
Abstract
This paper provides a review of the importance of primary care psychiatry within an Australian context. The aims of this review are: (1) to emphasize the integral role of mental health in overall health and well-being, (2) to elucidate the factors that make the provision of primary care psychiatry essential, and (3) to review the impact of the Australian government’s mental health policy initiatives on the mental health of the Australian population as well as on the practice of primary care psychiatry. From this review, it is evident that the discipline of psychiatry is integral to the overall health of the community. Furthermore, it is apparent that primary care psychiatry has a large and pivotal role to play in the prevention, treatment, and early detection of mental disorders in Australia and worldwide. The article concludes with some simple, actionable recommendations for the practice of primary care psychiatry.
Keywords
Introduction
The findings of 2 National Surveys of Mental Health and Wellbeing (NSMHWB) indicate that the rates of mental disorders within Australia have remained high and stable throughout the decade.1,2 This finding is despite the Australian government targeting mental health (MH) as a priority area since 1993. 3 Governmental policy highlights the importance of general practice (GP) in the provision of MH care, as GP acts as the gateway into the medical sphere. 3 Although almost half of the Australian population has suffered from a mental disorder in their lifetime; the majority of individuals unfortunately do not seek help or receive the treatment that they need.1,2 Essentially we are failing to reach those who are the most in need; consequently, individuals, families, and society are continuing to suffer from the impact of mental disorders.
The purpose of this article is 3-fold: first, to emphasize integral role of psychiatry in promoting and maintaining the wellbeing of the community; second, to elucidate the factors that makes the provision of primary care psychiatry (PCP) essential; and last, to review the impact of Australian policy initiatives on the MH and well-being of the Australian population. The article concludes with some recommendations to enhance the effectiveness of provision of PCP services in GP.
The Relation between Health and Mental Health
Since the 17th century, progress in medical science has been remarkable; knowledge pertaining to the workings of the body and the effects of diseases has advanced immensely. 4 Respectively, there have also been vast increases in life expectancy rates and reduced mortality from infectious diseases in developed countries. This trend is attributable to not only medicine, but also advancement in sanitation and general living conditions. 5 The only exception to this decrease in mortality rates from infectious diseases came about with the emergence of HIV/AIDS. 4
The reduction in infectious diseases changed the burden of disease, and chronic diseases such as heart disease, stroke, and cancer increased. 5 Thus these changes in the burden of disease lead to the reconceptualization of the nature of health. As before, the aims of public health had been to avoid death as a result of infectious diseases; hence, the notion of health was defined in negative terms as the absence of disease. This definition is also in accordance with the dominant model in medicine, the biomedical model. This model views disease as being accounted for entirely by variations from the biological norm. 6 However, with the emergence of chronic diseases with more complex etiology, the emphasis started to be placed on the positive aspects of health in order to circumvent the impact of these chronic conditions.
The 1948 Constitution of the World Health Organization (WHO) defines the concept of health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” 7 Since the delineation of this term in 1948, the conceptual definition of health by the WHO has remained unchanged. The focus on the positive aspects of health is further reflected in the WHO’s changes to the measurement of the Global Burden of Disease (GBD) from mortality rates to the Disability-Adjusted Life Years (DALY). 8 The DALY measures the number of years of life lost as a result of premature mortality coupled with years of life lost as a result of ill health. 8
This conceptualization of health is incongruent with the traditional biomedical model of disease, which focused primarily on physical health and is aligned with the opposing biopsychosocial model of disease. The biopsychosocial model postulates that biological, psychological, and social factors are all important determinants of health and that diagnosis, treatment, and prevention of disease should consider the interaction of these determinants. 6
Miettinen and Flegel attempted to revise the conception of health in line with the traditional biomedical model by removing the realms of mental, social, and well-being from the definition. 9 Thus their conception of health is centered on the domain they view as treatable by a medical practitioner being the “physical,” or rather, “physical diseases.” This attempt at redefining health highlights the disagreement between the 2 opposing dogmas in medicine.
