
Abstract
Introduction:

Current guidelines suggest a multimodal approach to treating scars but there is no gold standard for treatment; however, there is exciting therapeutic potential for the use of autologous fat grafting (AFG). Functional and aesthetic improvements have been reported, including pain relief and scar quality improvement.
Aims:
To explore the current evidence regarding the use of AFG in hypertrophic and painful scars.
Methods:
A systematic review of the literature was conducted using 11 MeSH terms in PubMed, Medline and EMBASE. English studies that used AFG to treat scars in human participants were included.
Results:

A total of 746 studies were found and 23 studies (from 2008 to 2016) were included: five studies were evidence level V; nine studies were evidence level IV; eight were evidence level III; and one study was evidence level II. A total of 1158 patients were assessed for improvement in scar characteristics including colour, thickness, volume, pain and restoration of function at affected sites, following treatment. Positive outcomes were noted for all parameters and a significant improvement in AFG’s analgesic effect was recorded in 567 out of 966 patients, P < 0.05.
Discussion:

AFG is a minimally invasive and safe approach to treating scars, a promising alternative to surgical excision. The technique of blunt cannula insertion optimises the release of scar retraction, which contributes to the analgesic effect of this treatment method. The evidence supports current theories of mesenchymal stem cell’s regenerative and anti-inflammatory properties responsible for scar healing. There are limited high quality studies to support its use and future randomised controlled trials should be conducted.
Lay Summary
Currently there is no gold standard treatment for scars, however there is exciting potential for the use of autologous fat grafting (AFG). This technique uses liposuction to extract fat from areas of the body where it is readily available. It is then processed to remove all debris and injected under a scar. We carried out a study to review its use in clinical practice.
Results of the literature suggest fat contains specialised stem cells that possess properties which improve the quality of scars. Fat injection has been shown to decrease tension which softens scar tissue and provides pain relief. Analgesic effects are caused by nerve repair and scar entrapment release. As well as functional benefits, the evidence also shows fat grafting improves the cosmetic appearance of a scar. In conclusion, AFG is a safe treatment method with few complications. This method poses promising benefits in future treatment of scar-related conditions.
Introduction
There is currently no gold standard treatment for scars; however, there is promising therapeutic potential for autologous fat grafting (AFG), a treatment pioneered by numerous institutions.1,2 The key aims of scar revision are to camouflage the tissue to the surrounding skin and restore functional capacity at the site. 3 Neuropathic pain may also be experienced in scars, caused by the entrapment of nerve fibres in scar tissue. AFG harnesses the regenerative properties of adipose derived stem cells (ADSC) to restore function, improve appearance and provide analgesia. 4
Current guidelines for scar treatment support a multi-modal approach, with the best results following combination therapy of laser treatment, 5-fluoracil and corticosteroids for hypertrophic and keloid scars. Newer therapies include mitomycin c and onion extract, which are currently growing in interest alongside AFG.1,2
AFG has had an expanding role in plastic surgery due to its filling effects and regenerative properties. 5 Historically it was used to treat wounds with tissue loss and congenital deformities. 6 However, the introduction of liposuction increased its availability and its clinical applications to treat facial lipoatrophy, breast surgery and buttock augmentation.7–9 Coleman (1995) further evolved its application when he described a reproducible technique of injecting lipoaspirates. 10 This increased the survival of harvested fat, which is now an established method of administering autologous grafts.
Rigotti et al. (2007) first described the regenerative capacity of ADSC to treat chronic oncological lesions after radiation therapy. 7 They reported an improvement of lesions that had previously been irreversible, with hydration and neo-angiogenesis. Following this, Klinger et al. (2008) documented the first use of AFG in treating scars. 11 This case series included three patients with burns of the face, hands, trunk and limbs, who were treated with two sessions of AFG and followed up after six months. A positive outcome was reported with increased softness and, improved texture and thickness of scar tissue. Histological staining also demonstrated tissue architectural remodelling, supporting Riggoti et al.’s theory of ADSC’s regenerative potential.7,11
Aims
The aim of this study was to carry out a detailed search of the current literature assessing the efficacy of AFG in treating scars and analgesia. In doing so, we aim to test the hypothesis of the regenerative capabilities of adipose tissue and develop further evidence of the role of ADSC in scar healing and analgesia. The evidence can be used to guide future treatments and construct further research in this area.
