
Abstract
Objective:
To review our 4-year experience (2008–2011) with delivery room triage of large for gestational age infants of diabetic mothers.
Design/Methods:
Retrospective cohort investigation of 311 large for gestational age infants of diabetic mothers (White’s Class A1 (77), A2 (87), B (77), and C-R (70)).
Results:
Of 311 women, 31% delivered at 34–36 weeks gestational age and 69% at term. While 70% were delivered by cesarean, 30% were vaginal deliveries. A total of 160 asymptomatic infants were triaged from the delivery room to the well baby nursery. Of these, 55 (34%) developed hypoglycemia. In 43 cases, the hypoglycemia was corrected by early feedings; in the remaining 12, intravenous dextrose treatment was required. A total of 151 infants were triaged from the delivery room to the neonatal intensive care unit. Admission diagnoses included respiratory distress (51%), prevention of hypoglycemia (27%), prematurity (21%), and asphyxia (1%). Hypoglycemia affected 66 (44%) of all neonatal intensive care unit infants.
Conclusion:
Safe triage of asymptomatic large for gestational age infants of diabetic mothers from the delivery room to well baby nursery can be accomplished in the majority of cases. Those infants in need of specialized care can be accurately identified and effectively treated in the neonatal intensive care unit setting.
Background
Large for gestational age (LGA) infants of diabetic mothers (IDM) are at high risk of significant neonatal morbidities, including prematurity, birth trauma, respiratory distress, and hypoglycemia that often require admission to the neonatal intensive care unit (NICU).1–4 Although beneficial, admission to the NICU may prolong hospitalization, disrupt maternal–infant interaction,5–8 and affect breast-feeding (BF) initiation.9–11 The ideal management of the LGA IDM should maximize maternal–infant contact, which is best accomplished in the well baby nursery (WBN), without compromising those infants in need of NICU care. Recent publications support admissions of IDM to transitional or intermediate care facilities to promote bonding, BF, and attachment.12,13 A decrease in the number of unnecessary NICU admissions and shorter NICU stays may have a dramatic financial impact and, more importantly, may improve today’s low BF initiation rates for this challenging obstetrical population. In our institution, late preterm (34–36 6/7 weeks GA) LGA IDM and term LGA IDM are triaged to either the WBN or the NICU.8–10 Successful delivery room (DR) triage for this unique group of infants depends on a clear definition of those deemed symptomatic, a strong postnatal screening and management approach for hypoglycemia, and a sound understanding of the clinical changes that may develop during their hospitalization.
Objective
To review our experience (2008–2011) with the DR triage of LGA infants born to women with gestational and pregestational diabetes mellitus.
Subject and methods
This retrospective cohort investigation was approved by the Institutional Review Board of Wexner Medical Center at The Ohio State University. Hard copies and electronic maternal and neonatal records were reviewed. Women diagnosed with gestational (Class A1–A2) and pregestational (Class B and C-R) diabetes mellitus according to clinical and laboratory criteria were grouped using the modified White’s classification. 14 Women with chronic hypertension and/or superimposed preeclampsia were included. Obesity was defined by a body mass index (BMI) of 29–34 kg/m2 and extreme obesity by a BMI ≥ 35 kg/m2. 15 The study population consisted of women with diabetes and their LGA (birth weight ≥ 90% for GA) or macrosomic (birth weight ≥ 4000 g) infants if delivered at ≥34 weeks, a point in gestation in which most infants are able to orally feed. 16 Pregnancies affected by major or fatal malformations were excluded. In cases of twin gestation, only the firstborn infant was reported. Upon arrival to labor and delivery, women’s feeding preference for their infants (BF or formula feeding) was ascertained.
Depending on the condition of the mother and her infant following delivery, maternal–infant interactions (holding, skin-to-skin contact, BF, and postpartum visitation) were encouraged. Our institutional guidelines for management of LGA IDM recommend that any symptomatic infant regardless of the mother’s class of diabetes be directly transferred to the NICU. Indications for NICU admission included respiratory distress (respiratory distress syndrome (RDS) and transient tachypnea of the newborn (TTNB)), prematurity (severe hypotonia and poor sucking behavior), perinatal asphyxia, and birth trauma. Our guidelines also recommend that asymptomatic LGA infants born to Class A1 and A2 mothers be transferred to the WBN for routine care, whereas those born to women with pregestational diabetes Class B and C-R be admitted to the NICU for prevention of hypoglycemia.
