
Abstract
Informed consent in the veterinary sphere has been surprisingly under-researched, despite it being a professional ethical requirement. As consent is given by animal owners on behalf of patients who are unable to consent for themselves, its underpinning ethical basis cannot exactly mirror consent given by adult human patients with capacity. Any attempt to research consent in the veterinary context requires consideration of its legal, ethical and practical applications. This investigation of consent practices in veterinary settings in the United Kingdom was undertaken using interpretation of medicolegal cases, together with three discrete empirical studies comprising the textual analysis of consent forms, consent discussions for the elective neutering of companion animal patients, and interviews with key participants in the consent process. The chosen approach required a methodology that would facilitate triangulation between empirical data analysis and doctrinal legal research. Here, I describe the first use of interpretive description as a methodology of veterinary socio-legal studies, in the context of practice-based research. With foundations in traditional social science methodologies such as hermeneutics, grounded theory, ethnography and symbolic interactionism, interpretive description provided a multi-disciplinary methodological perspective. Its underpinning methodologies informed the methods that were used for data collection, and for subsequent analysis. I combined interpretation of legal decisions and professional ethical guidance with thematic surveys of empirical data to reach higher levels of analysis. The resulting conceptual description of consent in veterinary practice enabled the production of normative guidance appropriate for those in practice, thus fulfilling the methodological aims of interpretive description. Specifically, the key findings were that the consent form should act as a fuller record of the consent discussion, that attention should be paid to achieving an appropriate balance between client autonomy and patient ‘best interests’ and that consent should provide protection to all three parties (client, patient and veterinary professional).
Introduction
In the United Kingdom, the informed consent of the animal owner is required before any treatment is given to animal patients. As stipulated by the Royal College of Veterinary Surgeons (RCVS), the regulatory body for the veterinary profession in the United Kingdom,
Veterinary surgeons must communicate effectively with clients, . . . and ensure informed consent is obtained before treatments or procedures are carried out. (RCVS, 2020a: 2.4)
However, obtaining informed consent to the treatment of animals is fraught with ethical difficulties. These include the fundamental problem that the person giving consent is not the patient undergoing treatment. Accordingly, consent based on the autonomy of the patient, as is predominantly the case in medicine, is unsuitable for the veterinary context (Ashall et al., 2018; Gray et al., 2018). In addition, as veterinary medicine is a private form of healthcare, the veterinary practice–client relationship is contractual. Indeed, the RCVS specifically links consent and contract, confirming that ‘(i)nformed consent, . . . is an essential part of any contract’ (RCVS, 2020b: 11.2).
Despite a dearth of literature examining informed consent in veterinary practice, previous authors have approached the subject from a normative viewpoint, outlining the processes that should be followed to obtain consent. Key papers by Fettman and Rollin (2002), Flemming and Scott (2004), and Passantino et al. (2011), describe how consent should be obtained from a medico-legal perspective, while resisting critical evaluation of these requirements. However, relatively few empirical studies of veterinary consent have been conducted, with some replicating previous studies in medicine. For example, Whiting et al. (2017) used a questionnaire to investigate the perceptions of consent among clients at a large veterinary hospital, finding that the majority of respondents considered that the process provided protection to the hospital in case of negligence.
Compared to human medicine, there is a dearth of knowledge regarding the veterinary informed consent process as it happens in practice, including its purpose and ethical foundations. This perceived gap in research inspired the design of an inter-disciplinary and mixed methods study that aimed to capture the essence of consent in veterinary practice, analysing it from a combination of ethical, social and legal perspectives. The empirical work utilised routine neutering of companion animals (dogs and cats) as a case study, based on the routine and ubiquitous nature of these procedures. As a veterinary surgeon with an interest in practice-based research and experience of teaching clinical communication skills, I brought my own perception of what a ‘good’ consent process would look like, and how it might be achieved through effective communication, thereby ensuring a good outcome for the animal patient. However, I was passionate about finding out what was actually happening in practice, how those involved conceptualised consent, and how decisions were made by both human parties on behalf of the animal patient. This involved soliciting the views and beliefs of participants in the process and comparing these with observations of consent processes as they were conducted in practice, thus requiring an approach that was fundamentally social science-based and qualitative in both methodology and analysis.
The broad aims of my research were therefore to capture the essence of consent to treatment in the context of planned elective surgery, to analyse the practical approach taken to consent and, based on the findings from these analyses, to formulate guidelines for practice. Achieving these aims required an approach incorporating multiple perspectives; for example, interrogating the roles of the consent form and the accompanying discussion which combine to produce an ‘informed’ consent, and soliciting the views of key participants regarding what constitutes an ‘ideal’ consent process. These perspectives, combined with the contribution from doctrinal legal research, would characterise the meaning, purpose and processes of consent in the veterinary medical setting, and the construction of how consent is, and how it should be, obtained in the ‘real-world’ clinical context.
Having decided on a qualitative approach, I next had to evaluate the intended research audience. Several previous studies of veterinary communication-related topics have used positivist, objective approaches with some success. Techniques such as careful coding, measuring and quantifying of video transcripts of veterinary consultations have produced meaningful results; for example, Shaw et al. (2004) pioneered the use of the Roter interaction analysis system, which gives a numerical value to each segment of a video-recorded interaction, in the veterinary context. While acknowledging the usefulness of such an approach, my research questions required eliciting participants’ beliefs and values; for example, what should be in a consent discussion? The participants’ own experience of the consent process was, therefore, fundamental to the answer, and required more than objective measurement.
