
Abstract
Introduction
Gestational diabetes mellitus (GDM), defined as any degree of glucose intolerance first discovered during pregnancy, 1 is estimated to complicate 5%-7% of all pregnancies annually. Infants born to mothers with GDM have an increased risk of developing a range of adverse birth outcomes; however, excessive fetal growth is the most common morbidity.2,3 Documented outcomes associated with excessive fetal growth include shoulder dystocia, brachial plexus injuries, clavicle fractures, meconium aspiration, perinatal asphyxia, hypoglycemia, and fetal death.4-6 Excessive fetal growth also increases the risk of maternal complications,4,5 and it may be associated with longer-term outcomes such as type 2 diabetes and metabolic syndrome among offspring. 7
Evidence suggests that proper disease management can lead to improved perinatal outcomes.2,8-11 The potential for excessive fetal growth outcomes coupled with the complexity of medical management among women with GDM suggests that prenatal care may be associated with improved outcomes. The research reported here examines the degree to which excessive fetal growth outcomes vary across levels of prenatal care among women with GDM.
Methods
Study Population
We constructed a retrospective cohort of all women with a singleton live birth in South Carolina from 2004-2007 for whom both birth certificate and maternal hospital discharge claims were available. To avoid bias associated with multiple pregnancies by the same individual, analysis was restricted to singleton live births from the first pregnancy during the period. Analysis was further restricted to women with births > 28 weeks gestation, since prenatal screening for gestational diabetes typically occurs between 24-26 weeks. 1 Women with missing values for large for gestational age (LGA) or prenatal care data were also removed from analysis, leaving a total of 179 957 women in the study population.
Data were obtained from the Office of Research and Statistics of the South Carolina Budget and Control Board. The Office of Research and Statistics serves as a repository for all health information in the state of South Carolina, including mandatory reporting for all hospital discharges. The study was approved by the University of South Carolina Institutional Review Board.
Dependent Variable: Excessive Fetal Growth
Excessive fetal growth served as the primary outcome variable; we used 3 measures. Our first measure, infants born in the 90th and 95th percentiles for weight, was defined using sex-specific birth weight percentiles for gestational age from Oken et al. 12 These items were taken from the birth certificate and gestational age was determined using the clinical estimate. Third, we used a standard variable for macrosomia, defined as infants with birth weights ≥ 4500 g, regardless of gestational age.
Independent Variables of Interest Prenatal Care
Adequacy of prenatal care was measured using the Adequacy of Prenatal Care Utilization index. 13 This index characterizes prenatal care use according to the timing of initiation and adequacy of visits received. These 2 variables can be combined to create a single 4-level prenatal care use index: Inadequate, Intermediate, Adequate, and Adequate Plus. For the purposes of this study, we combined Intermediate and Adequate prenatal care use into 1 category. Care is defined as “Inadequate” for women initiating prenatal care after the fourth month of pregnancy or women receiving < 50% of recommended visits. “Intermediate/Adequate” prenatal care includes women entering prenatal care in months 1-4 who received 50%-109% of the recommended visits. Finally, “Adequate Plus” care includes women entering prenatal care in months 1-4 who received > 110% of the recommended visits. Receipt of Adequate Plus care can reflect underlying health conditions warranting intensive use. 14 Data for this variable were obtained from birth certificate records.
Previous studies have noted the limitations of relying on birth certificate data alone for the identification of maternal complications associated with pregnancy, including GDM.15-17 The use of hospital discharge claims in conjunction with birth certificate records can greatly improve the ascertainment of medical conditions that have an impact on pregnancy. 18 For the present research, women in the cohort with GDM indicated on the birth certificate or with an ICD-9 code of 648.8 (GDM) in the hospital discharge claim were considered to have GDM. Approximately 8910 women were identified as having GDM on the birth certificate. Linking birth certificate records with hospital discharge claims identified an additional 3705 women with an ICD-9 code of 648.8 not indicated in birth certificate records.
Covariates
Anderson’s Behavioral Model for Health Services Use served as the conceptual framework for selecting appropriate covariates. 19 Predisposing characteristics were derived from the birth certificate and include race/ethnicity, maternal characteristics, education, and parity. Enabling characteristics were also derived from the birth certificate and include marital status and insurance status. Measures of individual need held constant in the analysis include maternal body mass index, excessive gestational weight gain, gestational hypertension, and smoking status. Environmental characteristics include rural residence based on Rural-Urban Commuting Areas. 20
Analysis
Bivariate analysis comparing outcomes among categorical variables used chi-square tests for independence. In addition, unadjusted odds ratios were obtained for levels of prenatal care and selected measures of excessive fetal growth outcomes by GDM status. Multivariable logistic regression was performed with each of the outcomes (LGA 90th percentile, LGA 95th percentile, and macrosomia, > 4500 g) serving the dependent variable. Interaction terms for adequacy of prenatal care and GDM status were included in each model and found to be significant. Therefore, we used a composite variable created from adequacy of prenatal care and GDM status in the models. For this variable, the reference group was set as women with GDM and Intermediate/Adequate prenatal care. Comparison groups were women with GDM and Inadequate prenatal care, women with GDM and Adequate Plus prenatal care, women with no GDM and Inadequate prenatal care, women with no GDM and Intermediate/Adequate prenatal care, and women with no GDM and Adequate Plus prenatal care. Other environmental, predisposing, and enabling items and measures of individual needs were included as covariates in each model.