Methods
A systematic literature search was carried out by two independent authors using the PubMed, EMBASE and Medline databases. 11 MeSH terms were used to conduct the search, based on keywords used in literature on AFG treatment of scars (Table 1).12,13 Variations of the terms were included to ensure inclusion of all relevant articles, e.g. ‘fat graft’ could be substituted with ‘adipose graft’ or ‘lipofilling’. All possible combinations of terms were entered in the databases. Filters were applied, in accordance with pre-determined inclusion criteria (Table 2). Studies using human participants, written in the English language and fully accessible via PubMed, EMBASE and Medline, were included.
MeSH terms used in literature search.

Inclusion criteria to filter articles.

Articles returned from the search were screened using titles and abstracts. Eligibility was assessed independently by two authors. Studies that reported the outcomes of AFG as an intervention for scar healing and analgesia were included. The search was not restricted to any one scar type and included studies that used AFG with or without supplementary treatments. References of articles included in the search were reviewed to assess if further studies could be included (Figure 1). Full texts of the articles were read to further determine compliance with inclusion criteria and aims of this review. All articles returned from the search were categorised into levels of evidence based on the Oxford Centre of Evidence-Based Medicine (OCEBM) levels of evidence (Table 3). 14 No formal statistical analysis was carried out due to the heterogeneity of outcome measures and quantitative data in the studies included.
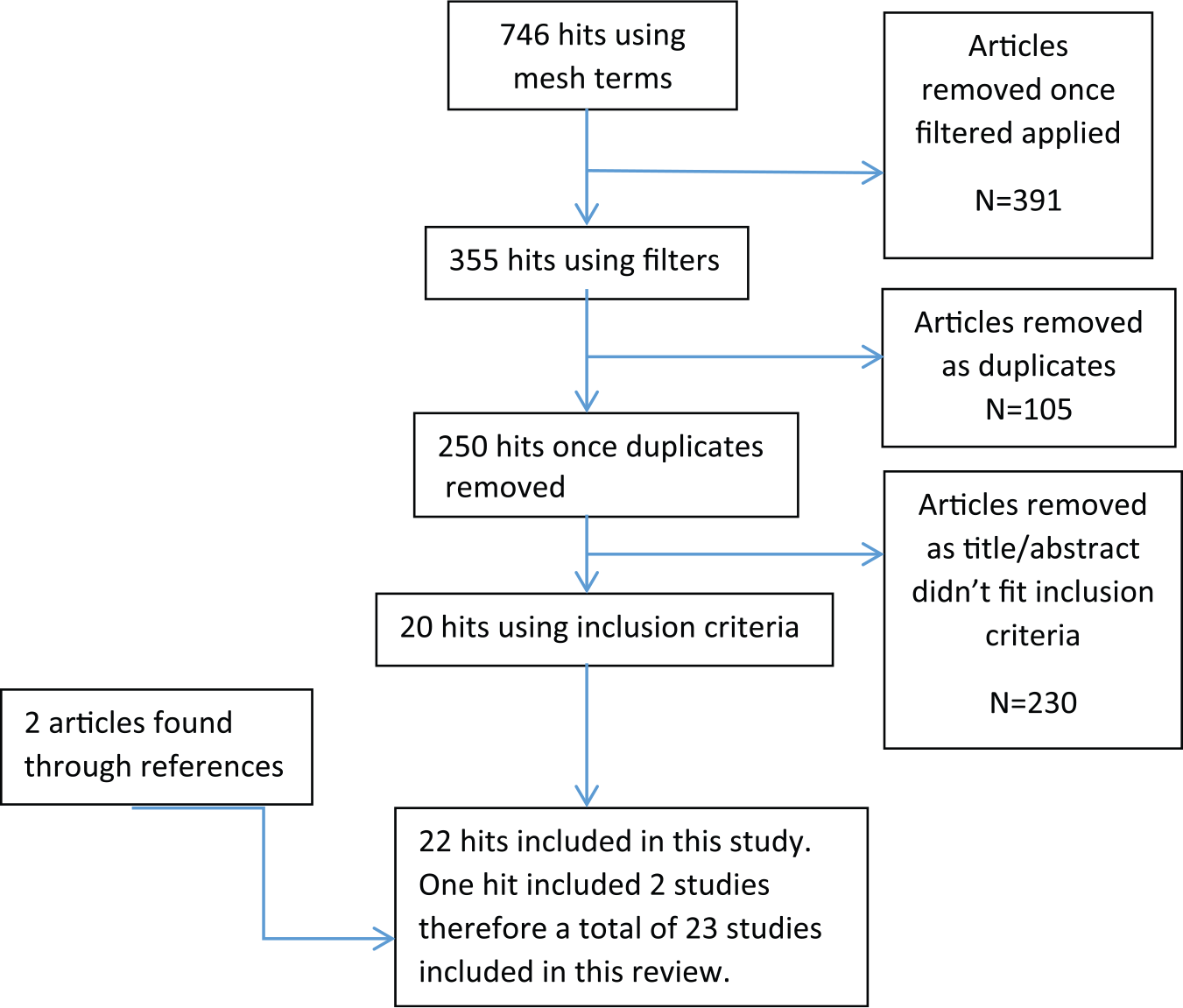
Diagram showing method used to determine articles included in this review.
Levels of evidence per OCEBM.

Results
