the inpatient setting.2,5-6 Wolinsky reported that dual users had a 56% greater relative risk of mortality than comparable nonveterans, suggesting that dual use was likely to increase the risk of uncoordinated care, which could lead to increased hospitalizations and other adverse outcomes. 2 Few studies have examined primary care dual-management, and to our knowledge, no studies have examined the impact of primary care dual-management on quality.
Our study objective was to determine the extent of dual-management and evaluate the association between primary care dual-management and measures of quality among veterans with a common chronic condition (hypertension) and other common comorbid conditions (diabetes, hyperlipidemia, and obesity).
Methods
Subjects
Primary care patients were recruited from the Iowa City and Minneapolis VA Healthcare Systems and four affiliated community-based outpatient clinics (CBOCs) from September to November 2004. Eligible patients included a convenience sample of 191 primary care patients with hypertension confirmed by chart review. Patients were recruited while waiting to see their primary care provider and asked if they would participate in a 15-minute survey on blood pressure treatment. Of 191 patients approached to participate, 189 agreed (99%).
Survey
Because identification of non-VA providers was not in the medical record, dual-management was determined by the question: “Outside the VA, do you have a primary care provider such as an internist or family doctor that you see on a regular basis?” For subjects who answered affirmative, two follow-up questions were asked: (1) type of non-VA provider (ie, internist, family practitioner, nurse practitioner, physician’s assistant, or other), and (2) which provider (ie, VA primary care provider, non-VA primary care provider, VA specialist, or non-VA specialist) manages blood pressure.
Additional information was collected through review of the VA medical record including demographics, hypertension medications and intolerances, blood pressures (BP) for the past 12 months, comorbid illnesses, whether the patient was at their BP goal, and if they were on the Joint National Committee on the Detection and Prevention of Hypertension (JNC-7) guideline concordant therapy. BP goal was defined as <140/90, or <130/80 for patients with diabetes or renal insufficiency. Two physician-investigators (PJK, AI) reviewed patient VA medical records to determine appropriate goal BP and guideline concordant therapy. They reviewed JNC-7 guidelines, performed implicit chart review, and discussed cases; formal interrater reliability wasn’t performed. Guideline concordance was defined by being on a thiazide diuretic, either alone or combined with drugs of other classes, or having certain high-risk conditions with compelling indications for the initial use of other antihypertensive drug classes (eg, beta blockers, angiotensin converting enzyme inhibitors). Medication lists were reviewed with the patient to ensure accuracy. Low density lipoprotein (LDL) cholesterol and hemoglobin A1C values were abstracted from the chart from the prior 12 months. The Institutional Review Boards (IRB) of the Iowa City and Minneapolis VA Healthcare Systems approved this study and all patients signed informed consents.
Data Analysis
Descriptive statistics were generated for both samples. Differences between groups were analyzed using Student’s t tests and analyses of variance for continuous variables and chi-square tests for categorical variables. P values < .05 were considered significant. All analyses were performed using SAS version 8.0 (Cary, NC).
Results
Mean age of subjects was 65.8 years, 97% were male, and 92% were white with no significant differences between dual-managed and VA-only managed subjects by gender, race, education, mean blood pressure, or comorbid illnesses. However, dual-managed subjects were older (69.1 vs 64.0 years; P < .01) and more likely to have a medication copayment (70% vs 48%; P < .01) (see Table 1).
