
Abstract
There is an urgent need for innovative solutions to address the global burden of mental illness. Evidence for the positive impact of music on mental health is growing; therefore, music may aid in engagement and intervention outcomes as an adjunct to psychological therapy. Psychologists’ intentional use of music within their practice is uncommon and not typically part of psychology training. Drawing on the authors’ disciplinary expertise in clinical psychology, music therapy, community music, and music education, this study aimed to investigate trainee clinical psychologists’ perspectives on the use of musical care as an adjunct to talk therapy. We used a convergent mixed-methods design to investigate trainees’ knowledge, confidence, and willingness to integrate musical care into clinical practice pre- and post- a three-hour experiential education session delivered to three trainee cohorts. Quantitative results indicate the session significantly improved trainees’ knowledge of using musical care, including understanding of the role of music therapy, confidence in using music in therapy, and willingness to incorporate musical care into their future clinical practice. Further, the education session improved student understanding of what music therapists do and increased trainees’ perception of the benefits of referring clients to music therapists. Qualitative analysis revealed that while most trainees used music personally, few incorporated it into therapy sessions. Key barriers included insufficient training and resources, with trainees requesting more evidence-based techniques, case examples, and clearer referral pathways for interprofessional collaboration. These findings highlight the effectiveness of a brief experiential multiprofessional education in promoting interdisciplinary collaboration and expanding therapeutic toolkits. This study presents a practical approach for integrating musical care education—led by music professionals—into clinical psychology training programs.
Keywords
The global burden of mental illness is profound and cannot be addressed by any single discipline or professional group alone. In 2010, the World Health Organization (WHO) advocated for interprofessional collaboration in education and practice to strengthen health systems and improve health outcomes. This watershed framework defined interprofessional education (IPE) as “when two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes” (WHO, 2010, p. 13). Over the last 25 years, IPE has steadily expanded in scope and is now an accreditation requirement for many health professional programs, including those with a mental health focus (Brewer et al., 2024).
Similarly, “musical care” is a term encompassing varied musical practices beyond “boundaried health settings” (Spiro et al., 2023, p. 2), defined as “the role of music—music listening as well as music-making—in supporting any aspect of people's developmental or health needs” (Spiro & Sanfilippo, 2022, pp. 2–3). Musical care provides a valuable framework for healthcare professionals to explore and implement the diverse ways music can support health and wellbeing for clients across the lifespan in clinical settings. However, the interdisciplinary, cross-boundary work of musical care requires significant learning effort and can be complicated by the different discourses each profession brings to the table (see earlier Tsiris et al., 2016 on the challenges of interdisciplinary work in music, health, and wellbeing).
In this sense, then, the multifaceted and interdisciplinary nature of musical care resonates strongly with the spirit and intent of IPE. Within music therapy, for example, the case for IPE is based on the argument that it will enhance teamwork and collaboration and ultimately improve client outcomes (Purvis, 2010). Music therapy researchers have advocated for interprofessional research to strengthen the quality of research and the application of practices such as Guided Imagery and Music (also known as The Bonny Method) (Short & Heiderscheit, 2020). Laahs and Derrington's (2016) phenomenological study found that interdisciplinary peer review between a music therapy student and a dance movement psychotherapy student was beneficial in overcoming some of the challenges identified by Tsiris et al. (2016)—the students broadened their perspectives of other professions and developed cross-professional communication skills (see also Ballantyne & Baker, 2013). A study by Short and Heiderscheit (2023) showed that music therapy teaching faculty often rely on research evidence from other health disciplines to inform their teaching, including seeking information on psychotherapeutic processes.
Despite the reported benefits of IPE, the worlds of clinical psychology, music therapy, and musical care more broadly remain largely separate. Collaboration between music psychology and music therapy disciplines has been marked by epistemological debates, such as the perception that music therapists are “disinterested in science” (Carlson & Cross, 2021, p. 181). One study surveying 123 music therapists and music psychologists found a perception gap between the two groups: Both groups held inaccurate perceptions of each other's attitudes toward interdisciplinary research, yet both were positive and interested in working together across disciplines (Carlson & Cross, 2021). On the psychology side, studies report the benefits of music programs to improve cognitive performance and social identification with older adults (Dingle et al., 2020), emotional awareness and emotion regulation in young people (Dingle & Fay, 2017; Larwood & Dingle, 2022; Sharman & Dingle, 2015), and social wellbeing for young adults (Papinczak et al., 2015). These studies point toward untapped opportunities for collaboration that could be realized by addressing professional misperceptions and creating more formal pathways for interdisciplinary engagement.