All 23 studies adopted liposuction to harvest autologous fat grafts. 15 studies processed AFG according to Coleman’s technique involving 1062 patients.3,5,17–21,24–29,31 Additional methods included simple filtration and Telfa rolling.23,33 Most commonly the aspirate was centrifuged at 3000 rpm for 3–5 min. Aspirate was injected under scar tissue at the dermal-hypodermal junction and a technique of retrograde fat deposition was used, allowing fat distribution in multiple planes, dispersed in a web-like matrix. Eight studies reported that fat distribution was matched in importance by the scar release induced through needle insertion at the site.3,5,11,19,21,26,27,30 This technique achieved reduced skin contracture and increased tissue viability.
Donor sites included the abdomen, medial thigh, hips and trochanteric regions. The abdomen was used as a donor site in 16 studies and was the only site in 11 studies, in 340 patients.3,5,11,15,17–22,26–28,30,31 This donor site is preferable due to the abundance of fat and ease of access with the patient supine.
The number of sessions varied among studies, with 13 studies using one session of AFG treatment.3,5,18,20–24,28,29,31,33 Ten articles report using more than one session in some or all participants.10,15–17,19,25–27,30 Mazzola et al. (2013) states that volume filling is the first step and further scar quality is achieved through a second session. 30 Studies were guided by further treatment based on contour and volume filling or by outcome improvement, e.g. pain, itch and restoration of function. Average follow-up was 11.4 months (range 3–60 months). Long-term follow-up mostly occurred up until 12 months and loss to follow-up was only reported by Caviggioli et al. (2011). 21
All 23 articles assessed cosmetic changes post treatment, e.g. colour, scar appearance in relation to surrounding skin and thickness. 12 articles studied pain relief; six articles used the Patient and Observer Scar Assessment Scale (POSAS), which included assessment of relief of pain and itch alongside pliability, vascularisation and scar surface area;3,5,19,21,24,27–32 two articles used histological outcomes to assess microscopic changes at the cellular level; and six articles assessed functionality at the site of the scar post treatment.10,17–20,23,25,27 Outcome measures were heterogeneous, involving both quantitative and qualitative data.