Results
Characteristics of Population
Characteristics of women in the study population are shown in Table 1. Approximately 6.9% of women were identified as having GDM. Over half (54.9%) of women with GDM were non-Hispanic white, 38.9% non-Hispanic black, and 3.2% non-Hispanic other, and 9.0% were of Hispanic ethnicity. Characteristics of women with GDM differed from their counterparts in several notable areas. Women with GDM were more likely to be over the age of 35, married, obese; to have private insurance; and to have both prepregnancy and gestational hypertension.
Characteristics of South Carolina Cohort of Women with a Singleton Live Birth 2004-2007, by Gestational Diabetes Mellitus Status
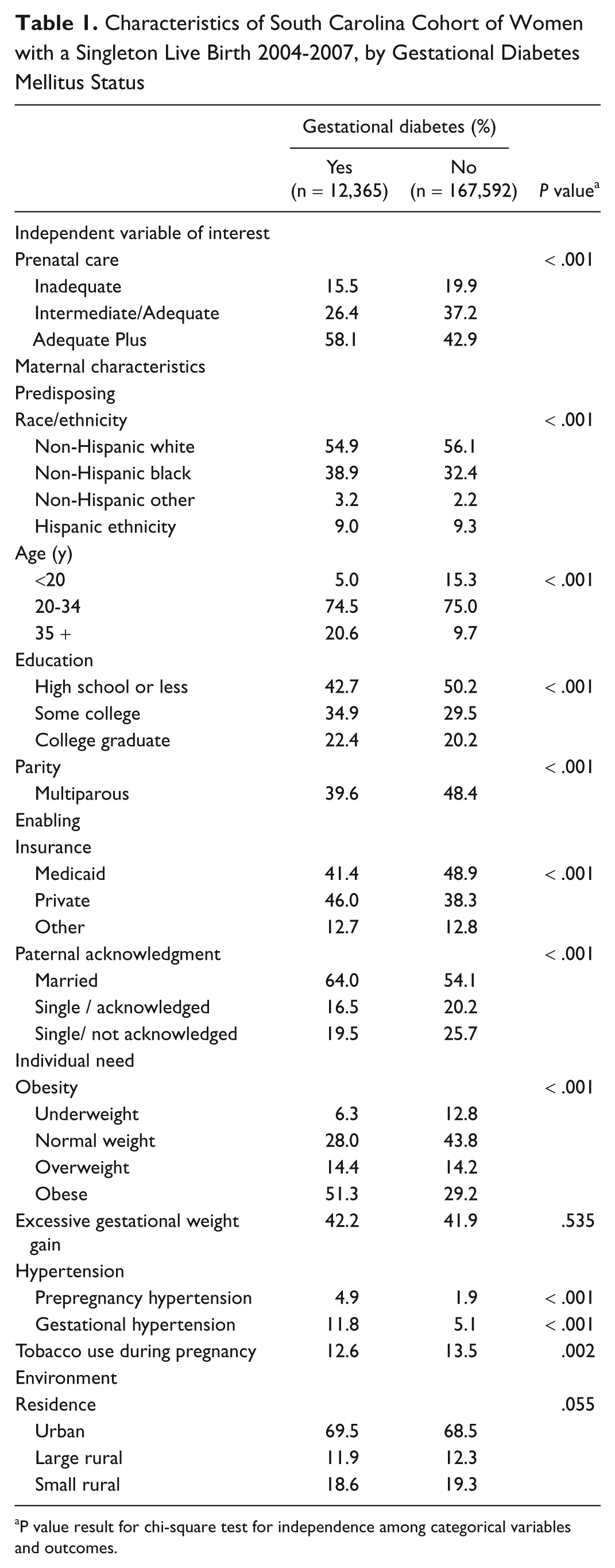
P value result for chi-square test for independence among categorical variables and outcomes.
Excessive Fetal Growth Outcomes by Level of Prenatal Care
The majority of women with GDM received Adequate Plus prenatal care (58.1%); however, 15.9% received Inadequate care (Table 1). As shown in Table 2, the proportion of excessive fetal growth outcomes was higher among women with GDM than among those without GDM, regardless of the level of prenatal care. There was a significant interaction effect between GDM status and level of prenatal care received. Among women with GDM, the proportion of births with any of the 3 excessive fetal growth outcomes was highest among women receiving Inadequate or Adequate Plus care, and lowest among those with Intermediate/Adequate care, whereas the opposite was true for women without GDM (Table 2). In the multivariable analyses that follow, an interacted variable that combines GDM and care status is used, with GDM and Intermediate/Adequate Prenatal Care as the referent level.