Previous qualitative studies in the veterinary context have yielded valuable and influential results. Among the overwhelming predominance of quantitatively designed studies in veterinary science, an increasing number of papers have reported the use of qualitative methodology, although reporting is sometimes limited to the methods used, with little or no methodological explanation. One common approach utilises a qualitative method (e.g. interviews) to provide information for a subsequent quantitative study, such as a questionnaire. It is less common to find ethnographic methods such as observation or case studies, although these have been used for investigating the giving of behavioural advice during consultations (Roshier and McBride, 2013), the relationship between errors in practice and teamwork (Kinnison et al., 2015), and communications training interventions for veterinary surgeons (Bard et al., 2017). The trend towards increasing use of qualitative methods in veterinary research demonstrates a greater acceptance of qualitative methodology for practice-based research and therefore confirms my choice of approach, which was designed to combine traditional doctrinal legal research (analysis of veterinary and medical case law pertaining to informed consent) with a three-branched empirical study. The latter aimed to explore (1) the role and content of the consent form (2) the contents of the consent discussion and (3) the views of those involved in the consent process.
Philosophical approach to research
In an attempt to identify a philosophical basis that would underpin both doctrinal legal research and the tripartite empirical work, I investigated potential epistemological and ontological pathways.
Epistemologically, the best fit for my study seemed to be social constructionism, which acknowledges the existence of multiple realities depending on the individuals involved, the context of the investigation, the analysis undertaken, and the involvement of the researcher. As knowledge would be created through the process of my research, through interpretation of ‘informed consent’ by key participants, and through attempts to discover its meaning via its documents, events and activities, it was ‘constructed in and out of interaction between human beings and their world’ (Crotty, 1998: 42).
The choice of ontological basis was more problematic. While a realist ontology may align with aspects of legal research, in that the law has an objective reality, and laws are ‘material and concrete phenomena’ (Silbey, 2013: 25), legal study contains a strong relativist component, with interpretation of legal rules seen as subjective (Hutchinson and Duncan, 2012). A realist ontology is given further support by the RCVS, which requires consent forms to be used in specific situations (RCVS, 2020b), thus giving consent a professional ethical reality. Conversely, participants give meaning to consent by the use of language, suggesting a relativist ontology. As neither seemed suitable as a single ontology, my solution was to incorporate a dual ontology, supported by Crotty’s (1998: 63–64) proposal that both realism and relativism can be applied to a constructionist approach.
Finally, the analysis of both judicial decisions and empirical data seemed to fit with an interpretive approach. Consent depends on the language used by the person giving the information, and how it is interpreted by the receiver. Interpretation, in turn, depends on previous experiences in similar and contrasting situations, which could also be applied to participants’ understanding of consent in interviews. Furthermore, the analysis of medico-legal decisions, professional ethical guidance and the language used on consent forms suggested an interpretivist construction of informed consent.
Interpretive description methodology
The choice of a social constructionist and dual ontological approach to data collection combined with an interpretive approach to analysis required an appropriate methodology, which could be applied to the multiple disciplines of law, professional ethics and sociology. Interpretive description, developed to cater for the health professions’ specific requirements for knowledge in situations combining care with clinical and scientific medicine (Thorne, 2016; Thorne et al., 1997), seemed to fulfil the criteria. This methodology is designed to provide the coherence and integrity of the theoretical approach with the design variations required by the ‘context, situation and intent’ (Thorne, 2016: 16) of the disciplinary setting. In borrowing from several of social science’s foundational methodologies, such as ethnography, grounded theory and phenomenology, it imports methods for data collection and aspects of data analysis from each, while avoiding strict adherence to their philosophical traditions, or the wholesale adoption of the theoretical drivers used for most social science research.
Other donor methodologies have been added to the list, including symbolic interactionism. The latter’s purpose of ‘understanding how individuals and groups make meaning and act in situations in which automatic responses are inadequate’ (Oliver, 2011: 411) matches the world of practice problems that led to interpretive description’s creation. Furthermore, it requires that to understand something, it must be investigated in a natural setting, as was the case for the observed consultations. To understand policy, its effect on those whom it influences must be investigated; this was achieved through my interviews with key practitioners, who could be regarded as Blumer’s ‘acute observers’ who are ‘well-informed’. (Blumer, 1969: 41). Symbolic interactionism was therefore a key underpinning methodology for my studies
Although more difficult to identify a donor methodology for doctrinal legal research, due, in part, to the lack of explicit methodological discussion by many researchers in this domain (Hutchinson, 2015), it became clear to me, as a non-lawyer, that hermeneutics (from phenomenology) was fundamental to the interpretation of legal decisions (Van Hoecke, 2011).
Legal research methods
Reliance on the interpretive aspect of legal research increased its potential contribution to subsequent empirical analyses. In addition to relevant case material, analysis of professional ethical guidance, often described as ‘soft law’ (Mörth, 2011) contributed to my overall understanding of how findings or guidance may translate into practice, especially when exploring how this guidance impacts on veterinary professionals and how it is often influenced by personal ethics. These aspects would be investigated with interview participants.