Volume injected
Volume of fat injected was in the range of 0.5–80 mL, reported in 15 articles.3,5,15,20–23,25–28,30,32,33 Guerrissi et al. (2015) reported the largest volume injection of 80 mL in a 21-year-old man with circumferential burns of the right leg. 25 The volume injected was proportional to the extent of scarring and surface area affected. Klinger et al. (2013) suggests that 1 mL AFG for each 3.5cm2 should be used and Piccolo et al. (2015) suggested 1.6–2.0 mL per 10 cm2.5,34 No other studies reported a volume : scar size method for calculating injected AFG volume. The degree of scar retraction more commonly guided volume of fat injected.
Pain and itch
The analgesic effect of AFG was assessed in 966 patients.3,5,19,21,24,27–32 In total, 832 patients had an improvement in pain following treatment; of these, 567 showed a significant improvement. This was measured using POSAS, visual analogue scale (VAS), the neuropathic pain symptom inventory (NPSI), Manchester scar scale (MSS), present pain intensity index and the McGill pain questionnaire. Caviggioli et al. (2011) used AFG to treat post-mastectomy pain and 28 out of 34 patients withheld analgesia following lipofilling. 21 Furthermore, pain reduction post AFG was significant, P < 0.05 in the treatment group compared with controls. AFG’s analgesic effects were reported for facial scars, perineal post-surgical scars, burns and vaginal lacerations. Pain relief was reported as early as 14 days’ follow-up.
POSAS outcomes were assessed for 126 patients in six studies; however, data were available for 95 patients only. An improvement in patient and observer outcomes for scar colour, regularity and thickness were reported. A total of 82 patients reported a significant improvement in pain and itch following treatment.5,19,24,28,29,31
Restored function
Five articles aimed to restore function at the site of the scar tissue in 713 patients, summarised in Table 4.5,19,20,25,27 Functional deficits included limited facial movements with facial burns and reduced mobility of joints due to scar retraction. AFG restored functional capacity in these patients. Guerrissi et al. (2015) demonstrated this with restoration of leg extension after treatment of retracted scars following burn injury. 25
Studies assessing the effect of AFG on functionality.

Scar appearance and tissue hardness
All 23 articles commented on the scar appearance and cosmetic restoration post AFG treatment. Positive outcomes were reported in all studies regarding appearance of scars, including erythema, contouring, elasticity, thickness, texture, softness and colour. Significant results were reported in four articles. Klinger et al. (2013) reports improvement in all POSAS parameters, both patient and observer after three months of follow-up. 5 All these parameters were significant compared to controls except pain and itch (Tables 5 and 6).