Little is known about clinical psychologists’ knowledge, confidence, and willingness to use musical care as an adjunct to “talk therapy.” 1 Clinical psychology is the branch of psychology that focuses on the assessment, diagnosis, formulation, and evidence-based treatment of mental health disorders across the lifespan. In Australia, the title “Clinical Psychologist” is a protected endorsement under the Health Practitioner Regulation National Law. Graduates must first complete a five- or six-year accredited psychology pathway, then a two-year master's degree or three-year doctorate in clinical psychology, followed by a registrar program before full endorsement by the Psychology Board of Australia (PsyBA).
The Psychology Board of the Australian Health Practitioner Regulation Agency requires psychologists to be competent in understanding the roles of other professionals, and working collaboratively with them (Ahpra, 2024). The Australian Psychology Accreditation Council requires clinical psychology programs to educate and assess trainees in their ability to consult and collaborate with other professionals on clinical planning and referrals, particularly in complex case presentations (APAC, 2019). 2 A systematic review of research on the impact of IPE in undergraduate and postgraduate psychology teaching programs revealed that IPE covers a range of health professions, including medicine, nursing, social work, occupational therapy, physical therapy, dietetics, speech language pathology, health science, athletic training, exercise science, and pharmacology (Oxlad et al., 2021). The systematic review does not mention arts in health, music therapy, or other music-based interventions as disciplines or approaches included in IPE for psychology students.
While the gold standard of IPE is characterized by bidirectional learning where professionals from different disciplines learn about, by, and from each other, our study takes an important first step toward IPE by implementing a multiprofessional approach. In this approach, clinical psychology students learned about musical care from a community musician/music educator and a music therapist. Although this approach does not achieve the complete reciprocal learning of IPE, it lays the foundations for future IPE between the disciplines of psychology and musical care.
The multiprofessional approach to education we adopted in our study addresses an identified need for arts professionals to design and lead the integration of creative arts into healthcare education. A recent review by Howlin et al. (2025, preprint) examines the integration of the visual arts, performing arts, and creative writing into health professional education, primarily in nursing and medicine. The review found that arts professionals rarely lead such education, and that it is created in collaboration with them only around one-third of the time. The review highlights the need for more education—led by arts professionals or designed in partnership with them—that covers patient-focused outcomes, community arts, creative arts therapies, and social prescribing. The literature reveals an opportunity to incorporate experiential, multiprofessional, or IPE-based training in musical care (broadly encompassing the roles and activities associated with music therapy, community music, and adjunctive uses) into psychology students’ training.
Adjunct Therapies and Music
Psychologists have begun to explore adjunct therapies that are complementary to talk therapy, such as animal therapy (e.g., equine-, canine-assisted therapy) (Lutzky-Cohen & Schneider, 2017; Maujean et al., 2013; Trevathan-Minnis et al., 2021), yoga (Varambally & Gangadhar, 2016), mobile apps and SMS messaging (Rathbone & Prescott, 2017), dance (Dwarika & Haraldsen, 2023), virtual reality (Freeman et al., 2017), and psychedelics (Luoma et al., 2020). These adjunct methods may be considered based on the psychologist's interest, the client's preference, or when traditional psychological intervention has not been successful. Adjunct methods often aim to improve client engagement, interest, and motivation, and ultimately to meet the client's wellbeing needs and care requirements. Complementary to talk therapy, these adjunct methods may be used by a psychologist in session (if appropriately trained), or the psychologist may refer the client to a specialist in the field to receive the adjunct intervention.
Similarly, the use of music within a non-music therapist's professional scope of practice, such as that of a psychologist, is referred to as the adjunctive use of music (Short & MacRitchie, 2023). Music therapy refers to the use of music by a trained and qualified music therapist to achieve therapeutic goals (Short & MacRitchie, 2023). To become registered as a music therapist, one must complete an accredited music therapy tertiary course and hold current registration with a national music therapy association (AMTA, 2024). Beyond qualified music therapists, some training may be offered to other health professionals. For example, Guided Imagery and Music (GIM), the Bonny Method, is considered an advanced specialist music therapy training (Grocke, 2019), and in some parts of the world, different courses on GIM may be offered to trainees outside of the music therapy field (EAMI, 2025). GIM practitioners use this psychodynamic and multimodal therapy of music listening with clients in a deeply relaxed state to stimulate imagery, memories, and feelings, helping the client understand life issues and promote mental and spiritual wellbeing and health (MIAA, 2021).