Irrespective of Miettinen and Flegel’s reconceptualisation of health, 9 disease can be defined as “a disorder with a specific cause (which may or may not be known) and recognisable signs and symptoms,” as well as “any bodily abnormality or failure to function properly.” 10 The notion of disease in this definition is not confined to the physical or mental realm; rather, they are disorders that affect the mind or body that are recognizable through a common taxonomy of symptoms that in turn impede “normal” functioning. Hence, there can be diseases that affect the body as well as the mind.
More recently Ngui et al have called for more effective strategies and initiatives that incorporate MH as a vital component of health. 11 Also, the WHO and the World Organization of Family Doctors (WONCA) emphasized that health workers have been overly focused on physical disorders to the detriment of MH. 12 Therefore, it is fundamental that the concept of health is not fragmented by ignoring integral and influential components of health, namely MH.
The notion of MH, in accordance with the WHO definition of health, 7 is not defined merely as the absence of mental disorder or impairment; rather, the term MH is meant to refer to a wider sense of well-being. The concept of MH is related to our emotions, thoughts, and behaviors and is strongly related to our ability to function in our everyday lives. That is, a person with good mental health has the ability to generally deal with day-to-day obstacles and function successfully in society. 3
On the contrary, individuals who have poor MH and suffer from mental disorders have difficulty handling day-to-day issues and do not have the ability to function well within society. Mental disorder can be defined as a harmful dysfunction; that is, the individual suffers from a personal dysfunction that is behavioral, psychological, or biological in nature or a combination of these entities. 13 This dysfunction is clinically recognizable by a set of symptoms, and the individual’s affliction is viewed as harmful or a deviation from the cultural standards. 13 Hence, referring back to the definition of disease, it is apparent that mental disorder adheres to the criteria of the definition, that a mental disorder is a disorder with a cause that may or may not be known that is recognizable by a taxonomy of symptoms that impedes proper functioning.10,13
Mental disorder, in addition to causing pain, distress, and disability to the individuals that are suffering from them, also affects the individual’s family and friends along with the broader community. Henderson et al. report that anxiety, affective, and substance use disorders contributed to almost 6 million sick days per month in 1997 in Australia. 14 Furthermore, it is thought that the problem will further increase over the next 10 years, with depression projected to be the second highest burden of disease globally by 2030.15,16
Traditionally mental disorders have been the domain of psychiatry. Psychiatry is defined as “the study of mental disorders and their diagnosis, management and prevention.” 10 However, as long ago as the 1950s, with the advent of deinstitutionalization, the philosophy of care of the mentally ill moved to a community-based paradigm. 17 Unfortunately, this transition was far from smooth, and many mentally ill individuals were displaced and failed to receive the care that they required.17,18
More recently, it has been advocated that MH should become an integral component of primary care, as all individuals have the right to quality MH care. Furthermore, the provision of MH services through primary care should facilitate reaching those individuals who have previously gone untreated. The following section discusses the ideology of PCP and highlights both the pragmatic and idealistic reasons why the provision of PCP is a fundamental component of GP.
Primary Care Psychiatry
Primary care refers to services that are delivered at the general health care level, that is, medical services that are delivered by a non-specialized physician or health professional. 19 Primary care physicians act as the gatekeepers into the medical sphere, and within industrialized societies, this role is undertaken by general practitioners (GP). General practitioners, in addition to with acting as gatekeepers, are responsible for the provision of most ambulatory care for diverse range of illnesses. Primary care services for MH ideally should incorporate the early identification of mental disorders; care for individuals with common mental disorders (anxiety, affective, and substance use disorders); management of individuals with more serious mental disorders that are stable; care for the MH needs of individuals with physical conditions; as well as the promotion of MH within the community. 12 Primary care is the first contact that the patient makes with the medical system.
The need for PCP, apart from being advocated by policy, is also facilitated by a number of pragmatic factors.12,20 In addition, there are also issues pertaining to the “best” care for the patient, along with where the majority of patients with mental disorders go to seek help. The practical issues are all centered on the central issue pertaining to the accessibility of psychiatric services. 21-23
First, it is apparent that there is a global shortage of psychiatrists. This shortage is especially prevalent in developing nations, where mental health workers are migrating to more developed nations, but it is also prevalent in Australia.21,22 However, even in developed nations, accessibility is limited by the geographic distribution of psychiatrists. The vast majority practice in metropolitan areas, which means that there is a void in psychiatric services in rural and remote areas. 23 Additionally, there has also been an increase in the number of psychiatrists working part-time, limiting the number of provider hours being worked. 23
Second, even if there are psychiatric services that can be accessed, there is a disparity in the individuals that have the ability to access them. The lack of access to public sector psychiatrists is well recognized by the profession in Australia, and psychiatrists in the private sector charge above the scheduled fee. 23 Ultimately, individuals who are the most disadvantaged in society, and thus are more prone to MH issues, are unable to obtain the assistance they require.