Summary of effect of supplementary additions on scar tissue.
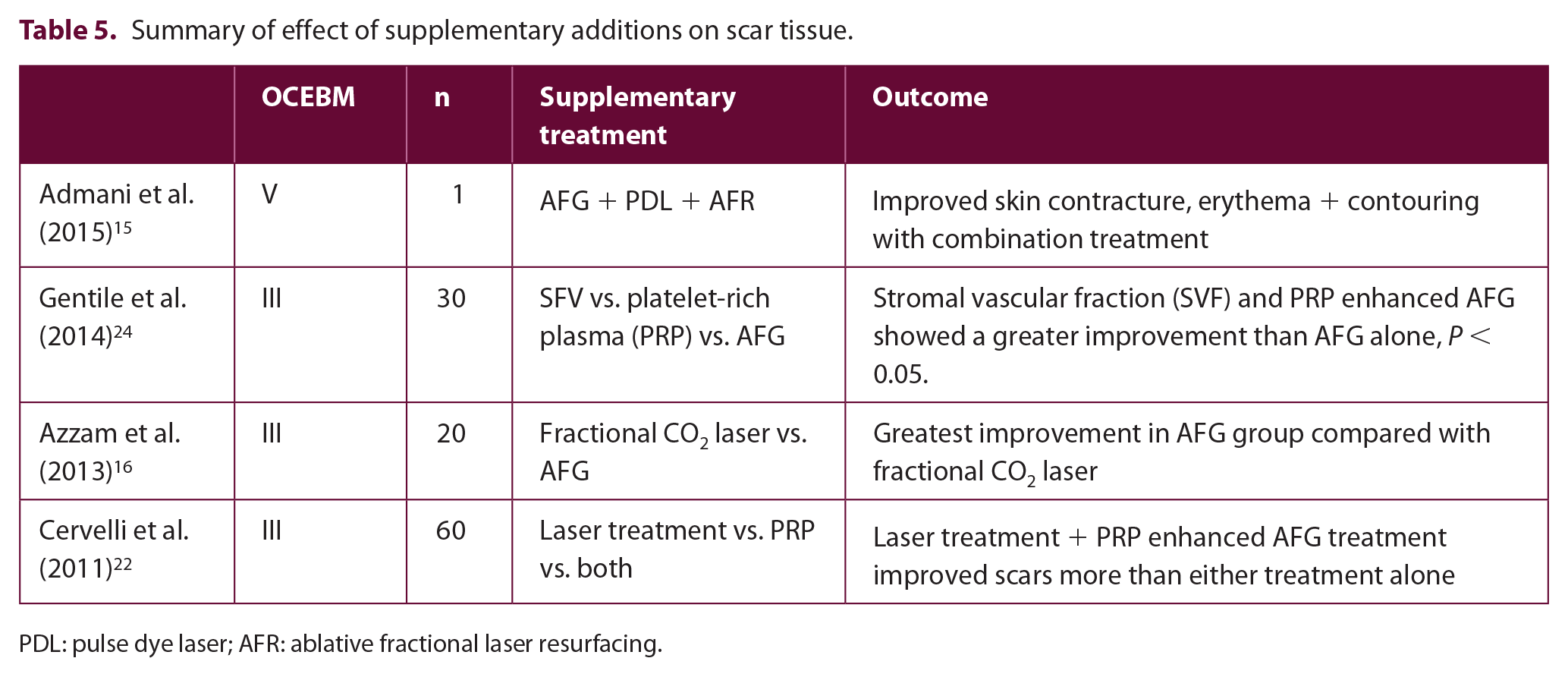
PDL: pulse dye laser; AFR: ablative fractional laser resurfacing.
Summary of scar features using POSAS.

No improvement post AFG treatment.
Significant improvement post AFG treatment (P < 0.05).
Improvement post AFG treatment.
NA, information not available.
Durometer measurements were used to report tissue hardness. Maione et al. 29 and Klinger et al. 5 both report a significant reduction in durometer measurements, three months after AFG treatment in 56 patients, compared with preoperative scores (Table 7).
Summary of articles included in this review.

Volume and contour definition
Nine articles studied the volume and contour definition of scars following AFG treatment in 794 patients.5,17,23–25,28,30,33 Scar depression is a feature reported for many cases; AFG produces a volume filling effect post treatment. Klinger et al. (2013) reported an improvement in all 694 patients following AFG treatment. 5 No significant difference was reported. Mazzola et al. (2013) and Guerrissi et al. (2015) determined that multiple sessions were needed to achieve a complete fullness.30,25 Out of 14 patients, 12 received multiple AFG treatments. All 14 patients reported volume and contour restoration. Bollero et al. (2014) used contrast-enhanced ultrasound (CEUS) to detect post-treatment vascularisation in 28 patients. 17 Twenty-four patients reported an improvement in scar characteristics of softness, colour and contour. CEUS confirmed the presence of increased vascularisation. However, in the remaining four patients that showed no improvement in volume post treatment, no CEUS vascularisation was detected.
Histological studies
Klinger et al. (2008) and Bruno et al. (2013) both studied the changes that occur within scar tissue following AFG treatment in a total of 96 patients (Table 8).11,18 Both studies report the morphological appearance post treatment, displaying features closer to normal tissue, compared with pre-treated scars. Lipofilling induced organised collagen deposition, vascularisation and reappearance of the papillary dermis. Bruno et al. (2013) report an altered presence of antibodies, including reduced presence of P63, responsible for diffuse differentiation and proliferation in the epithelium. 18 Reduced P63 expression inhibits these processes. Alternatively, Ki67 expression increased, linked with stem cell induced cellular proliferation.
Summary of histological findings.

H&E: Hematoxylin-eosin.