Following the suggestion that legal researchers could learn from the structure and methods of systematic reviews to make case selection transparent (Baude et al., 2017), I formulated a suitable search strategy for doctrinal research, using on-line legal databases (Lexis Library UK, 2016; Westlaw UK, 2016). The initial search terms of ‘Veterinary’ AND (medicine OR treatment) AND ‘informed consent’ yielded 17 negligence-based cases, of which only two contained specific reference to consent. Widening the search terms to ‘Veterinary’ AND ‘negligence’ left 8 cases deemed relevant for further analysis, but none of the cases turned on informed consent, or failure to obtain consent. The lack of suitable cases from veterinary medicine was not unexpected, as few cases from this arena reach the higher courts, primarily due to the relatively low value of animal patients (Fox, 2012).
Refocusing my search on human healthcare law, utilising the terms ‘Medical AND treatment’ AND ‘informed consent’, yielded 446 cases. Careful reading and selection of cases that addressed consent or risk disclosure as a main topic left 27 cases for further scrutiny. Cases deemed as significant (in confirming or distinguishing decisions in preceding case law) were studied in detail. Additional cases cited in relevant works by legal scholars were added to the results, together with new cases flagged by regular email alerts from legal databases and journals.
I analysed key passages of the selected medical cases using a hermeneutics approach, trying to view text as being reshaped with every new interpretation, rather than having a stable meaning (Mootz, 2016: 775–777). Through this method, I identified the gradual legal move in medicine from a physician-centred to a patient-centred standard. Although this interpretation was based primarily on the disclosure of risks required for consent to be ‘informed’, it also allowed recognition of other components deemed necessary for a valid consent.
In view of judges’ reported examination of professional codes of conduct and guidelines in medical negligence cases, not least in Montgomery v Lanarkshire Health Board (2015), I consulted the most recent versions of medical professional guidelines. Priority was given to guidance produced by medical registration and licencing bodies, for example, the General Medical Council (GMC) and the Royal College of Surgeons of England (RCSE). Naturally, the RCVS’ guidance on communication and consent provided an intriguing comparative set of professional ethical guidelines. Analysis of professional guidance revealed the gradual move from a doctor-centred to a patient-centred consent to medical treatment in professional advice to doctors (GMC, 2008; RCSE, 2016) but little evidence of a similar move in veterinary medicine. As perhaps anticipated, in view of the lack of legal guidance, the veterinary profession still relies on professional ethical guidance for its interpretation of consent.
Empirical research methods
I was interested to see whether empirical research would reveal a more client-centred approach to consent existing in the ‘real world’ of the veterinary clinic, despite contrasting evidence in the RCVS guidance. In designing a ‘mixed methods’, rather than a ‘mixed methodologies’ study, I utilised a single methodology (interpretive description) but multiple methods to collect data, that is, submission of consent forms, participant observation and interviews. Documentary analysis of forms, transcripts of observed consent discussions and transcripts of interviews with key stakeholders provided empirical data. Analysis of each data source informed the others to produce the multiple perspectives required, with triangulation in this case intended to broaden the understanding of the topic, rather than to increase the validity of the data (Ritchie and Ormston, 2014).
Prior to empirical data collection, application for ethics approval was submitted to the University of Birmingham Humanities and Social Sciences Ethical Review Committee. Initial approval was granted for collection of consent forms and observation of consultations in February 2016 (reference number: ERN_16-0077), with additional approval for interviews in September 2016 (reference number: ERN_16-1138).
The first study analysed the language used on consent forms, to clarify their role in the consent process. Collection of blank consent forms avoided any data protection issues that would have arisen if client details were included. I was careful to outline the conditions for consent for those submitting the forms, that is, that they would be anonymised and that they would be analysed by me as the researcher, with portions of text used to exemplify themes in my doctoral thesis and in any subsequent publications. Following multiple posts on social media sites and email requests to targeted practices (comprising large corporate group practices and charity hospitals) 60 forms were submitted. Of these, 41 were included in the final analysis after exclusion of duplicates, forms for other procedures, and those originating from outside the United Kingdom and Ireland. The forms were anonymised by removing practice details before being thematically analysed.
The second study involved direct observation of consent discussions, investigating the communication of consent in terms of the requirements for a valid consent. As a procedure that is performed almost daily in most veterinary practices in the United Kingdom, elective (non-therapeutic) neutering of companion animals (cats, dogs and rabbits) provided a case study with frequent opportunities for observation. In addition, it ensured there was partial standardisation of the information that should be provided as part of the consent discussion. Initial attempts at practice recruitment were unsuccessful, with personal visits and revisits to several local practices resulting in failure to recruit a single participant. A serendipitous meeting with the director of a large veterinary practice facilitated the recruitment of a ‘case study’ setting. Following my attendance at a practice meeting, where I explained the research, answered questions and responded to concerns, the practice team agreed to participate. Study information sheets were left at the practice for individuals to read and consider. Consent was obtained in writing from all veterinary surgeons involved, prior to each consultation. This included consent for recording of the consultations and the use of quotes in my thesis and any subsequent publications. The approach I took to obtaining consent from clients was slightly different. Receptionists asked those clients arriving for pre-neutering appointments if they would agree to discuss the study with me while they were waiting. I then spoke to all clients who had agreed to this, explaining the study and going through the consent form with them. I obtained written consent from all clients involved prior to the consultation. Data were collected using ethnography-derived participant observation. The criteria for these observations were that the consultations had to involve the owner(s) of an animal being presented for a pre-neutering examination and consent discussion, and the veterinary surgeon who would undertake the consultation. I was present as an observer, although not participating in the consultation. This allowed me to note any physical tasks that took place or explain any silences on the recordings. Ten consent discussions, involving a total of eight veterinary surgeons with experience ranging from 2 to 12 years, were observed. Each consultation involved one or two clients and was recorded on a digital voice recorder, placed in a suitable position in the room. Transcription was performed as soon as possible after observation, to enable the noting of any tasks (such as clinical examination or weighing the animal patient) that took place during key moments in the discussion, and to allow concurrent data analysis to evaluate saturation. There were no apparent differences in the conversations conducted by the veterinary surgeons, despite them having varying experience. All covered similar topics, and their consultations were of a similar length.