Characteristics of All Subjects (N = 198), Stratified by Dual-Managed (N = 67), and VA-Only Care (N = 122)
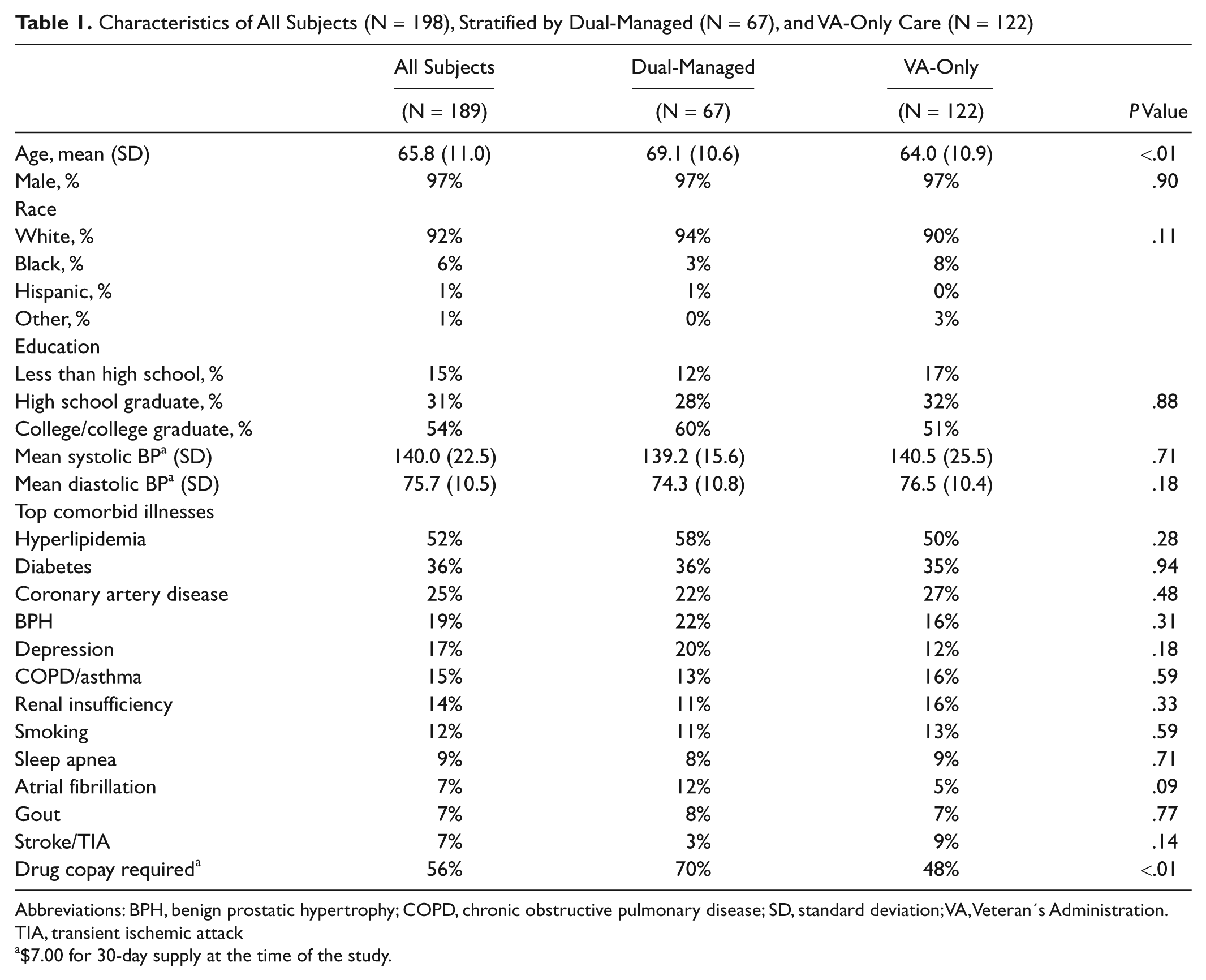
Abbreviations: BPH, benign prostatic hypertrophy; COPD, chronic obstructive pulmonary disease; SD, standard deviation; VA, Veteran’s Administration. TIA, transient ischemic attack
$7.00 for 30-day supply at the time of the study.
Patient Survey Results
When asked, “Outside VA, do you have a primary care provider such as an internist or family doctor that you see on a regular basis?” 36% responded “yes” (N = 67), indicating dual-management. Analyzed by site, 42% of Iowa subjects were dual-managed compared to 28% in Minneapolis (P = .04); no other site differences were noted. When queried about who manages their hypertension, 88% indicated a VA provider, 16% a non-VA provider, and 4% both. Among the subset of the 67 dual-managed subjects, the non-VA providers were family physicians (73%), internists (6%), nurse practitioners/physician’s assistants (6%), and others (9%). Of these dual-managed subjects, 67% said their blood pressure was managed by a VA primary care provider, 3% a VA specialist, 46% a non-VA primary care provider, and 8% a non-VA specialist (sum greater than 100% due to multiple responses).
Quality of Care
Quality of care process measures and intermediate outcomes are reported in Table 2. With regard to hypertension measures, 51% of the subjects were at goal blood pressure, 58% were on JNC-7 guideline concordant therapy, and 32% were both at goal and on guideline concordant therapy. In addition, 31% reported knowledge of their BP goal. There were no significant differences between dual-managed and VA-only managed subjects in any of these measures.