Music is less common as an adjunct therapeutic tool for psychologists, perhaps due to common misunderstandings among healthcare professionals. For example, within the nursing profession, such misunderstandings include references to music therapy as a complementary and alternative medicine (CAM) practice (Li et al., 2013). A Canadian study of oncology healthcare professionals’ (mainly nurses’) knowledge and attitudes to music as a therapeutic tool in healthcare differentiated between “music care” and “music therapy” in their survey instrument and included definitions of these terms. Nonetheless, the authors acknowledged as a limitation that healthcare professionals “may not have been clear” on the distinction (Esplen et al., 2020, p. 386). It appears that those surveyed often used these terms interchangeably. The authors concluded that, at least in the oncology context, there is a need for more structured music care education to increase understanding and use. Similarly, a study by Franco et al. (2018) on healthcare professionals’ knowledge and perspectives of music therapy as a CAM suggests some blurring of understandings between the use of music activities or music as an adjunct by non-music therapists versus the use of music therapy by a professionally trained and qualified music therapist.
Perhaps one way to combat this confusion is to include experiential education on musical care. A recent study in the United Kingdom of student nurses’ experience of a creative health placement as part of their curriculum facilitated by community artists showed an overall positive experience of the event (Ridgway et al., 2024). The educational approach was strongly experiential, with students participating in activities involving art, dance, and music creation. While students found the learning experience challenging, the opportunities for self-reflection and learning about the creative arts for self-care were beneficial. Education that includes a receptive experience of music, such as music listening, may also assist learning with the application of music activities in nursing practice (Lai, 2011) and can support physicians’ close listening skills with their patients (Nicholas et al., 2024).
These studies highlight the challenges in educating healthcare professionals about the use of musical care in health settings and the value of experiential learning. Given the use of adjunct and complementary therapies within clinical psychology, musical care as an adjunct therapeutic tool has the potential for widespread application to improve client wellbeing and increase referrals to qualified music therapists. Despite the potential for musical care to support clients’ wellbeing, psychologists’ intentional use of music within their practice is uncommon and not typically part of psychology training. Furthermore, there appears to be a lack of referral pathways and interprofessional collaboration among clinical psychologists, music therapists, and musicians working in the health and wellbeing sector.
Aim, Research Questions, and Hypotheses
Drawing on the authors’ disciplinary expertise from clinical psychology, music therapy, community music, and music education, this study aimed to investigate the perspectives of trainee clinical psychologists on the use of musical care (including community music activities, music listening, and referral to music therapy) as an adjunct to talk therapy. To achieve this aim, we asked the following research questions:
How do clinical psychology trainees use musical care, and what barriers and training needs exist? Does a musical care education session, including experiential activities, improve trainees’ knowledge, confidence, and perceived applicability in practice? How do trainees view musical care in multiprofessional collaboration?
Method
The study used a convergent mixed-methods design whereby quantitative and qualitative data were collected simultaneously and findings are presented together within a combined report to provide complementary information about the topic (Creswell & Clark, 2017). The quantitative and qualitative elements were weighted equally in the study.
Participants
Participants were Master of Clinical Psychology (MCP) students at the University of Southern Queensland, Australia (Table 1). Three different cohorts of MCP students participated in the study: two were provisionally registered cohorts, and one was an advanced entry cohort (MCPA). MCPs are provisionally registered psychologists undertaking a 6th year of study to be eligible for endorsement in clinical psychology, while MCPA students are generally registered psychologists undertaking a bridging year of study to qualify for endorsement in clinical psychology. There were 54 student participants, the majority of whom (77.8%) self-identified as female. The majority (33.3%) of participants were in the 25–34-year-old age bracket. Most of the sample (59.3%) were provisionally registered psychologists; a subset (40.7%) were students enrolled in the advanced entry MCP program and were generally registered psychologists.
Frequencies of demographic categories.

Procedure
Participants attended the education session delivered to the three separate MCP student cohorts during February 2024. Students were informed that study participation was voluntary, anonymous, and unrelated to their program enrolment. The course leader provided verbal research information, and students reviewed a participation information sheet. Implied consent was obtained through completion of a hard-copy pre-session measure assessing knowledge, interest, and confidence in music-related care. Post-session, participants completed a similar feedback measure. Questionnaires were collected by the researchers, with non-participants able to return blank surveys in envelopes to maintain anonymity. Ethical approval was obtained from the Human Research Ethics Committee at the University of Southern Queensland prior to data collection.