Screening for neonatal hypoglycemia (blood glucose < 40 mg/dL) was done via serial point of care testing (Accu-Chek®) starting by the first hour of life and prior to the first feeding. WBN infants with hypoglycemia were breast-fed or given formula feeding. Those with recurrent hypoglycemia were treated with intravenous (IV) dextrose (4-6 mg/kg/min). All infants admitted to the NICU were started on IV dextrose (60–80 mL/kg/day) on arrival.
Given that women who breast-feed only 1–2 times per day are likely to stop BF soon after delivery, 17 we defined BF as initiated if, at the time of discharge from the hospital, the infant was exclusively breast-fed or was receiving ≥50% of the feedings directly from the breast or by expressed breast milk. Due to the study design, no follow-up information was gathered on infant feeding practices beyond hospital discharge.
Statistical analysis
Comparisons between groups and subgroups of patients were made with Student’s t-test for continuous variables and chi-square or Fisher’s exact tests for categorical variables. Significance was established at a p value ≤0.05. Univariate logistic regression and multivariate logistic regression were used to ascertain the strength of association of maternal variables (diabetes class, primiparity, BMI, smoking, and mode of delivery) and neonatal variables (GA, birth weight, and gender) with admission to the NICU.
Results
Our study population consisted of 311 women (77 Class A1, 87 Class A2, 70 Class B, and 77 Class C-R diabetic) and their LGA infants. Of them, 195 (63%) were White, 69 (22%) were African American, 25 (8%) were Hispanic, and 22 (7%) were African or Asian. Educational level varied as follows: <11th grade, 72 (23%); high school, 179 (58%); college or postgraduate, 60 (19%). Of the pregnancies, 90% were singletons. The four twin pregnancies were dichorionic diamniotic. While 25% of the mothers were obese, 55% were extremely obese (Table 1). There were 51 mothers (16%) with preeclampsia and 28 (9%) with chronic hypertension. All 77 Class A1 women were on diet control, 46 of 87 Class A2 women were given Glyburide®, and the remaining 41 Class A2 women and all Class B and C-R women were on insulin.
Study population according to infants’ admission site.

WBN: well baby nursery; NICU: newborn intensive care unit; BMI: body mass index; GA: gestational age; SD: standard deviation; NS: not significant.
Upon arrival to labor and delivery, 226 (73%) of the 311 women intended to breast-feed, whereas the remaining 85 (27%) intended to feed formula. Of the 311 deliveries, 217 (70%) were cesarean, of which 109 (50%) were repeat operations. Common indications for the 108 primary cesarean deliveries included failure of labor to progress, breech presentation, macrosomia, and fetal distress. All infants were LGA, but 167 (54%) were also macrosomic. All mothers and their infants survived.
WBN admissions
Of the 311 LGA IDM, 160 (51%) were admitted to the WBN for an average hospital stay of 3 ± 2 days. They included 23 (24%) of 95 late preterm infants and 137 (63%) of 216 term infants. Of the 160 infants, 55 (34%) became hypoglycemic (Table 2). Of the 55 hypoglycemia episodes, 40 (73%) affected Class A2, B, and C-R infants. Of the hypoglycemia episodes, 41 occurred during the first 2 h of life, and the remaining 14 between 2 and 6 h. Only 8 (15%) of the 55 blood glucose values were ≤25 mg/dL. All infants were promptly breast-fed or fed formula. Of the 55 hypoglycemia episodes, 43 (78%) were corrected by early feeding; the other 12 (22%) required temporary IV dextrose treatment. Of the 55 hypoglycemia episodes, 29 (53%) were single low glucose values, whereas the remaining 26 (47%) had recurrences (median 2, range 2–5).
Hypoglycemia (blood glucose < 40 mg/dL) during the first 48 h of life.