Supplementary additions
Four articles, including 101 patients, assessed the use of additional treatment alongside AFG (Table 5).15,16,22,24 These include laser treatments and enhanced AFG with SVF and PRP. Admani et al. (2015) describe a combination treatment in one case including AFG, AFR and PDL. 15 A total of nine treatments were issued to address the different components of the scar. AFG treated volume contouring, AFR treated the irregularity and contracture of scar tissue, and PDL treated the erythema.
Laser treatments were used in two further studies in 80 patients, to encourage tissue tightening and remodelling.16,21 Azzam et al. (2015) determined both treatments resulted in scar improvement but the AFG treatment group had an overall higher rate of improvement compared with the fractional CO2 laser group. No significance was reported. Alternatively, Cervelli et al. (2011) determined that laser treatment, in combination with PRP-enhanced AFG, yielded the greatest improvement. The laser treated group showed a 30% improvement in 20 patients, compared with an 18% improvement in 20 patients treated with AFG. No significance was reported. 21
SVF and PRP enhancement were used in two studies, on 70 patients.21,24 SVF is abundant with ADSC and PRP encourages ADSC proliferation. This was assessed by Gentile et al. (2014), comparing SVF and PRP enhanced AFG to controls. 24 A significant difference was determined in contour maintenance compared to controls (treatment with AFG), for PRP and SVF preparations (P < 0.0001). An improvement of scar texture, contour and softness was reported.
Discussion
Injection of autologous fat grafts under scar tissue has resulted in a restoration of functionality and cosmetic appearance, rendering AFG a viable alternative for scar management (figure 2).5,7 This therapy has demonstrated an ability to reduce pain and improve scar colour, pliability, thickness and contouring, in a variety of scar-related diseases. It is hypothesised that ADSC are responsible for this phenomenon. 7 While AFG is a promising treatment for scars, there is limited evidence due to the quality of the studies, as demonstrated in this review.

Autologous fat transfer process. (Image by
Fat stores are abundant with ADSC, which can generate epithelial hyperplasia and angiogenesis. 5 Although the exact mechanism remains unclear, it is proposed that the release of growth factors is responsible for this (Figure 3). These include VEGF, PDGF, TGF-b, MMP, IGF-1, BGFG and BDNF. Growth factors stimulate endothelial cells, fibroblasts and tissue progenitor cells to remodel scar tissue.35–37 Bruno et al. (2013) and Klinger et al. (2008) demonstrated a similar mechanism with organised collagen deposition and epithelialisation following lipofilling, during histological staining.11,18 Klinger et al. (2013) demonstrated the presence of papillary dermis after AFG treatment which supports the theory of tissue architectural remodelling. 