Experiential Education Session
Authors MF and JK facilitated the three-hour education session with a 15-min break in the middle. The first section was led by MF (music educator and community musician); it covered the role of arts in health and wellbeing, and introduced the music, health, and wellbeing continuum (Short & MacRitchie, 2023) and musical care (Spiro et al., 2023; Spiro & Sanfilippo, 2022). This section included an experiential group singing activity and reflection. The second section was led by JK (music therapist) and began with an experiential music listening exercise where students connected songs to statements about memories/feelings/emotions, followed by a discussion on using music as an adjunct in clinical psychology practice and the benefits of interdisciplinary collaboration with musical care professionals such as music therapists and community musicians. See Supplementary Materials for detailed session information.
Measures
The measures used were bespoke tools developed by the multidisciplinary research team to align with the session objectives and study aims, designed to maximise face validity (see Supplementary Materials). Before the education session, participants completed a self-report measure including 12 items assessing personal music use, knowledge, confidence, interest, and perceived efficacy of music-based approaches, rated on 7-point Likert scales. Sample items included “I feel confident using music in therapy” (7 = Strongly agree to 1 = Strongly disagree) and “How would you rate your knowledge of what music therapists do?” (7 = Excellent). Two open-ended questions addressed previous experience with music integration and perceived barriers. Higher scores indicated greater knowledge, engagement, and confidence in using music-related activities.
Post-session, participants completed an evaluation measure featuring eight selected baseline items plus three additional Likert-scale items assessing session satisfaction and intention to access further resources. Sample items included “I enjoyed this education session” (7 = Strongly agree to 1 = Strongly disagree) and “In the future, how likely are you to refer a client to a music therapist?” (7 = Very likely to 1 = Very unlikely). Two open-ended items solicited requests for further training and general feedback. Higher scores indicated greater engagement and confidence with music-related activities.
Analysis
Author RI manually entered participants’ questionnaire data into IBM Statistical Package for the Social Sciences (SPSS), version 29.0 (IBM Corp, 2022) for analysis. A participant identification code was generated to link participants’ pre- and post-survey responses. For each Likert item, a change score (post – pre) was computed and screened with the Shapiro–Wilk test; all seven distributions departed from normality (ps < .05). Consequently, pre- to post-change was analyzed with two-tailed Wilcoxon signed-rank tests.
Descriptive statistics (percentages, means, and standard deviations) were calculated to summarize participants’ demographic characteristics and questionnaire responses before conducting inferential analyses. Associations among variables were examined using two-tailed Spearman rank-order correlations, given the ordinal nature and non-normal distribution of the Likert-scale items. Effect sizes are expressed as r for Wilcoxon tests (calculated as |z|/√n; Rosenthal, 1994) and as ρ for Spearman correlations.
To control the familywise error rate, the seven Wilcoxon comparisons (intervention effects) and the five exploratory correlations (variable relationships) were treated as two independent families; Bonferroni-adjusted critical levels were therefore α = .007 for the change-score family and α = .010 for the correlation family, and all p-values reported below are interpreted against these thresholds.
Qualitative analysis was conducted by the two authors specializing in clinical psychology. Authors RI and SB brought the perspectives of practicing clinical psychologists and university educators to the research and were positioned as insiders. Both are committed to interdisciplinary approaches and to integrating innovative practices, such as musical care, into therapy.
Responses to qualitative pre- and post-workshop survey items were explored via Structured Tabular Thematic Analysis (ST-TA) (Robinson, 2022). This form of thematic analysis is designed to analyze brief texts. It uses spreadsheet software such as Microsoft Excel to organize the data and thematizing. ST-TA draws on the ecumenical approach (Boyatzis, 1998) and the reflexive approach (Braun & Clarke, 2006, 2021) (Robinson, 2022). It involves calculating theme frequencies to convey how common a theme is within a dataset. Frequencies may be considered more meaningful in brief-text databases. For the current study, an inductive approach was taken to analyze the data to ensure that the research was guided by the brief texts rather than specific theoretical guides.
The analysis followed the phases for inductive analysis in ST-TA (Robinson, 2022). After data familiarization and repeated reading, initial codes were generated and grouped into clusters to develop themes. Each text line was linked to at least one theme, with some text segments included in multiple themes if they addressed various topics. This inductive process involved working back and forth between themes and data until a comprehensive thematic set was established (Creswell & Creswell, 2022). The next phase involved tabulating the themes against data chunks. Author RI created an Excel spreadsheet to tabulate themes against data segments, enabling clear frequency calculation. Author SB reviewed these allocations to ensure the analytical scheme was transparent, rigorous, coherent, and trustworthy (Robinson, 2022). An agreement consensus exceeding 80% was achieved (Miles & Huberman, 1994). While a theme's frequency does not necessarily reflect its relevance, it provides a precise measure of prevalence across responses (Robinson, 2022). An interactive dialogic approach was adopted by both analysts throughout the analytic process (Russell & Kelly, 2002). This process led to the development of accurate thematic schemes that were a product of the knowledge basis of both analysts. Analysis was then discussed with the research team.