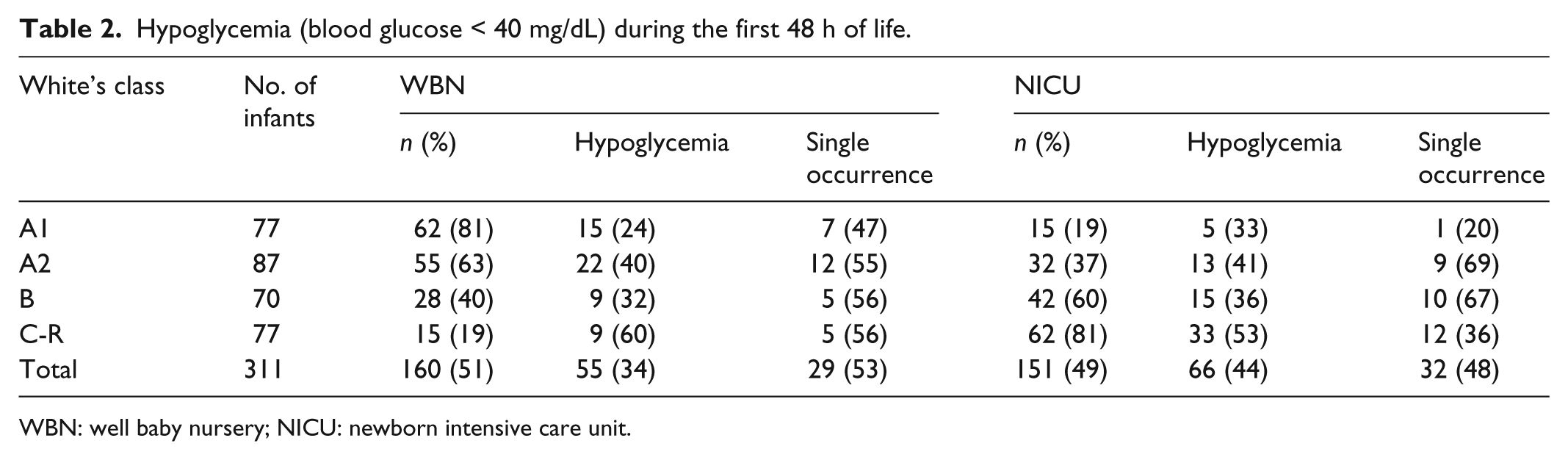
WBN: well baby nursery; NICU: newborn intensive care unit.
Eight infants with TTNB were briefly admitted to the NICU but returned to the WBN within 1 day. Three other infants with feeding intolerance were transferred to Nationwide Children’s Hospital (NCH) for diagnostic procedures but were found to be normal and discharged.
Of the 160 infants admitted to WBN, 45% were fed during the first hour and the remaining 55% during the second. First feedings were with formula except for 22 infants delivered vaginally, who were exclusively breast-fed throughout their hospitalization. One of these infants developed a single episode of hypoglycemia that was corrected by additional BF. Of the 160 infants, 153 (96%) were discharged home simultaneously with their mothers. At discharge, 24 (15%) of 160 infants were exclusively breast-fed, 52 (32%) were breast-fed with formula supplementation, and the remaining 84 (53%) were taking formula. BF initiation was higher (63%) among the 120 infants whose mothers intended to breast-feed.
NICU admissions
Of the 311 LGA IDM, 151 (49%) were admitted to the NICU for an average hospital stay of 7 ± 7 days (Table 2). They included 72 (76%) of 95 late preterm infants and 79 (37%) of 216 term infants. On arrival to the NICU, 39 (26%) of the 151 infants were hypoglycemic; they, like the remaining 112 nonhypoglycemic infants, were promptly placed on IV dextrose. Despite IV dextrose infusion, an additional 27 infants had at least one low blood glucose value. In all, 66 (44%) of the NICU infants (30 TTNB, 4 RDS, 14 late preterm, 16 from the prevention of hypoglycemia group, and the 2 infants with severe asphyxia) developed hypoglycemia. Of the 66 episodes, 32 (48%) were single low glucose values, whereas the remaining 34 (52%) had recurrences (median 2, range 2–6).