5 This hypothesis is further supported by Bollero et al. (2014) who demonstrated AFG induced vascularisation with CEUS after three months. 17 A significant association was detected between vascularisation and scar contouring and improved appearance. 17
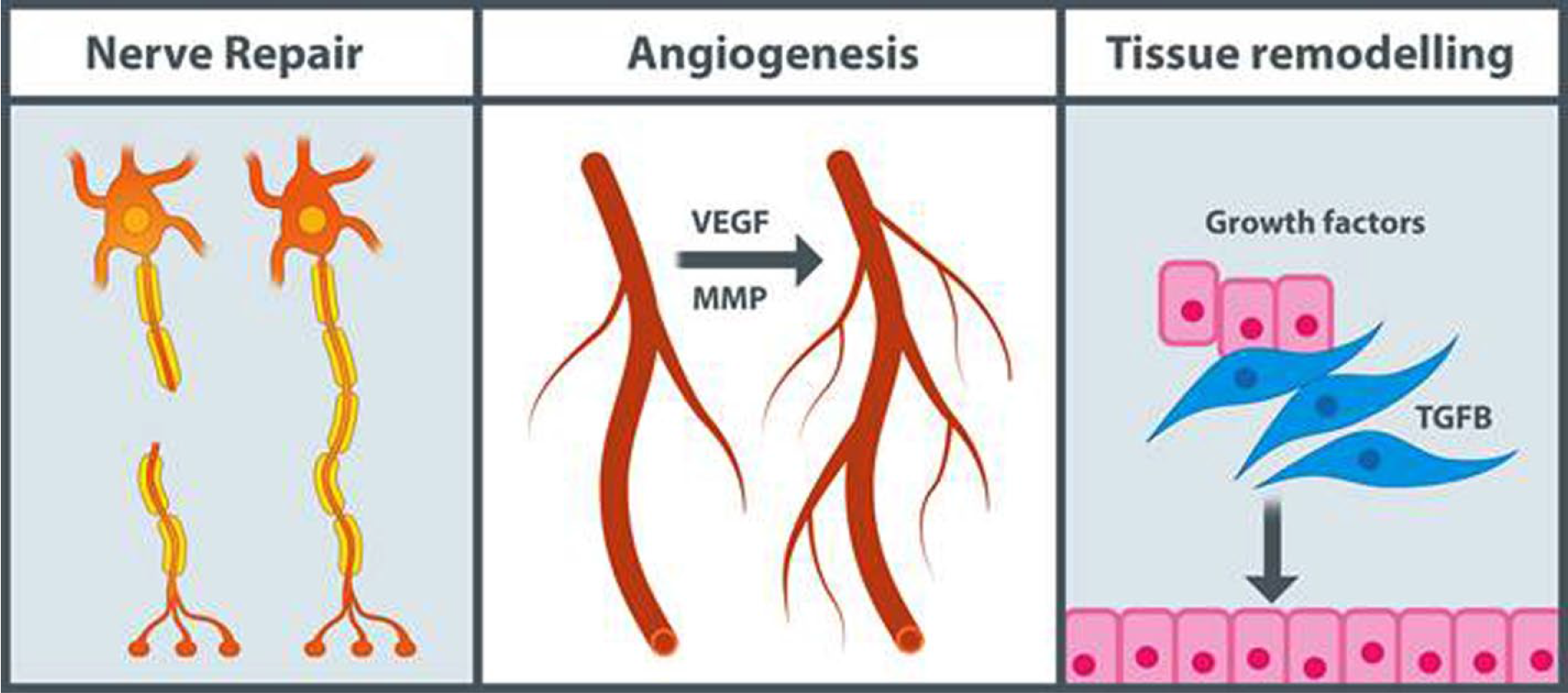
Theories of mesenchymal stem cell’s regenerative and anti-inflammatory properties responsible for scar healing. (Image
Analgesic effects are produced by nerve repair, mediated by BDNF and scar entrapment release. The injection procedure itself is responsible for making space under the scar and releasing fibrotic tissue, following needle insertion.3,4,38 Ulrich et al. (2012) demonstrated that 18 out of 20 patients had immediate relief of pain following cannula insertion and release of fibrotic tissue. 32 Lisa et al. (2016) suggests that the ADSC create a microenvironment, following tissue regeneration, which encourages nerve release. 4 This includes neo-angiogenesis and increased hydration. ADSC possess anti-inflammatory properties that have been demonstrated in murine studies. TGF-β initiates immunosuppression by acting on T-cells and may be responsible for an analgesic effect. Huang et al. (2015) describe damage to nociceptors and peripheral nerves as the cause of neuropathic pain experienced from scar tissue causing an inflammatory response. 39 It is also hypothesised that the actions of cytokine interleukin 10 (IL-10) are responsible for the inhibiting CD4 and CD8 and thus generating an anti-inflammatory response. 39 ADSC are an abundant source of IL-10.
A significant improvement was detected in studies regarding pain relief following AFG. Huang et al. (2015) demonstrated a rapid analgesic effect of neuropathic pain, just one week after treatment. 3 This was a significant improvement (P < 0.05), using the VAS and NPSI scores. Ulrich et al. (2012) and Caviggioli et al. (2011) both reported long-term analgesic effects at six months and 13 months, respectively, indicating AFG sustainable effects.21,32
This systematic review assessed the efficacy of AFG in treating scar tissue, in 23 articles. Positive outcomes were reported, including restoration of function and aesthetics. This included colour, thickness, pigmentation and relief of pain and itch. Scars ranged from cleft palates to post-mastectomy painful scars, all showing improvement following one or more treatments. This suggests AFG can be used as an alternative to surgical scar excision, in scar-related diseases.