Results
Trainees’ Use of Music
Before completing the education session, most participants (75.9%) indicated that they frequently to always used music as a tool to support their own wellbeing. However, the extent to which trainees incorporated music into therapy sessions was notably lower. The majority (72.2%) of trainees reported that they never or almost never used music during therapy sessions. 31.5% stated that they never suggested music-related tasks (e.g., homework activities) to clients outside of sessions. 24.1% reported rarely to occasionally suggesting such tasks, while only 3.7% frequently did so. The frequency with which trainee clinical psychologists used music to improve their own wellbeing was significantly and positively associated with how often they suggested music-related tasks to clients outside of session activities (r = .361, p = .007).
Participants who had used music in their psychological practice were asked to describe how they used it with their clients. Three themes captured their practices (28 participants, 58% response rate):
Music for emotional regulation (26 participants, 54%) including using music to facilitate relaxation and coping. Participant 8 shared using music “during mindful practice,” Participant 14 reported using “ambient music in the background,” and Participant 25 described having a “client who played guitar and enjoyed music. We explored playing guitar and listening to music to help ground him when he was feeling overwhelmed/anxious/sad/depressed.” Music to activate change through exploration of feelings or homework activities (10 participants, 21%). For example, Participant 49 shared “discussing songs and music the client connects with, the meaning of that music,” and Participant 18 described how they used music for homework tasks: “I have assigned H/W for a client to find a song that explains how they are currently feeling.” Using music to facilitate client engagement (10 participants, 21%). Participant 24 shared how they used music to build rapport and engagement with child clients: “I have used music in a client-centered way, e.g., at a child's request, twice! Once, I was trying to highlight a child's strengths at dance and she taught me some of her concert routine. Another time, a child wanted to share and perform ‘It's tricky' for me, so I put it on.”
Qualitative responses regarding what barriers and training needs exist for trainee clinical psychologists revealed three themes from 42 responses (87.5% response rate):
Insufficient training and resources (31, 73.8%). This theme reflected participants’ need for more training to better understand musical care, including the need to develop skills to use music effectively in clinical practice “in an evidence-based way” and uncertainty about access to and the availability of registered music therapists. Participant 13 stated that she was, “unsure how to best incorporate it to the best benefit of the client.” Further, participants described access to appropriate resources as a barrier to using music in clinical care, such as equipment and sound-proofed rooms. Client or personal factors (11, 26.2%), reflecting statements that trainee psychologists were concerned about their own ability to use music, client preferences, concerns about sensory sensitivities, and cultural considerations (e.g., religion). Participant 23 stated, “…musical talent of self (or lack thereof); embarrassment to put self out there musically.” No barriers (4, 9.5%). Respondents had not encountered barriers, nor did they perceive any barriers to using music in therapy or for training needs.
Qualitative responses obtained post-session that asked about additional training or learning needs indicated two themes from 16 responses (33.3% response rate):
Evidence-based strategies for one's own practice (13, 81.3%) described a desire to learn more about the evidence base for music in one's own clinical practice, including the physiological impacts of music on clients, and specific strategies for using musical care in therapy. Participant 47 stated, “I would like to understand how to integrate this into my practice with some examples and case studies and practice/role plays.” Collaborating with registered music therapists (RMTs) (6, 37.5%) described wanting to learn more about the role of RMTs, accreditation processes, referral pathways, and collaboration.
These results show that participants generally recognize the value of music for personal wellbeing but lack sufficient training, resources, and confidence to incorporate music-based interventions into their therapeutic practice effectively. Some participants highlighted the need for more education on evidence-based musical care strategies and collaboration with registered music therapists.
Musical Care Education Session
Pre- and post-session ratings were examined to determine if a musical care education session improved trainees’ knowledge, confidence, and perceived applicability in practice. There was no significant difference between generally registered and provisionally registered trainee clinical psychologists on any of variables.
Prior to the education session, most participants rated their knowledge of using music for therapeutic purposes as limited. Specifically, 24.1% of students described their knowledge as extremely or very poor, while 57.4% rated it as poor or fair. Fewer than one in five (18.6%) students reported having good or very good knowledge of using music for therapy.