Quality of Care Measures for Hypertension, Obesity, Hyperlipidemia, and Diabetes Mellitus, Stratified by Dual-Managed and VA-Only Care a
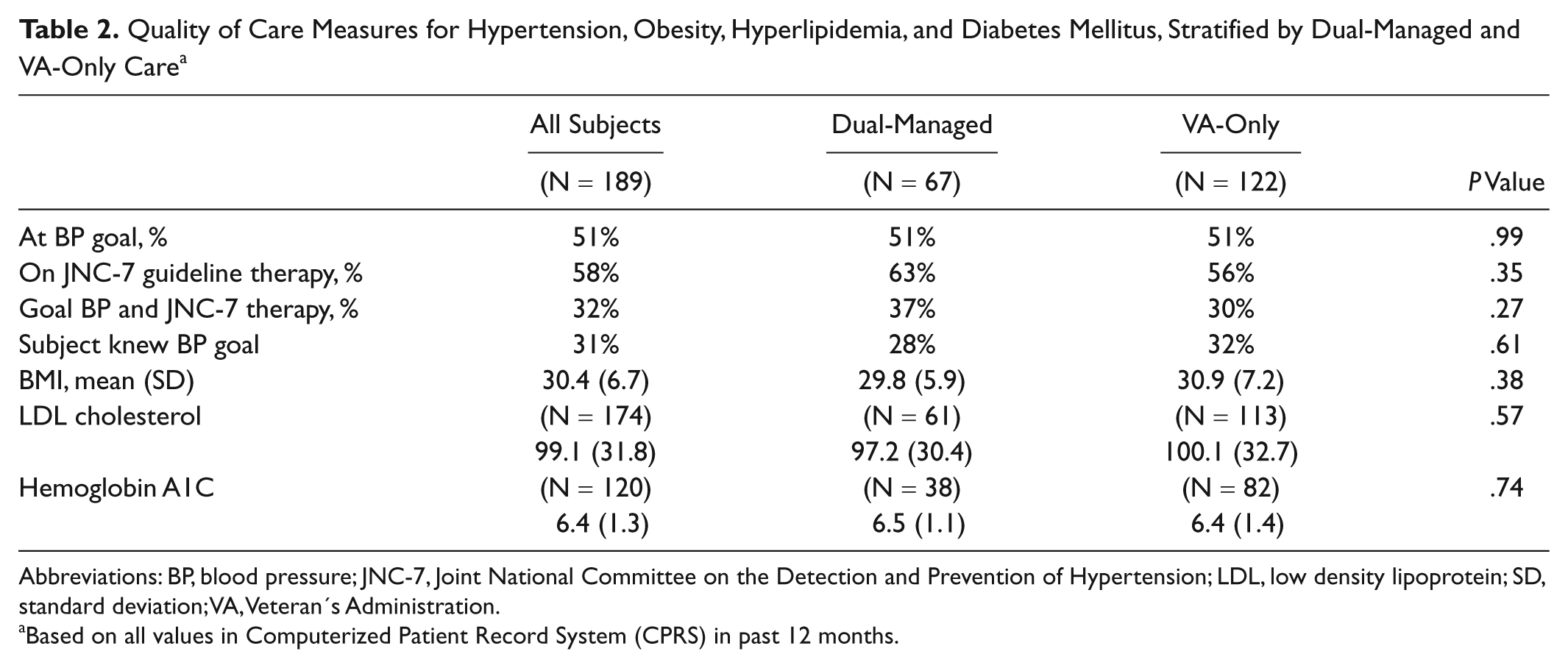
Abbreviations: BP, blood pressure; JNC-7, Joint National Committee on the Detection and Prevention of Hypertension; LDL, low density lipoprotein; SD, standard deviation; VA, Veteran’s Administration.
Based on all values in Computerized Patient Record System (CPRS) in past 12 months.
In relation to obesity, mean body mass index (BMI) was 30.4, with no significant difference between groups. Among the 174 subjects with LDL cholesterol values in the prior 12 months, mean LDL was 99.1 mg/dl with no difference between dual-managed and VA-only managed. Mean hemoglobin A1C values, available for 120 subjects, were 6% with no difference between groups.
BP Medication Use
Subjects used a mean of 2.4 BP medications with no different between groups (see Table 3). Due to VA formulary limitations, specific BP medication classes are described in detail with notable differences. VA-only patients were more likely to be on ACE-inhibitors (62% vs 43%; P = .02) or a medication designated “other category,” such as hydralazine or clonidine (11% vs 2%; P = .02). Dual-managed patients were more likely to be on a thiazide (43% vs 28%; P = .03) or an angiotensin-receptor blocker (ARB) (13% vs 3%; P < .01). For patients using only one BP medication (ie, monotherapy), there were no significant differences between groups (results not shown).