Respiratory distress was the most common admission diagnosis, involving 77 (51%) of the infants (Table 3). Eight late preterm and three term infants had RDS requiring mechanical ventilation (median 2 days, range 1–6 days) and surfactant administration. The remaining 66 (32 late preterm and 34 term) infants had TTNB: 22 needed nasal continuous positive airway pressure (CPAP) (median 1 day, range 1–2 days), 22 received oxygen only (median 0.5 day, range 0.5–3 days), and the remaining 22 required neither.
Delivery room triage of LGA IDM.

WBN: well baby nursery; NICU: newborn intensive care unit; RDS: respiratory distress syndrome; TTNB: transient tachypnea of the newborn.
In all, 72 late preterm LGA IDM were admitted to the NICU. For 40 of the infants, the primary diagnosis was respiratory distress; for the remaining 32, it was prematurity.
Of the 151 NICU infants, 41 (27%) were admitted to the NICU for prevention of hypoglycemia (3 were Class A1, 10 Class A2, 10 Class B, and 18 Class C-R). Of note, 27 (66%) of these 41 otherwise asymptomatic term infants were macrosomic. Of the 41 infants, 18 (44%) developed hypoglycemia (11 were single occurrences). In all, 38 (93%) of the 41 infants admitted to the NICU for prevention of hypoglycemia were reunited with their mothers at the WBN within 1 day. Two infants with feeding intolerance stayed in the NICU longer, and one Class C infant with meconium aspiration syndrome was transferred to NCH.
Of the 311 infants, 94 (30%) were born vaginally; of these, 18 (19%) had shoulder dystocia. None of the infants had brachial plexus injuries or fractured bones; two, however, had severe perinatal asphyxia that required admission to the NICU and transfer to NCH for therapeutic hypothermia with whole body cooling. Both infants had normal magnetic resonance studies and were discharged home at 14 days.
Of the 151 infants, 13 (9%) were transferred to NCH due to a variety of conditions. Two infants with asphyxia (described above), one with right ventricular hypertrophy, one with meconium aspiration syndrome, and another with hypoplastic left colon were transferred shortly after birth. The remaining eight infants were transferred later due to feeding intolerance (3), necrotizing enterocolitis (2), absence of the coccyx (1), severe ankyloglossia (1), and viral meningitis (1). All infants survived and were discharged home (median 28 days, range 14–86 days).
Excluding the 13 infants transferred to NCH, 109 (79%) of the 138 infants who remained in the NICU were discharged together with their mothers (remaining behind were 25 late preterm and 4 term infants). At discharge, 20 (14%) of 138 infants were exclusively breast-fed, 37 (27%) were breast-fed with formula supplementation, and the remaining 81 (59%) were taking formula. BF initiation was higher (58%) among the 106 infants whose mothers intended to BF.
Per our guidelines, the percentage of infants admitted to the NICU increased in direct relation to the severity of maternal diabetes (Table 3). Thus, as expected, the majority of NICU admissions involved Class B and C-R mothers. Univariate logistic regression showed that Class C-R (odds ratio (OR) 126.9; 95% confidence interval (CI) 28.980–555.796), late preterm (OR 9.824; 95% CI 5.826–16.564), Class B (OR 6.346; 95% CI 3.043–13.233), cesarean delivery (OR 3.619; 95% CI 2.267–5.778), and macrosomia (OR 2.994; 95% CI 1.481–6.053) were strongly associated (p < 0.0001) with NICU admission. Conversely, infants born to Class A1 and A2 mothers were less likely to be admitted to the NICU. Multivariate analysis reaffirmed the strength of Class B and C-R as predictors of NICU admission even after controlling for other variables (macrosomia, prematurity, and diabetes Class B and C-R).