Further compounding this shortage of psychiatrists is the trend to discourage medical students from furthering their education in psychiatry and thus becoming psychiatrists. 11 Therefore, it is evident that through the promotion and supply of primary care psychiatry, MH will be much more readily supported within the general population. Thus there will be an ability to provide a more affordable mixture of primary and secondary care psychiatric services as needed. 20
In relation to “best” practice, the provision of PCP has the potential to reach the broader community, as most individuals see a GP. General practitioners are the first point of contact and may be the only form of contact for many individuals. 24 Seeing a GP also facilitates an integrated treatment approach for individuals’ psychological and physical needs. 12 The provision of PCP additionally assists with the continuity of care that individuals with mental disorders critically require. 24 Most importantly, though PCP is facilitated by the patient-centered interaction that should occur in GP, this treatment approach builds rapport and trust between the physician and the client.25,26 This patient-centered approach improves health outcomes as well as encouraging continuity of care.25,26
A further issue pertaining to “best” practice and the GP being the principal point of contact is the opportunity for early intervention for individuals with mental disorders, if primary care physicians are well equipped with the knowledge and skills necessary to identify common mental disorders. 27 Having these skills will facilitate early intervention, which also leads to better patient MH outcomes. 27
Policy Initiatives Related to the Provision of PCP within Australia
It is evident that MH is a fundamental component of overall health and that worldwide, not just within Australia, there are not enough psychiatric services to meet the growing MH needs of the general population. Coupled with the issues related to accessibility, there are issues pertaining to “best” practice and quality of care that need to be addressed in PCP. This section will review the policy initiatives related to MH and PCP within Australia that have been implemented since the early 1990s.