Trainees’ understanding of the role of music therapists was limited. Only 24.5% of trainee clinical psychologists rated their knowledge of what music therapists do as fair to very good. Confidence in using music within therapy was similarly low, with only 14.8% of participants reporting that they felt confident in this area. Despite this, there was strong recognition of the potential value of music in therapeutic contexts, with 81.4% agreeing or strongly agreeing that music can improve client outcomes. Reflecting this recognition, most trainee clinical psychologists (64.8%) reported being very or extremely interested in learning more about music and wellbeing.
Wilcoxon signed-rank tests examined pre- to post-session changes in trainee clinical psychologists’ knowledge, confidence, attitudes, and behaviors related to music therapy and the use of music in clinical practice. All p-values were Bonferroni-adjusted (α = .007). Results indicated significant changes across all variables, suggesting that the education session had a meaningful impact on trainees’ knowledge, understanding, and confidence related to music in therapy, and the benefits of music therapy more broadly (Table 2).
Changes in students’ perspectives pre- and post- education session. NB. p-values are two-tailed and Bonferroni-adjusted within the family of seven comparisons (α = .007). Effect size r calculated as |z| / √n. All tests used Wilcoxon signed-rank due to non-normal difference score distributions.
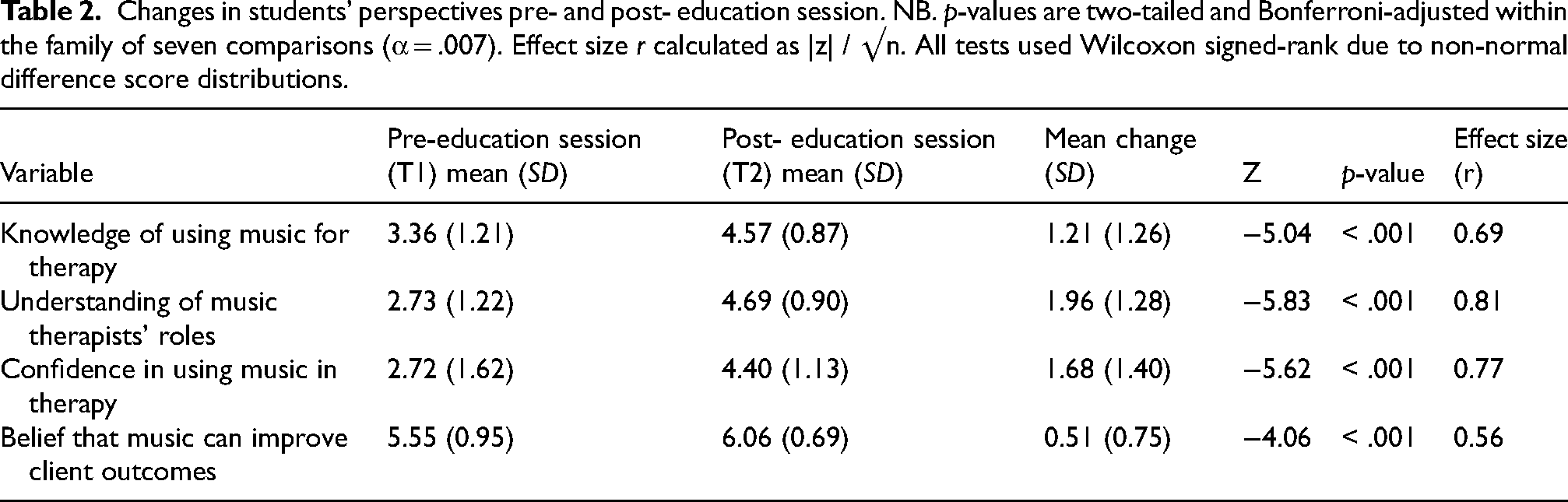
Trainees reported a significant increase in their knowledge of using music for therapeutic purposes, an enhanced understanding of music therapists’ roles, and increased confidence in using music in therapy. Additionally, there was a significant increase in participants’ beliefs that music can improve client outcomes. Overall, all effect sizes were large, suggesting that the education session had a substantial impact on trainees’ knowledge of using music in therapy, confidence in using music in therapy, and beliefs that music can improve client outcomes.
Views on Musical Care and Interprofessional Collaboration
Trainees who reported greater personal use of music for their own wellbeing also showed a significantly stronger interest in learning about music and wellbeing (ρ = .597, p < .001; Bonferroni-adjusted α = .010) and were more likely to refer clients to music therapists in the future (ρ = .371, p = .006). There were positive associations with confidence using music in therapy (ρ = .305, p = .025) and beliefs in its potential to improve client outcomes (ρ = .292, p = .032), but these did not remain significant after correction.