Discussion
The incidence of diabetes complicating pregnancy continues to rise around the world.4,14 Thus, it may be anticipated that the rate of NICU admissions will increase—especially for LGA and macrosomic IDM.1,4,8,9,18 Undeniably, specialized care is beneficial and even lifesaving for many LGA IDM; however, this must be balanced against the potential disruption of maternal–infant contact, which could negatively impact BF initiation and attachment.5–9,18,19 Recently, a more liberal management has led to an increase in admissions of vulnerable but asymptomatic infants (i.e. preterm, LGA, IDM, etc.) to WBN or to intermediate care facilities.8,12,13,20,21 Since maternal–infant interactions (early BF, bonding, attachment) are maximized under these conditions, it is not surprising that BF initiation was lower among infants in the NICU as compared with that among those admitted to the WBN.8,10–11,22,23 Whether this is the result of mothers’ concern for the health of their infants, anxiety, stress, delayed lactogenesis, or a combination of all these factors is still debatable.5,15,24 Furthermore, in a population of women who often undergo cesarean delivery, it is unrealistic to expect early extended skin-to-skin contact between mother and infant. 7 In spite of these considerable obstacles, we have observed that intention to BF often overcomes all and that initiation of BF occurred.7–11
Respiratory distress, prematurity, and hypoglycemia are consistently recognized as NICU admission diagnoses for both LGA and non-LGA IDM.1,3,4,8,10,11,25,26 The high incidence of TTNB observed in our study may be related to the rate of cesarean deliveries, whereas the low occurrence of RDS suggests later gestational delivery. The prompt resolution of respiratory distress and the successful initiation of oral feedings among the late preterm infants we observed may indicate a potential for shorter NICU stays and an earlier return to the WBN.
Recent efforts have reduced the proportion of late preterm births in the United States, although these births increased from 7.3% to 9.1% from 1990–2005. 26 In order to avoid the risk of stillbirth or major complications, late preterm delivery of LGA IDM may be indicated. Hence, late preterm infants, especially those who are LGA IDM, remain a group at risk for morbidities that require admission to NICU, prolonged hospital stay, and low BF initiation.2,19,25,26 Our data showed that at least 25% of asymptomatic late preterm LGA IDM infants could be safely triaged from the DR to the WBN.
In some medical centers in the past, LGA or macrosomic IDM whose mothers were on insulin (Class A2, B, and C-R) were routinely admitted to the NICU for detection, prevention, or treatment of hypoglycemia.1,22 Clearly defined hypoglycemia surveillance programs and the benefits of early feedings of infants at risk provide an alternative to universal NICU admission of otherwise asymptomatic infants.2,8,10,11,27,28 Harris et al. 2 reported that the independent risk factors for neonatal hypoglycemia were LGA (47%), late preterm (54%), and IDM (48%). Of note, seven of eight infants in that study who had all three risk factors suffered more frequent and severe hypoglycemia. Our data do not corroborate that observation, however, as hypoglycemia occurred in only 45 (47%) of the 95 infants who were LGA, late preterm, and IDM.
It is worth noting that the most recent publications report single low glucose episodes, few recurrences, and rare cases of symptomatic or refractory hypoglycemia.2,8,10,11,27 Our data demonstrate that hypoglycemic episodes among LGA IDM in the WBN occurred between 1 and 4 h of life and, more importantly, that the majority were corrected with early BF or formula feeding.8,10,11,27,28 It is also possible that the low recurrence of hypoglycemia may be an additional benefit of early feedings.8,10,11,20,22,27 The low incidence of hypoglycemia among IDM who were exclusively breast-fed is encouraging but remains preliminary.20,27
Based on our experience, we discourage NICU admission of asymptomatic LGA Class A1 and A2 infants for prevention of hypoglycemia. Since hypoglycemia among LGA IDM increased in direct relation to the severity of maternal diabetes, our guidelines still recommend NICU admission for asymptomatic LGA Class B and Class C-R IDM.1,2,8,10,11,22
Limitations of our investigation are those inherent in retrospective studies and related to the difficulties of standardizing clinical care for a population of extremely high-risk infants.
Summary
Asymptomatic LGA IDM born to mothers with Class A1 and Class A2 diabetes can be safely triaged from the DR to the WBN. Although hypoglycemia affects some of these infants, the overwhelming majority of the episodes can be corrected by early feeding. NICU admission based on the recognition of common morbidities appears feasible and safe. Moreover, identification of infants who require transfer for further specialized care can be accomplished in a timely fashion. Finally, decreased disruption of maternal–infant interaction and simultaneous discharge from the hospital may improve BF initiation rates, especially for those mothers who intend to breast-feed.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.