The third empirical study involved interviews with 10 ‘purposively sampled’ key stakeholders, selected for their knowledge and for the ease of establishing contact, either due to location, connection or time available. Six interviews took place on-line, while four were conducted face-to-face. The interviewees comprised three veterinary surgeons, two of whom worked with small animals and one with farm animals, all with at least 10 years’ experience in practice, two veterinary nurses, both with at least 10 years’ experience in practice, two representatives (one veterinary surgeon and one lawyer) of professional organisations and three animal owners, two experienced (had owned animals for at least 10 years) and one new (had just acquired first pet). These participants either had recent experience of obtaining or giving informed consent, or they provided normative guidance to practitioners, thus fitting with a symbolic interactionist approach to participant selection. All participants were sent information sheets about the study and consent forms in advance of the interviews and gave written (face-to-face interviews) or verbal (recorded as part of the on-line video interviews) consent prior to the interview itself.
For recruitment of veterinary professionals, I relied on personal contacts and veterinary organisations, while for animal owners, recruitment took place via social media forums and a research recruitment website (Call for Participants, 2016). Active interviews (Holstein and Gubrium, 1995) were conducted with each participant, thus allowing respondents to switch positions or take on new roles and perspectives when prompted by interview questions (Hoffmann, 2007). Three interviewees (two veterinary nurses and one veterinary surgeon) switched positions during the interviews; for example, a veterinary nurse switched roles to relate experiences of decision-making as an animal owner. Importantly, by regarding my own background knowledge as a resource that could link the research interests to participants’ experiences, active interviewing allowed ‘simultaneous coding and construction of knowledge’ (Holstein and Gubrium, 1995: 57) to take place during the interview.
Data analysis and triangulation
Analysis of the doctrinal legal research was completed prior to collection of data from empirical studies. Analysis of the empirical data was based on a ‘grounded theory’ approach (Glaser and Strauss, 2017). While interpretive description does not adhere to grounded theory’s rigid format for data analysis, instead requiring broad-based coding and experimentation with perspectives (Thorne, 2016: 161), it often utilises thematic analysis to identify and describe ‘implicit and explicit ideas’. (Guest et al., 2012: 10).
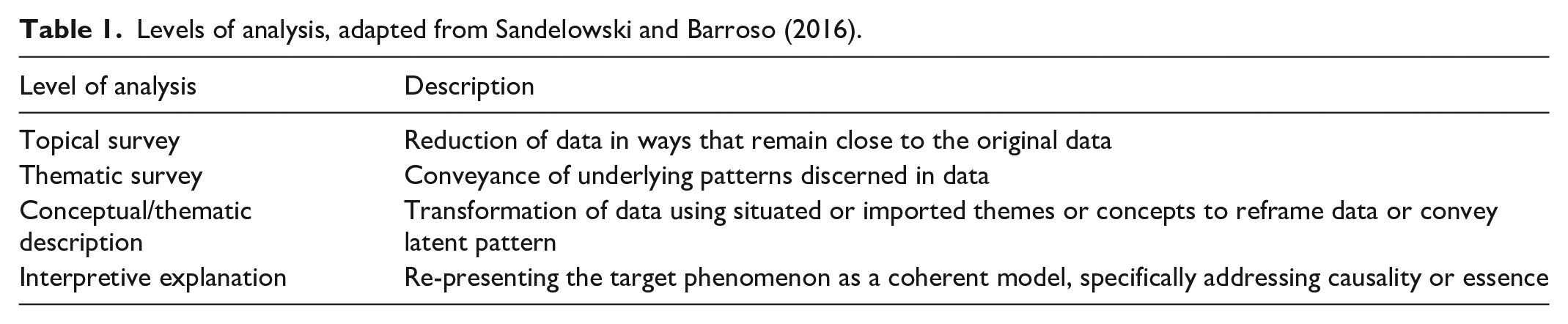
Transformation of the data required asking increasingly complex questions about their meaning. Useable findings require a level of analysis beyond mere description, thus moving the analysis further from the original data (Sandelowski and Barroso, 2016 – Table 1). Broad-based coding usually results in analysis that sits somewhere between ‘thematic survey’ and ‘conceptual or thematic description’, depending on the degree of transformation and abstraction of the data patterns.
Levels of analysis, adapted from Sandelowski and Barroso (2016).