Surgical excision of scars results in increased scar length and potential of worsening scar tissue. AFG has the advantage of being easily available and can be injected in multiple sites of the body. Furthermore, it is not immunogenic, is easily available and, according to Piccolo et al., is a procedure that has a short learning curve for surgeons. 34 The volume filling capabilities allow the natural contours of skin to be regained while counteracting the depressive and retracted nature of scar tissue. AFG is therefore a viable alternative to surgical excision.
This review demonstrated the consistency of the procedure and technique used, when lipofilling. 16 studies followed Coleman’s technique and ensured a maximum surface area between the grafted fat and recipient site. This was displayed by the deposition of fat in multiple planes which enhances graft viability for long-term benefit. Bircoll et al. (1987) recommend increments of 1-mL fat should be deposited in passages in different planes until the full volume has been reached. 40 This was adopted by Byrne et al. (2016), with significant improvement in range of motion in 13 patients with hand scars. 19
The volume injected was in the range of 0.5–80 mL in this review, with variable reasoning in each study. Guisantes et al. (2012) suggests that most clinicians are guided by the size of the scar and states that < 200 mL for any scar means even thin individuals would be eligible for treatment. 26 This is supported by Klinger et al. (2013) and Piccolo et al. (2015), who describe 1 mL per 3.5 cm2 and 1.6–2.0 mL per 10 cm2, respectively.5,34 The majority of studies were guided by volume restoration and degree of retraction rather than scar size when considering the need for a greater volume of fat.
Despite the advantages of AFG, complications were noted in 14 patients. This included postoperative haematoma and infection, need for further AFG sessions and surgical excision of scar tissue following unsuccessful treatment. However, the natural and rapid healing process, in combination with high levels of patient satisfaction, poses promising potential for AFG.
Limitations
There is a paucity of high-quality randomised controlled trials in the literature. This review demonstrates the abundance of evidence levels IV and V with case reports and case series. Furthermore, this review is limited by completeness of data including declarations of loss to follow-up. Observer bias was not reduced with blinding, therefore qualitative assessment of cases and controls by physicians should be interpreted with caution. This can be considered in future studies. Selection bias was noted with the exclusion of confounders, i.e. keloid scars and patients on steroids. Although this heterogeneity is to be expected, study populations varied with the number of treatable and non-treatable scars. Future consideration must be taken of age as a confounder. Huang et al. (2015) demonstrated unsuccessful treatments in patients aged > 50 years. 3 They required multiple sessions and scored low on patient satisfaction surveys. Dini et al.’s (2014) recent work, assessing age and adipogenetic capability of fat, demonstrated reduced ADSC activity. This can be assessed further in future projects. 17
Conclusion
This systematic review evaluates the existing literature and evidence regarding AFG in treating various scars. The documented description of its benefits in improving scar tissue is promising, indicating its ability to reduce functional limitations and enhance cosmetic appearance. Analgesic effects are caused by nerve repair (mediated by BDNF) and scar entrapment release. The injection procedure itself is responsible by making space under scar tissue and it is hypothesised that grafts containing TGF-β play a role in immunosuppression by acting on T-cells, resulting in an analgesic effect. However, there is a limited number of studies that report significant results and a lack of high quality randomised control trials. It is therefore difficult to conclude that AFG significantly improves scar tissue. What can be taken from this study is the potential of this treatment to be explored further in future, with an appropriate sample population and follow-up period. Detailed study of ADSC would be of great interest to support the current hypotheses that are indicated in this review. AFG is a safe treatment method with few complications and it poses promising benefits in future treatment of scar-related conditions.
Footnotes
Declaration of conflicting interests
KS is the editor of Scars, Burns and Healing but was excluded from the peer review process. This work has been presented as a Poster Presentation at the British Association of Plastic, Reconstructive and Aesthetic Surgeons Undergraduate Day in May 2016.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.