Wilcoxon signed-rank tests examined pre- to post-session changes in trainee clinical psychologists’ intentions related to using music in their own practice and referring clients to music therapists. Results indicated significant positive changes across both variables, suggesting that the education session meaningfully influenced trainees’ engagement with music and intentions for future interprofessional collaboration (Table 3). Specifically, we assessed perceived benefits from referring clients to music therapists, likelihood of using music in one's own therapy practice, and intentions to refer clients to music therapists. Results indicated significant positive changes across all variables, suggesting that the education session meaningfully influenced trainees’ engagement with music and their intentions for future interprofessional collaboration (Table 3). Effect sizes ranged from moderate to large.
Changes in students’ perspectives on the benefits of music, using music in therapy, and working with music therapists pre- and post- education session. NB: p-values are two-tailed and Bonferroni-adjusted within the family of seven comparisons (α = .007). Effect size r calculated as |Z| / √N. All tests used Wilcoxon signed-rank due to non-normal difference score distributions.

Trainees showed significant increases in their beliefs that referring a client to a music therapist could improve client wellbeing. Further, trainees’ likelihood of using music in therapy and referring clients to music therapists significantly increased after the education session. All effects ranged from medium (i.e., use of music in practice) to large (i.e., perceived impact of referring to a music therapist on wellbeing, and likelihood of referral). These results suggest meaningful improvements in their intentions to incorporate musical care and engage in interprofessional collaboration in future practice.
Discussion
This study aimed to investigate the perspectives of trainee clinical psychologists on the use of musical care as an adjunct to talk therapy. Results indicated that most clinical psychology trainees reported they were likely to use music in their future practice following the education session, supporting the impact of even a brief, one-off intervention on knowledge, attitudes, and confidence related to music in therapy and the profession of music therapy more broadly. This is exciting to see and raises the need for more research into the impacts of experiential learning, and in particular, the potential role of aesthetic experiences during music tasks, to enhance understanding of musical care. In the study by Ridgway et al. (2024), while some nursing students reported the experience of participating in a creative health placement as challenging, the authors encouraged all nurses to broaden their views around the benefits of creative arts learning experiences and to be “brave enough to try something different.” This approach aimed to increase nursing students’ awareness and appreciation of these benefits not only for themselves but also for those they care for (Ridgway et al., 2024, p. 3). Similarly, our results suggest that most of the trainee psychologists in this study were open and willing to consider musical care as part of their practice, and indeed most trainees (75.9%) already used music as a tool to support their own wellbeing. Results suggest that a combination of direct instruction, experiential learning, and immediate guided reflection (facilitated both during the education session and through the post-session survey) may help trainees connect their personal experiences with potential clinical applications.
Trainees were eager to learn more about musical care but identified barriers, including insufficient training opportunities and a lack of knowledge about available resources. Trainees requested access to more evidence-based techniques, case examples, and better pathways for interprofessional collaboration. Currently, opportunities to address these barriers are limited. We acknowledge that those seeking to integrate interprofessional education on musical care into clinical psychology training may face structural and institutional challenges. In Australia, an already crowded curriculum aimed at meeting accreditation and competency requirements leaves little room for additional elements, such as musical care and other complementary approaches. Musical care must compete for curriculum space with other allied health professions such as occupational and speech therapy. In Australia, there are few music therapy educators to support interprofessional education (IPE) efforts, with only two accredited programs currently offered nationally. Furthermore, doctors and allied healthcare professionals often lack awareness about the benefits of music in improving health and wellbeing (Forbes et al., 2025).
Trainees requested additional education about clearer referral pathways to enhance interprofessional collaboration. This seems particularly relevant given the rise of social prescribing globally, a public health model that relies on establishing referral pathways between healthcare providers and the community sector to address health-related social needs (Muhl et al., 2023). Psychologists practicing within multidisciplinary settings such as general medical practices and allied health clinics are strategically positioned to enhance patient care through improved referral pathways. These settings create opportunities for formal collaboration not only with music therapists but also with community music organizations that promote health and wellbeing. Integrated multidisciplinary clinics that include embedded music therapists alongside psychologists, while maintaining strong connections to community music resources, would serve a dual purpose: they would demystify “who does what and why” along the “music and health continuum” (Short & MacRitchie, 2023), while simultaneously establishing clear referral protocols. This approach would help practitioners and clients better distinguish between the various modalities under the musical care umbrella—music used adjunctively within therapy sessions, community music activities for wellbeing outside clinical settings, and specialized music therapy as a standalone therapeutic intervention. Such integrated models (of which there are already examples in Australia) would address the referral pathway challenges identified by trainees in our study and support social prescribing, promoting more comprehensive, coordinated care across the spectrum of musical interventions.