Consent form data analysis
Although I was aiming for conceptual description in each analysis, I found that the consent forms presented the most difficult challenge. The variation in language used on the forms required interpretation and judgement on how best to categorise sections of text. Initial coding used a constant comparative method to check the validity of any themes that arose from the data. Inevitably, as the level of analysis increased, perspectives from doctrinal research crept in, for example, themes involving respect for client autonomy (the ‘patient-centred’ approach found in my legal analysis) or the use of paternalistic language (the ‘doctor-centred’ approach) (Table 2). The term ‘paternalistic’ was used for initial coding and analysis, but I realised that the notion of ignoring the patient’s autonomy is inappropriate in this context, as the veterinary patient does not have autonomy. When abstracting the findings to the level of conceptual analysis, I therefore substituted the term ‘beneficence’ (trying to act in the best interests of the patient) for ‘paternalism’’.
Levels of analysis for consent forms.
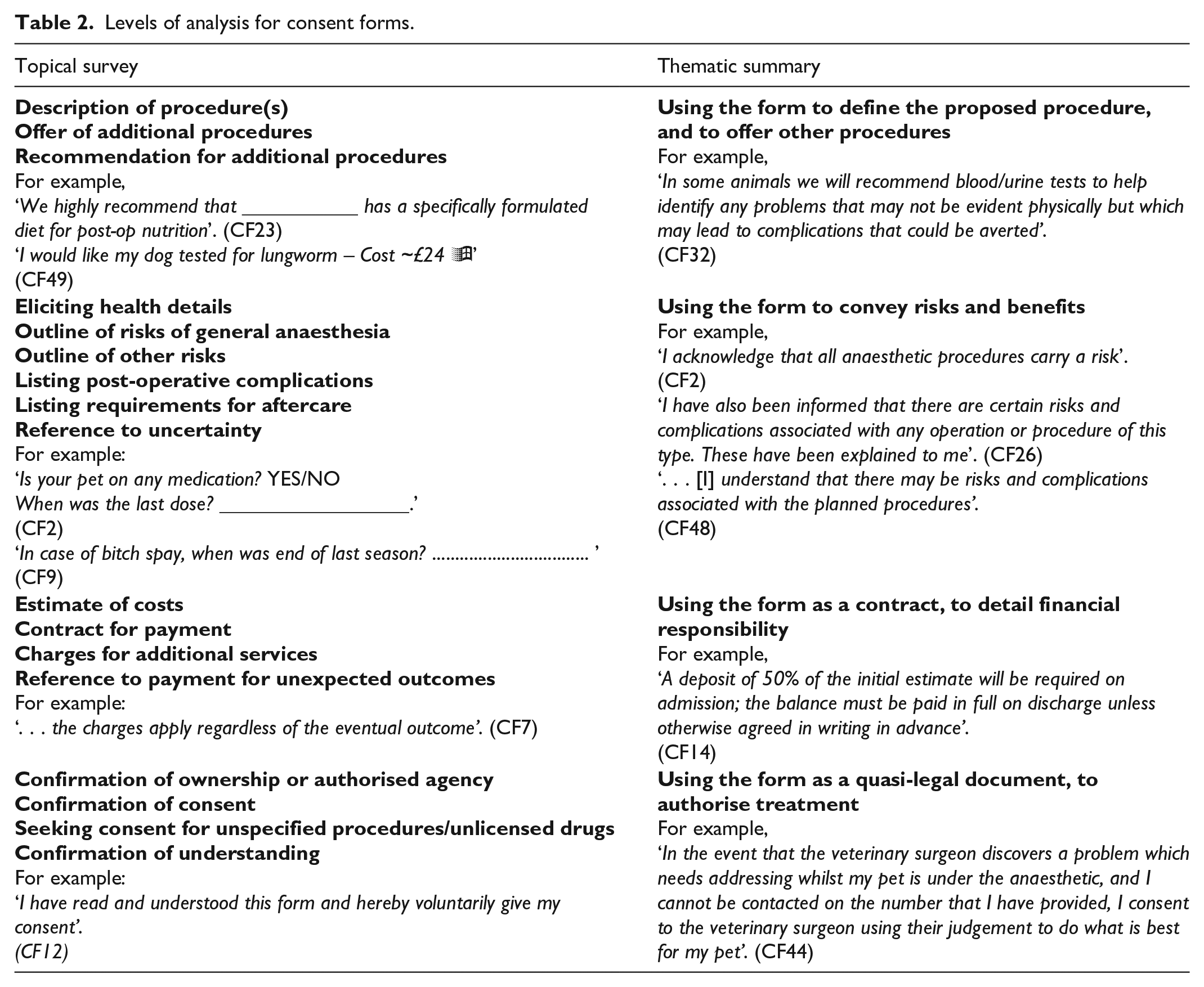
The conceptual description for consent form analysis comprised the constructs of respecting client autonomy vs demonstrating beneficence; deciding about level of risk disclosure; respecting client financial autonomy and defining the role of the consent form in the process of obtaining informed consent.
Observational study data analysis
Transcribing the recorded observations of consent discussions enabled me to define and re-define themes, using open coding (Charmaz and Bryant, 2016) for initial analysis. Resulting themes were synthesised into a thematic summary, informed by categories emanating from doctrinal research and from the prior analysis of consent forms (Table 3).
Levels of analysis for observed consent discussions.