To overcome the limitations pertaining to access of psychiatric services and to promote “best” practice, the Australian government has formulated a number of policies aimed at moving toward a more collaboratively based MH care framework that is reliant upon PCP. Within this framework, PCP is fundamental in coordinating and providing care for the MH needs of the Australian population. A brief summary of the policies that will be discussed can be viewed in Table 1. After a brief discussion of the pertinent policies, the focus will turn to the overall outcomes of these initiatives.
A Summary of Australian Policy Initiatives Relevant to Primary Care Psychiatry
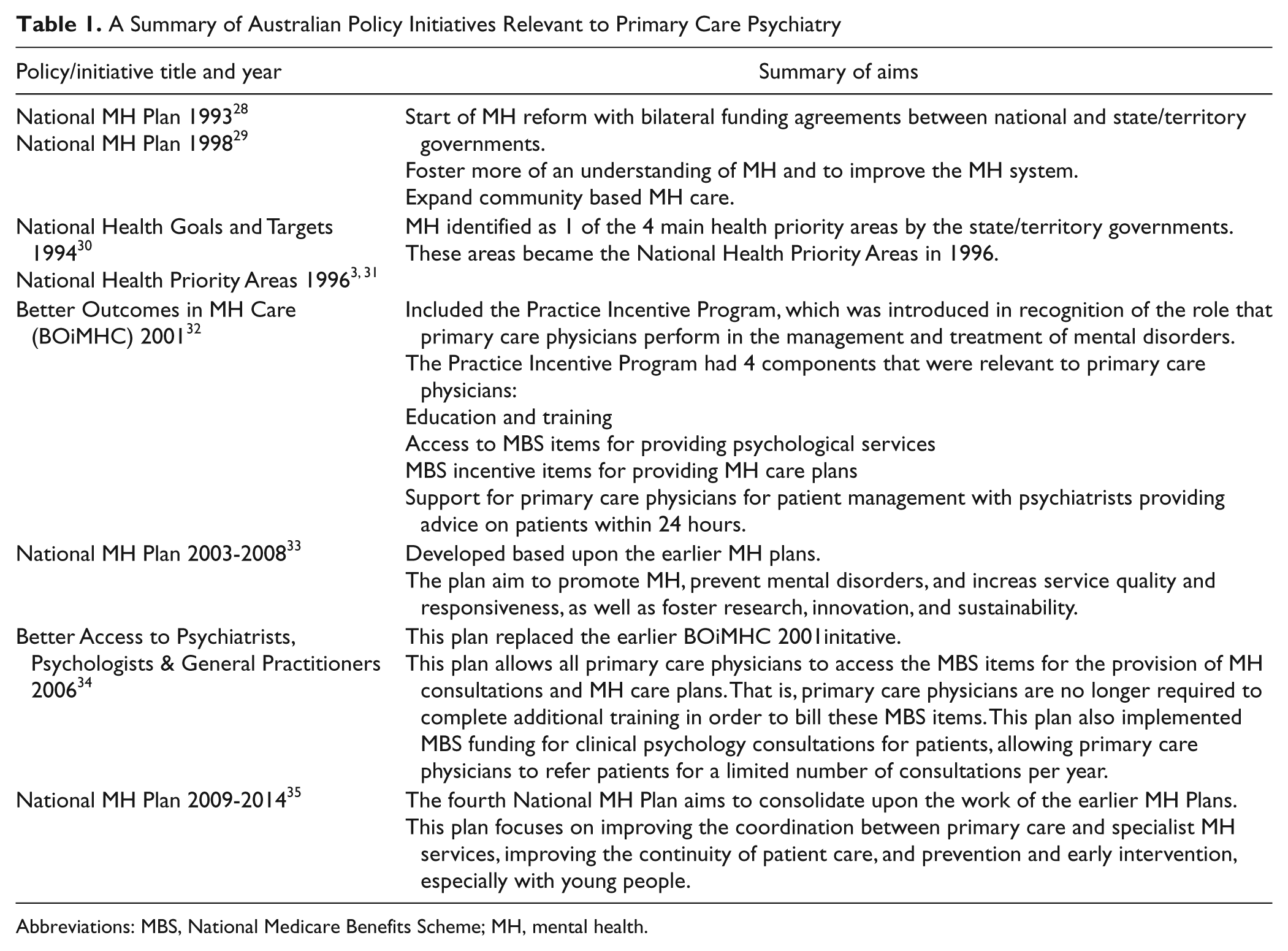
Abbreviations: MBS, National Medicare Benefits Scheme; MH, mental health.
The health system in Australia is the domain of the federal and state governments, as well as the private sector. 28 In Australia, the federal government funds Medicare, which is a national scheme that subsidizes most primary care, pharmaceuticals, as well as some private specialists. 29 Additionally, because of the fiscal control of the federal government, Medicare also provides the state governments with funds for health expenditure. 29
The initiation of MH reform in Australia commenced with the first National MH Plan in 1993 aimed at improving the MH care system and our understanding of mental disorders. 30 Mental health was then named as 1 of our 4 health priority areas in 1994.3,31 The second National MH Plan was rolled out in 1998 with similar aims as the first, of promoting MH and expanding community-based MH care.30,32 The third National MH Plan,which was based on the earlier 2 plans, was implemented in 2003. 33 It included the additional aims of prevention, improving service quality, and fostering research on MH. The most recent National MH Plan, implemented in 2009, aimed at consolidating the work of the previous 3 plans. 28 With the additional objectives of improving coordination between primary care and specialist MH services, continuity of patient care and a focus on prevention and early intervention, especially in young people.
In addition to the bilateral agreements stipulated in the National MH Plans,28,30,32,33 a number of other MH initiatives undertaken during this time are worthy of discussion. Most notably, the Better Outcomes in MH Care (BOiMHC) 34 and the Better Access to Psychiatrists, Psychologists, and General Practitioners 35 initiatives had the most fundamental impact on the PCP.