Blood Pressure Medication Use for All Subjects, Stratified by Dual-Managed and VA-Only Care
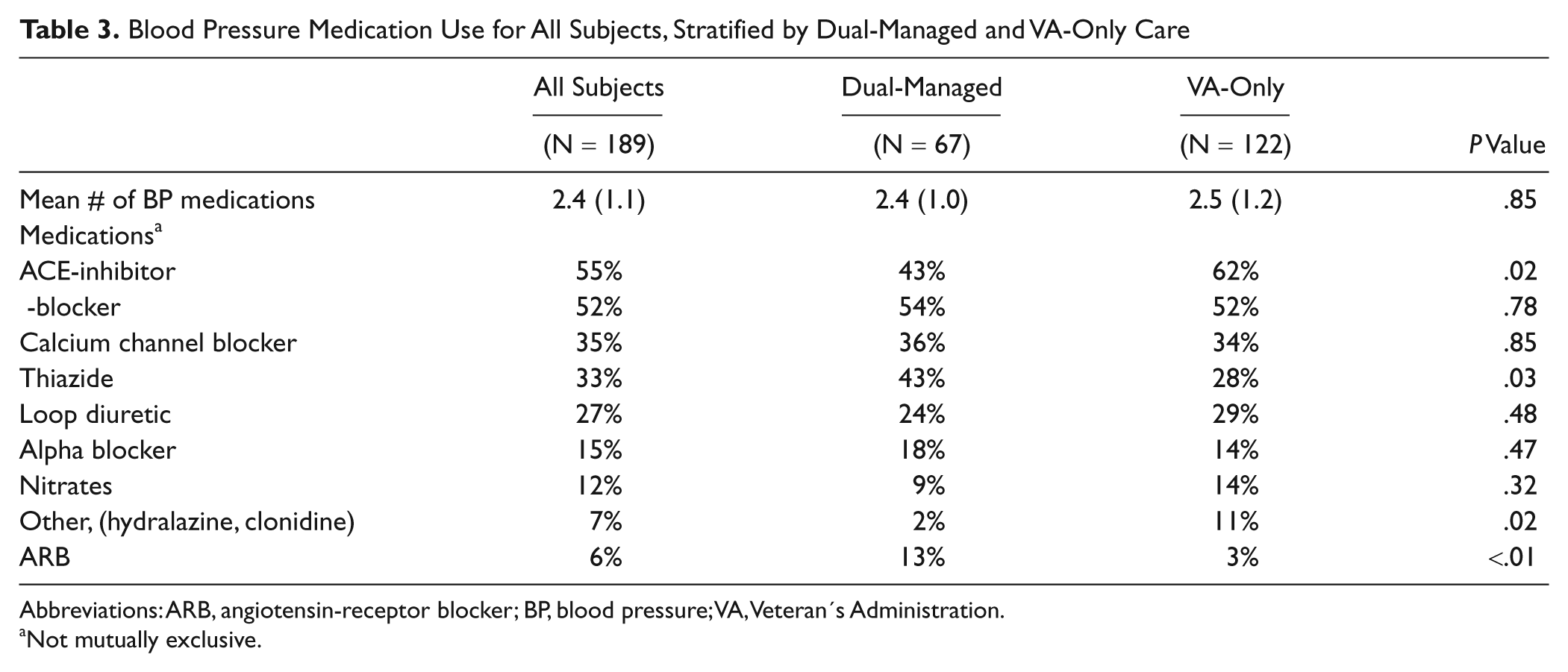
Abbreviations: ARB, angiotensin-receptor blocker; BP, blood pressure; VA, Veteran’s Administration.
Not mutually exclusive.
Discussion
The objective of our study was to determine the extent of primary care dual-management and better understand the potential impact on quality of care for veterans with hypertension. We found that 36% of participating veterans reported dual use, which is in the middle of the 10% to 54% range previously reported.1-4 Interestingly, the vast majority reported their VA provider managed their hypertension. Although this may represent social desirability as questions were asked in a VA clinic, it highlights the complex nature of identifying dual-management as patients may receive medical services from different sources, but may limit who provides certain aspects of their care. We also found a difference in dual-management by location, with higher rates of dual-management in Iowa (42%) compared to Minneapolis (28%), the same rate reported by Borowsky in Minneapolis in 1999. 1 Prior studies have shown higher rates of dual-management in both urban and rural3,7 VA patients, so this difference is not clearly explainable. While there were no significant differences in patient demographics in the two sites, it’s possible this difference is a function of travel time to primary care clinics or related to differences in private insurance status. Travel times and non-VA health insurance status were not available.