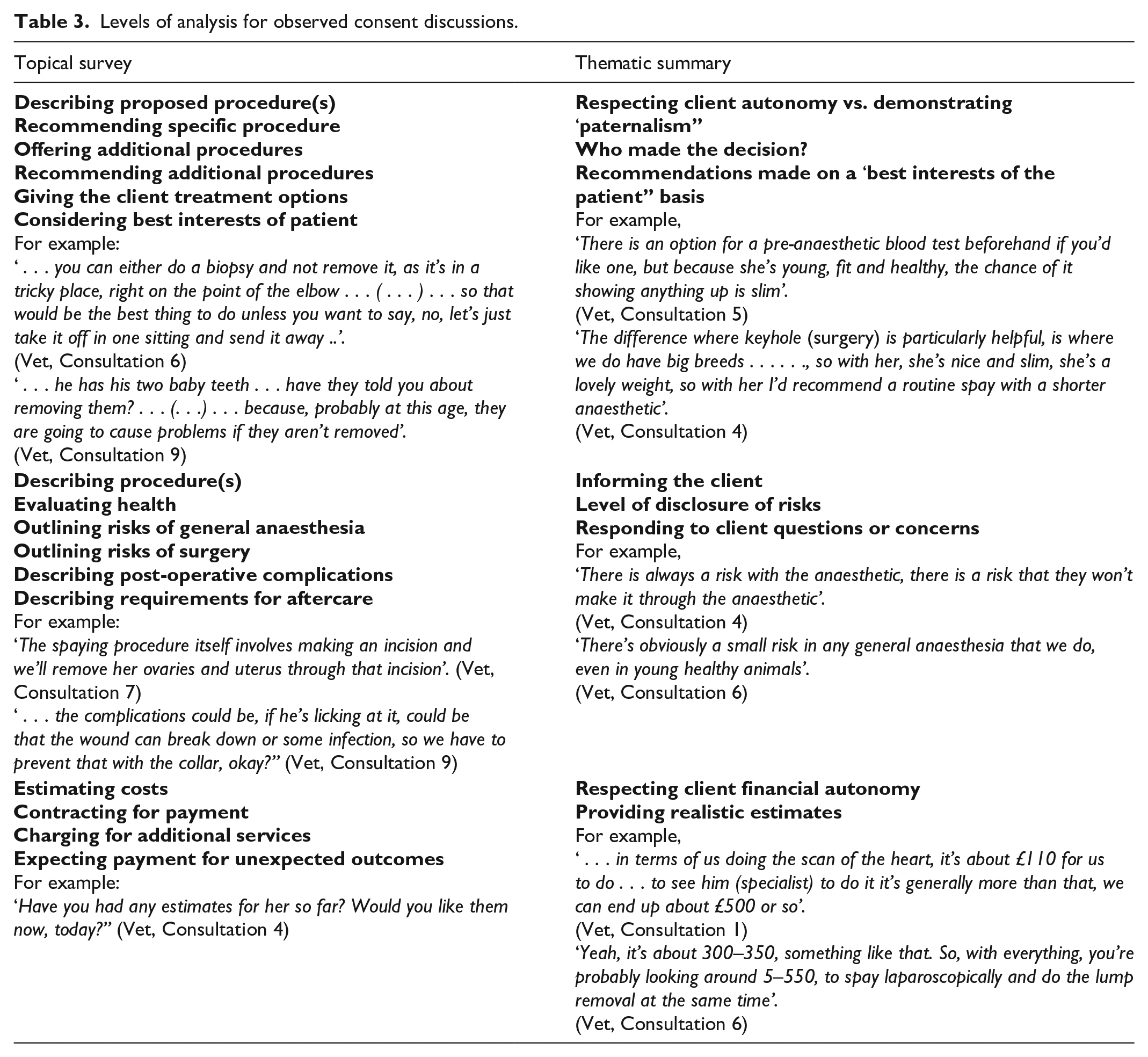
A more abstract interpretation of these observational data produced a final analysis at the level of conceptual description, revealing three predominant constructs: autonomy vs beneficence as consent’s underpinning principle(s), the degree of respect shown for client autonomy and recognition of constraints on client autonomy.
These constructs showed several similarities with those derived from the consent form data analysis, with respect for client autonomy and demonstration of beneficence emerging as key themes.
Interview data analysis
Interview data were transcribed and anonymised as soon as practicable after collection. There seemed to be no difference between online and face-to-face interview data regarding response to interview questions. Open coding allowed the inductive development of categories, incorporating novel topics presented by the interviewees. Although the initial round of coding was performed on a software programme that I used for data management for all studies (QSR NVivo), a second round of coding utilised hard copies of the transcripts and coloured highlighting pens. The two coding rounds were compared and combined, ensuring that coding was comprehensive and consistent (Table 4).
Levels of analysis for interviews.