The BOiMHC policy included a number of components relevant to PCP practice. These components were centered around increasing remuneration for eligible primary care physicians, as well as providing them with extra support and training. 34 Specifically, GP were eligible to access extra item numbers under the National Medicare Benefits Scheme (MBS) if they had completed the required education and training courses. 34 In other words, the government introduced a higher fee schedule available under the MBS to more adequately reflect the time and skills required for an MH consultation. This increase in remuneration reflects the complexity of an MH consultation, as well as acting as an incentive to primary care physicians to provide PCP services. 34 In order to receive these additional benefits, practitioners had to complete training in psycho-education, cognitive behavioral and interpersonal therapy. 34 The BOiMHC policy also included extra support for GP by providing remuneration to psychiatrists to support GP with patient management advice within 24 hours of their query. 34
The Better Access to Psychiatrists, Psychologists, and General Practitioners initiative then superseded the BOiMHC initiative in 2006. 35 The most important differences between the 2 initiatives were that primary care physicians no longer had to undertake additional training to be able claim the MH MBS item numbers.34,35 The other most significant difference was the provision of MBS-funded psychological services, thereby allowing GP to refer their patients to clinical psychologists. 35
The Current Status of MH within Australia
As can be seen from the above summary of selected Australian government policy initiatives,30-37 it could be argued that the Australian government has made a concerted effort to deal with MH issues in Australia since the early 1990s. However, are these policies resulting in the outcomes they were envisioned to achieve?
Hickie and colleagues ascertain that although Australia has been a global forerunner in the development of MH population-based policy, these policies have not been widely implemented, which thus constrains the advancements that have been made to date. 38 Furthermore, Griffiths supports Hickie and colleagues’ view advocating that even the harshest critics of the Australian MH system could not question the content and relevance of the MH policies and initiatives.38,39 Griffiths also blames the failings thus far on issues related to implementation, 39 specifically, a lack of commitment and investment on behalf of the federal and state governments.
Obviously, even the best policies, if not implemented, will not make an impact on the MH of the Australian population. A report written by the Mental Health Council of Australia, 40 a peak nongovernment organization, entitled Not for Service states that the Australian government has lost its way with MH initiatives since the advent of the First National MH Plan. 30 The First National MH Plan specifically advocated for the rights of individuals with mental illness and their caregivers. It moved care out of asylums and developed, but more importantly, supported, the prevention and treatment of common disorders. 40 Since this time, the report describes in detail the systematic failure of the MH system in Australia, with consumers not being able to access services and when they do gain access, their basic human rights are violated. 40
However, it must be recognized that some of the policy initiatives described above have assisted the plight of MH consumers in Australia. For example, the BOiMHC 34 and the Better Access 35 schemes both provided more grass-roots support to GP for the provision of PCP services. On the other hand, the change from the BOiMHC 34 to the Better Access 35 scheme meant that physicians were no longer required to complete mandatory training in the provision of MH services. Clearly this change is not in the best interests of consumers, and it compromises the quality of care provided.
A study conducted by Hickie and colleagues found that 50% of individuals with a mental disorder in Australia are not recognized as having a mental disorder by their GP. 41 More recently, Wilhelm and colleagues highlighted the need for physicians to attend to the somatic complaints of their patients, as patients are more willing to explain their psychological problems through somatic symptomology. 27 These issues pertaining to the diagnosis of mental disorders are more alarming because of the high rates of comorbidity of physical conditions with depression and anxiety.1,2 As these individuals with a comorbid mental disorder and physical condition are presenting to their GP, an opportunity to capitalize on early intervention is missed.1,2
On the contrary, Bushnell and Collings found that GP are more likely to diagnose a mental disorder in patients who attend their practice more frequently and exhibit higher levels of disability.42,43 Bushnell found that GP were more likely to formulate their MH diagnostic decisions over multiple visits as opposed to single consultations. 42 The association between diagnosis and level of disability is commonsensical. 43 However, it is important that GP are aware of these associations between diagnosis of a mental disorder, frequency of consultations, and level of disability in order to promote prevention and early intervention.42,43
This move away from mandatory training, although it appears to increase accessibility, has compromised “best” practice. Therefore, accessibility to MH services has been increased at a significant cost. Although on the surface, it appears as though all Australians have equal access to PCP services in GP and other mental health professions as a result of the MBS, this is unfortunately not the case.