We found almost no differences in intermediate outcomes or process measures of care evident from the VA medical record, suggesting neither benefit nor harm from dual-management. The few differences detected were mainly related to medication use. Dual-managed patients were more likely to receive a thiazide than VA-only patients. This was unexpected given VA efforts to promote guidelines that thiazide diuretics are first-line treatment. Higher rates of ACE-inhibitor use in VA-only managed patients can be explained by higher use of ARBs in dual-managed patients. At the time, ARBs were restricted by the VA formulary to patients who had failed an ACE-inhibitor. Because of this restriction, and possibly because of private sector use of ARB samples, more ARBs and less ACE-inhibitors were prescribed in dual-managed patients. Medication class prescribing rates were not explained by the presence of comorbid conditions.
The majority of previous studies have focused on quantifying dual use and identifying associated veteran characteristics as opposed to evaluating implications of dual use on quality of care.3,6-7,9-11,13 Similar to these studies, we found older age was associated with increased dual use. One explanation is that older patients are more likely to be dual-eligible for Medicare and VA services and may substitute non-VA care for VA care, as suggested by Weeks. 7 We also found that VA-only managed patients were less likely to have a medication copayment, suggesting either a higher level of VA benefit because of indigent status or service-connected disability, similar to findings of previous studies.3,9,11
Among studies that have assessed quality, Wolinsky et al concluded that dual use was associated with increased risk of mortality. However, these analyses were based on an indirect measure of dual use (no VA data was used nor were subjects asked about dual use). Furthermore, the main findings of these studies were driven by dual users of inpatient services who may be different from those being dual-managed by primary care providers in outpatient settings.2,5 Jia found that dual users were significantly more likely to be rehospitalized for any cause and for recurrent stroke 12 months after the index hospitalization, but it is unclear from the findings whether greater utilization in the form of hospitalizations represents poor quality care or appropriate care facilitated by greater access and/or needed by more severely ill patients. 12 Fischer et al found that dual users were actually more likely to receive predialysis nephrology care than VA only users. 14 Other studies addressing quality focused on the use of preventive services and found no difference between dual users and VA-only users. 15
Limitations
Our findings have several important limitations. First, precise definitions of dual-management or dual-use are not established. However, by asking the patient how they receive care, we were able to establish whether they received care from a non-VA provider. We did not have non-VA medical records to validate answers. Second, we used a convenience sample that could introduce bias, especially when asking patients who manages their hypertension. Of note, 99% of patients approached agreed to participate. Third, only VA medical records were available, so we lacked detailed information on non-VA care. However, VA and non-VA antihypertensive medications were reconciled during the interview to account for the absence of non-VA medications on the VA computerized medical record.8,16 Fourth, generalizability beyond a mostly white, male, Midwest, VA patient population may be limited. Fifth, due to the complexity associated with determining JNC-7 guideline-concordant therapy and lack of formal interrater reliability testing, there was some potential for misclassification. Finally, our sample size was small. However, given that almost all of our findings in Table 2 either favor the dual-management group or are nearly identical between the two groups, the only remaining measure that we could have failed to detect a significant difference in favor of VA-only was that the “subject knew BP goal,” for which only four percentage points separated the two groups.
Conclusions
This is the first study to evaluate the impact of dual-managed primary care on measures of quality and we found almost no differences between the VA-only and dual-managed groups. With the large numbers of returning veterans from current conflicts, most of whom will have non-VA health insurance yet are all eligible for VA services for a minimum of five years, the issue of dual-management will increase. Future studies should examine the impact of dual-management on other common conditions, examine other quality measures, explore cost-implications, and diagnostic testing redundancy.
Footnotes
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Dr Kaboli was supported by a Research Career Development Award (RCD 03–033–1) and a Investigator Initiated Research grant (IMV 04-066-1) both from the Health Services Research and Development Service, Department of Veterans Affairs. He was also supported by the Center for Research in the Implementation of Innovative Strategies in Practice (CRIISP) at the Iowa City VA Healthcare System, Iowa City, IA.