Proportion and Unadjusted Odds of Excessive Fetal Growth Outcomes by Adequacy of Prenatal Care and Gestational Diabetes Status, South Carolina 2004-2007

Abbreviations: CI, confidence interval; GDM, gestational diabetes mellitus; OR, odds ratio.
Significant differences (P < .05) in excessive fetal growth outcomes within levels of prenatal care based on GDM status.
Adjusted Analysis of Excessive Fetal Growth Outcomes
As shown in Table 3, after adjusting for additional covariates, women with GDM and Inadequate prenatal care were markedly more likely to experience excessive fetal growth outcomes than women also with GDM receiving Intermediate/Adequate prenatal care (odds ratio [OR] = 1.38, confidence interval [CI] = 1.15-1.66). Additionally, women with GDM receiving Adequate Plus prenatal care also had increased odds of large infant outcomes (OR = 1.19, CI = 1.04-1.36). Similar patterns were noted using more stringent definitions of LGA (95th) and macrosomia (total birth weight > 4500 g). When compared to women with GDM and Intermediate/Adequate prenatal care, the likelihood of large infant outcomes was highest among women with GDM and Inadequate prenatal care and to lesser degree women with Adequate Plus prenatal care.
Odds of Excessive Fetal Growth Outcomes, South Carolina 2004-2007

Abbreviations: GDM, gestational diabetes mellitus; HTN, hypertension; OR, odds ratio.
Several additional factors were associated with experiencing excessive fetal growth outcomes. Women with a previous birth, those 35 years of age and older, and those who were obese or had gained weight in excess of Institute of Medicine recommendations were much more likely to experience excessive fetal growth outcomes.
Discussion
The relationship between GDM and excessive fetal growth outcomes is well established in the literature.2,3,6,10,21 What is less clear is the extent to which prenatal care could be associated with excessive fetal growth outcomes among women with GDM. The present study focused on identifying variation in the likelihood of excessive fetal growth outcomes across levels of prenatal care. We found observed associations between prenatal care use and excessive fetal growth outcomes among women with GDM follow a U-shaped curve.
The likelihood of large infant outcomes was highest among women with GDM and Inadequate prenatal care, and to a lesser degree, among women with GDM and Adequate Plus care when compared to women with GDM and Intermediate/Adequate care. Findings related to the Adequate Plus category are not surprising, given that this use category is intended to identify women with intensive usage likely stemming from complicated pregnancies. However, data on the severity of GDM and pregnancy complications were not available for this study, which limits the conclusions that can be drawn from observed associations. Consistent with previous literature, this study also found obesity, GDM, and excessive weight gain to be associated with excessive fetal growth outcomes.7,22-26
Although a single cross-sectional study is not sufficient to establish that good prenatal care can improve infant outcomes among women with GDM, it does suggest directions for future research. Examining the impact of factors beyond the scope of a prenatal care use index should be a focal point for future research. More specifically, how might outcomes differ with receipt of supportive health services, such as self-management education and nutritional counseling? What role does maternal behavioral change during pregnancy have on observed outcomes? How might different GDM screening and diagnostic criteria influence observed outcomes? What is the comparative effectiveness of alternate GDM therapies in reducing excessive fetal growth? The ability to answer these important research questions is beyond the scope of the data available for this study.
The present study is limited in several ways. First, the study is observational and should not be taken to imply causality. Characteristics of women initiating prenatal care early and adhering to the scheduled number of visits could be systematically different from women with lower adherence. We attempted to control for this potential bias by including only the first pregnancy for women in the cohort and adjusting for covariates that could capture some of these factors that might be associated with late initiation of prenatal care. Second, the information used was obtained retrospectively from secondary sources, and variable accuracy could not be independently verified through chart review. Finally, the study is not able to account for variation in the quality of prenatal care provided and can only classify women by prenatal care use.
The study has several strengths. Although limited to a single state, the study draws from a large, diverse sample of women and includes a significant number of women with GDM. Second, linking birth certificate to hospital discharge data increased the level of ascertainment for GDM. Combining multiple data sources to more accurately identify women with GDM improved data quality and helped to minimize potential misclassification bias.
Gestational diabetes mellitus is an important pregnancy-related morbidity that can have a significant effect on maternal and infant outcomes. The occurrence of GDM is predicted to increase corresponding to increases in the prevalence of obesity and type 2 diabetes. As more women experience diabetes-related complications during pregnancy, the need for quality prenatal care services will continue to increase. Although prenatal care may not be able to prevent all adverse outcomes from occurring, it may be influential in minimizing the potential impact such conditions have on infant and maternal outcomes. Although intensive screening, management, and treatment have made it possible for women with GDM to experience pregnancies similar to lower risk women, many women still do not receive these services.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.