It is evident that more individuals from socioeconomically advantaged and metropolitan areas are using these MH initiatives.44,45 This difference may result from 2 factors, the geographic distribution of services as well as the out-of-pocket expenses that are now commonplace. More GP and MH professionals practice in more advantaged and urban areas as opposed to less advantaged, rural, and remote areas.44,45 Second, GP and other MH professionals are charging above the MBS-scheduled fee and therefore require a copayment from the patient.44,45 The prior BOiMHC initiative provided preferential access to these individuals from socioeconomic, geographic, and demographic backgrounds that had difficulty obtaining access to MH care. 46
A third factor in relation to accessibility is the trend in service use. It is apparent that more females than males are using these MBS MH services, and the vast majority are between 25-44 years of age. 47 This service use is in opposition to those who require the services the most, as well as those who are at the most risk. For example, men have much higher rates of suicide than women, and the majority of mental disorders have their onset before 18 years of age.45,47 It is also apparent that these services are also underused for indigenous Australians and Australians from culturally and linguistically diverse backgrounds. 45 These trends in service use are partly at odds with what the government was aiming to achieve, especially in respect to prevention and early intervention.
The provision of preventative and early intervention strategies have been highlighted in a number of the Australian government policy initiatives.30,32-35,37 Unfortunately, these initiatives have failed to reach fruition. Mental diseases, known to be a critical health issue afflicting young Australians, cause a high and enduring amount of disability. 47 As already stated, the majority of mental disorders have their onset in adolescence, however, we are failing to reach this group. 47 McGorry and colleagues state that the Australian government has failed to view young people as a distinct group that requires specialist intervention services. 47 Furthermore, adolescents are caught between pediatric and adult MH service delivery modes, and neither suits them. 47 Therefore, it is apparent that GP need to be attentive to the specialist needs of this age group.
Although distribution of the uptake of these services is not equal, the Better Access scheme has provided a necessary and valued endeavor with the provision of MBS-funded psychological services. 35 Previously, only a small segment of the Australian population could afford access to psychological services; now, with the provision of the services under the MBS, a broader segment of the Australian population has access to psychological services. This provision of MBS-funded psychological services has been called for by primary care physicians and MH professionals for a number of years. 40 In relation to PCP, this policy allows physicians to refer their patients to psychological services, thus lessening the burden on GP and increasing the recovery outcomes of the patient.
On the contrary, the Better Access scheme has been criticized, as a mere referral to another MH professional does not constitute collaborative care.35,46 It has been argued that the move from the BOiMHC initiative to the Better Access scheme has decreased collaborative care.35,46 It is apparent from the brief review and discussion of the Australian government MH policy, as it pertains to the provision of PCP services, that a lot more remains to be done to provide better MH services to the Australian population. It is hoped that the current National MH Plan will satisfy its objectives, 37 hence fostering a more collaborative care system coordinated through GP, to increase the continuity of care of consumers with mental disorders and their caregivers.
Conclusion
From the above review of the concept of health, it is evident that MH plays an integral component in the overall health and well-being of the individual. Although the Australian government has been actively seeking to alleviate the burden of mental disorders within Australia since 1993 through policy initiatives,30-37 it is apparent that these endeavors are not making the required gains. Although it is argued that the Australian government has been a global forerunner in the development of policy, these policies have not been properly implemented.38,39 To better support the Australian population’s MH issues, the Australian government needs to further invest in MH and support this investment with a determined commitment.38,39
Besides policy advocating for PCP, it is also necessary in terms of accessibility and “best” practice models for the provision of MH care. Therefore, it is fundamental that the importance of PCP is recognized and implemented within practice by all primary care physicians. In addition to recognizing the need for PCP, it is crucial that primary care physicians have the knowledge and skills necessary to provide quality PCP services. It is apparent from the above critique of MH policy and PCP in Australia that there are specific groups of individuals and factors of which primary care physicians should be aware in order to provide quality PCP. These key issues for the practice of PCP are summarized in Table 2. It is going to take a multifaceted approach from governments, primary care physicians, and MH professionals to alleviate the burden of mental disorders on the individual, family, and community within Australia and worldwide. It is only through such a comprehensive approach that we can support the MH, physical health, and well-being of society.
Some Recommendations for the Provision of PCP

Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.