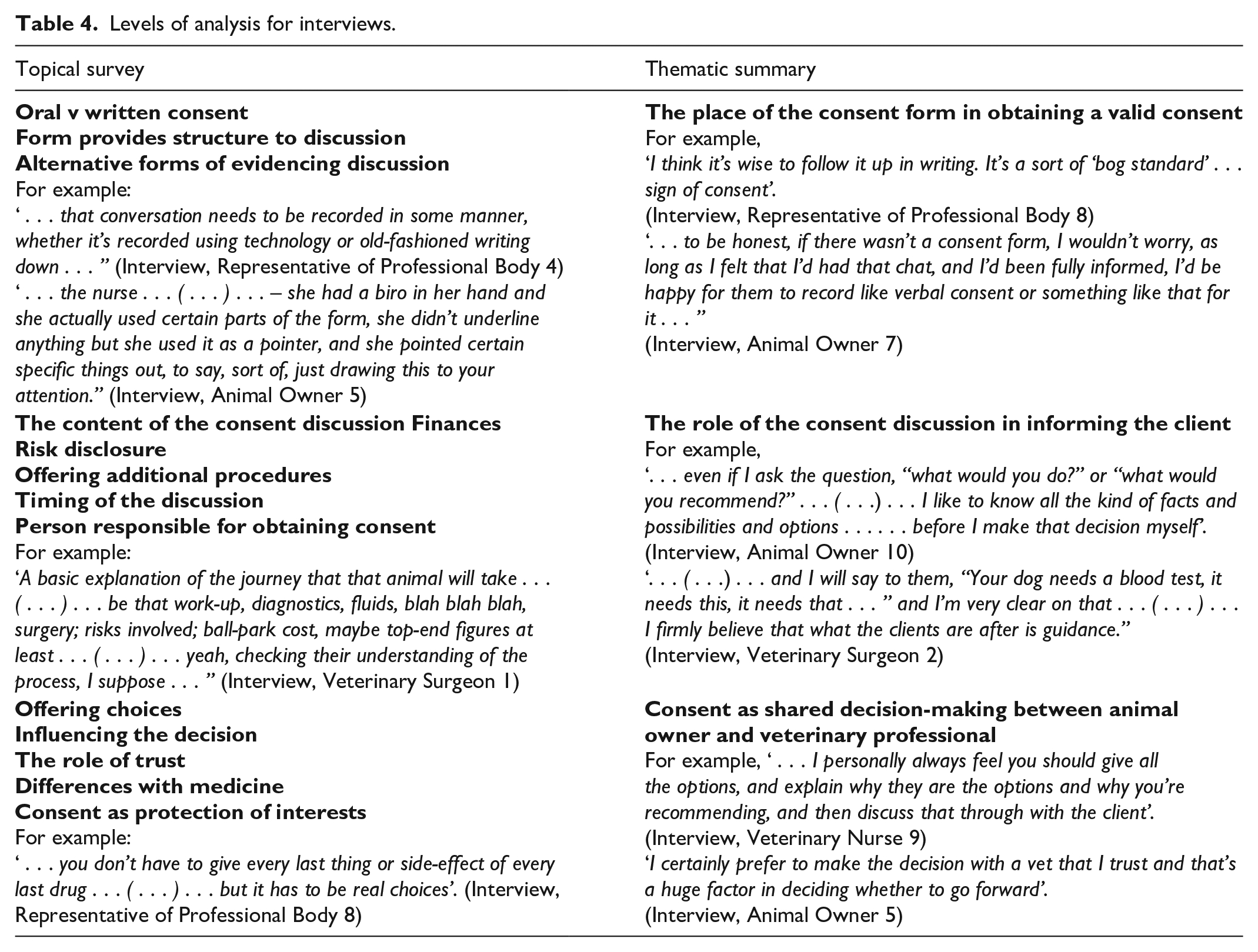
Working on the premise that interpretive description should be ‘located within . . . existing knowledge’ (Thorne et al., 1997: 173), interview data were further analysed using a critical analytical framework suggested by the preceding studies (Morse, 2004). A hermeneutics approach allowed a clear indication of what was located in the original text, working directly from the interview transcripts, and what was my interpretation of its meaning (Austgard, 2012). A fusing of horizons (mine as researcher, and those of the participants) allowed interpretation of the new knowledge within the framework of existing knowledge, from my prior experience, from doctrinal legal research and from the preceding analyses.
Conceptual description for interview data comprised the key constructs of how a balance is achieved between client autonomy and beneficence; the role of the form as protection for the veterinary professional, but also extending to protection for the client and, consequently, for the animal patient, and how the consent process can demonstrate respect for (constrained) client autonomy, through full disclosure of information including the risks involved with the proposed procedure.
The higher levels of analysis for interview data were clearly influenced by the results of earlier analyses, but with considerable input from my values, beliefs and experience. I reflected on how my background may have influenced data analysis, and how this was explicitly portrayed (Braun and Clarke, 2013). The foregrounding and appropriation of my own ‘fore-meanings and prejudices’ (Gadamer, 1989: 269–270) involved consideration of how my prejudices may have affected data collection and analyses. As my previous experience as a veterinary surgeon was documented on the participant information sheet for each study, it may have moderated participants’ responses to interview questions or their behaviour during consultations. All the ‘case study’ practice’s clients that were approached agreed to participate after talking to me, which raised important questions about the voluntariness of their consent. I made clear to these participants that I was not employed at the practice, therefore would have no input to their animals’ care. Nevertheless, evidence from medicine suggests that potential participants in clinical research are more likely to agree to take part when asked by a physician, demonstrating the effects of trust and power on consent (Nelson and Merz, 2002). Interestingly, this was later reinforced by an interviewee, who commented,
If a vet that I had great trust in, and that I had always seen acting in my pet’s best interests before, I couldn’t fail to consider what they would recommend. (Interview, Animal Owner 5)
In this area, the focus of my research (informed consent) and the methodology used to collect and interpret data seemed to converge. I put a great deal of thought into consent processes for my data collection, but the potential for my background as a veterinary surgeon to influence potential participants was one that I had not foreseen. Nevertheless, I am reasonably satisfied that those who participated did so voluntarily (by responding to an advertisement on social media, or in the case study practice, by agreeing to be approached before knowing that I was a veterinary surgeon).
Conceptual description of consent
My construction of consent in the veterinary context depended on a multifaceted approach to data collection, the application of hermeneutical analysis to judicial decisions and interview transcripts, and a grounded theory-based thematic analysis of data from consent forms and observed consultations. Bringing these together depended on the ability to think at a more abstract level. Doctrinal analysis clarified the legal basis of consent which, in combination with its professional ethical basis, influenced the conceptual analysis of the findings from empirical studies. The higher levels of analysis depended on the incorporation of prior analyses and my prior experience, knowledge and beliefs, justified through a hermeneutical perspective on the ‘fore-structure of meaning’ (Mootz, 1988: 534–535).
In summarising my conclusions, consent forms were rarely used to fully document the accompanying discussion, and evidence that they were used to support client autonomy was equivocal. The importance of respecting client autonomy was derived from analysis of the observed consent discussions, which highlighted that demonstrating respect for client autonomy included recognising the client’s financial autonomy.
Regarding the purpose of consent, the views of interview participants concurred with previous medical and veterinary research in holding that its primary purpose is to ‘protect’ the professionals involved (Akkad et al., 2006; Whiting et al., 2017). Participants suggested that consent conversations should include disclosure of specific risks, although there were strikingly differing opinions regarding how much respect should be given to client autonomy. The identification of trust as a potential influence on consent parallels my reflection on recruitment of clients for the observational study.
The synthesised conceptual description led to normative proposals for improved consent protocols in practice (Gray, 2019), both for the design of consent forms to allow more comprehensive recording of the accompanying discussion, and for the content of the discussion to include specific disclosure of risks, alternative treatment options, and financial obligations for treatment and aftercare. On reflection, the use of interpretive description facilitated the production of recommendations for practice, some of which were incorporated in the RCVS’s updated guidance on consent (RCVS, 2020b).
Limitations of the studies
Findings from this work are confined to a very small section of the veterinary medical world. Time constraints forced me to concentrate on one practice setting. I chose small animal practice (treating mainly cats and dogs) because it was the setting with which I was most familiar, the patient in this setting has a ‘privileged’ position, and it is the most common type of veterinary practice in the UK (RCVS, 2017). However, the selection of small animal practice did not make recruitment any easier, either for submission of forms, for conducting observations or for enlisting key participants. Due to problems recruiting veterinary surgeons for interview, I included one farm animal veterinary surgeon in the final analysis of interview data, even though this interview was intended as a pilot. This participant’s responses did not, however, differ from those of other veterinary surgeon participants. By choosing the routine, commonly performed procedure of neutering for the case study, I limited the analysis to consent obtained in a low-pressure and unhurried environment. Further research is needed to explore the way that consent is obtained in emergency situations, and how the decision-making of both the veterinary surgeon and client may differ in such circumstances.
The selected methodology of interpretive description took the research down a very applied path, with constant references to how the consent process could be changed in practice. In doing this, it may have missed some of the more philosophical aspects of consent, such as what it means to an owner to agree to medical treatment on behalf of the animal, and the approach of the veterinary professional, as either paediatrician or garage mechanic (Rollin, 2006). The methods used were selected to reflect the interdisciplinary nature of socio-legal studies, while facilitating the thematic analysis that underpins interpretive descriptive methodology and providing multiple sources of information to fulfil the requirements of case study design (Hyett et al., 2014). The integration of doctrinal legal research with three separate but triangulated empirical studies presented me with several challenges, not least the weighting afforded to the legal, ethical and empirical aspects of consent. The space devoted to each of these topics was determined by its practical application to consent in practice. These challenges would apply to similar research studies conducted in practical settings, while invoking legal and ethical normative guidance. Finally, the time available for each study was a constraint on what could be achieved. Larger numbers of participants and a wider selection of practices may have produced different findings, but I have tried to ensure the ‘ecological validity’ (Braun and Clarke, 2013: 280) of my findings by obtaining data from real world contexts and through triangulation of three types of empirical data collection and analysis.
Conclusion
The study found that consent in veterinary practice for routine surgery is recognised as a required step to authorise treatment, but there was little evidence of the client being fully informed about options, risks and benefits. Veterinary professionals seemed reluctant to give clients the full range of options, despite clients welcoming more information to enable them to make decisions. Consent was often obtained as a means of ‘protection’ for the veterinary professional, but it was not often ‘informed’, therefore its protection of the client and animal patient was debatable.
The article explains my philosophical approach to this study of consent in the veterinary clinic, introducing interpretive description as a potential methodology of health-related socio-legal studies. The selection of this methodology enabled a research design that utilised the most appropriate methods for data collection in each of the empirical studies, and the explicit use of knowledge gained from previous analyses to inform the next.
Evaluation of the methodology refers to its usefulness in research that involves applied and highly context-specific settings and its incorporation of several foundational social science methodologies. I have demonstrated how the triangulation of data collection methods enhanced the understanding of the consent process through providing several different perspectives, and through explication of the levels of analysis achieved for each piece of empirical work.
Footnotes
Acknowledgements
The author is indebted to the veterinary practices that submitted copies of their consent forms, and to all participants who agreed to take part in observations and interviews. The author also thanks the UK ESRC for their support of her doctoral studentship and postdoctoral fellowship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author’s doctoral studentship was supported by the UK Economic and Social Research Council (grant number 1615019), and the same organisation supports the author’s postdoctoral fellowship (grant number ES/T009136/1).
Data access
Data are available from the author on reasonable request