We acknowledge the limitations of the current study. The education sessions were a brief intervention with no long-term follow-up or educational support. This was due to limited opportunities within the curriculum for additional IPE and constrained resources. Qualitative data collection could have been more comprehensive. We obtained limited qualitative data on trainees’ experiences of the education session, and in hindsight, we should have asked more questions directly about the experiential elements (group singing and music listening) which, according to pre- and post-measurements, appear to have played an important role in shifting attitudes during the educational sessions. Further, pre- and post-session measures were bespoke tools developed specifically for this project and were not formally piloted prior to use. While measures were reviewed for content relevance and face validity by the multidisciplinary team, future studies should consider piloting or psychometric validation to enhance measurement robustness.
Our ability to demonstrate truly bidirectional learning through interprofessional education was limited; hence we have used the term “multiprofessional” throughout. We did not collect formal learning outcome data from the music facilitators (the music therapist and community musician/music educator). In this pilot, these personnel served primarily as facilitators rather than learners, so the quantitative and qualitative findings represent only one side of the interprofessional exchange—namely, psychology students’ gains in role clarity, therapeutic tool awareness, and understanding of collaborative practice. Although post-session discussion suggested valuable interprofessional insights, these reflections were anecdotal and not captured with the same rigor as the student data. A structural barrier to implementing fully reciprocal IPE in Australia is that only two universities in different states of Australia offer accredited entry-level music therapy programs. Future projects could examine IPE between the disciplines of music therapy and clinical psychology using an online platform to enable comprehensive collaboration and learning.
We acknowledge potential sources of bias in our research team. Authors MF and JK are advocates of music participation for health and wellbeing, while the remaining authors have strong interests in alternative therapies in clinical psychology. To minimize bias, we divided responsibilities: The music researchers handled intervention delivery, while the psychology researchers conducted data collection and analysis.
Future studies could explore clinical psychologists’ experiences during specific music activities such as singing, song sharing, music listening, or songwriting to see what impact, if any, these tasks have on their understanding of musical care. In a group setting, each of these tasks invites the participant to creatively connect with themselves and with others, and, particularly with a singing task, can often be perceived as daunting or uncomfortable. Engaging in these tasks as part of a group in a supported environment facilitated by musical care professionals may also assist participants’ understanding of how their clients might experience daunting or uncomfortable situations. Studies exploring the reciprocal benefits for clinicians and clients could further add to the knowledge base on the benefits of engaging with music for health and wellbeing purposes.
We acknowledge that in different cultural settings there are different professional regulations for clinical psychologists, psychotherapists, and counsellors. As our participants were Australian postgraduate psychology students aiming for clinical endorsement, they entered the workshop with a relatively strong grounding in psychopathology and evidence-based talking therapies, but minimal exposure to music-based interventions. In regions where psychotherapy is delivered by professionals with different baseline competencies, the curricular balance—and therefore the learning gains—may differ. Nonetheless, the core interprofessional principles (clarifying roles, negotiating intervention plans, and experiencing music activities) are broadly applicable. When adapting the workshop internationally, educators should align the depth of psychological content with local training requirements and professional scope regulations.
Conclusion
The findings of this study highlight trainee psychologists’ knowledge, confidence, and willingness to integrate musical care into clinical practice, while acknowledging implementation challenges. Given the competing demands placed on IPE within the clinical psychology curriculum, IPE on musical care is unlikely to be prioritized without greater awareness of the crucial role the arts and music play in fostering health and wellbeing. Even with growing interest in holistic health and interdisciplinary collaboration, practical implementation remains difficult (Jacobsen et al., 2025; see also Forbes et al., 2025). Approaching mental health holistically requires “stepping beyond disciplinary boundaries, to engage interdisciplinary perspectives and initiate creative interventions that support health and well-being” (Jacobsen et al., 2025, pp. 1–2).
The blurred boundaries and interdisciplinarity of musical care make it particularly well suited to IPE, offering healthcare professionals approaches that complement the traditional biopsychosocial model. Our exploration of trainee psychologists’ perspectives on musical care is timely given international calls to recognize creative approaches to health that account for “the complexity of human experiences” (Jacobsen et al., 2025, p. 2). This study demonstrates that multiprofessional education—designed by an interdisciplinary collaborative team featuring experiential learning led by arts professionals—represents a promising first step toward integrating musical care into IPE as a vital component of holistic mental health practice. Future research should focus on developing sustainable models for embedding such approaches in clinical training and practice.
Supplemental Material
sj-pdf-1-mns-10.1177_20592043251397336 - Supplemental material for Multiprofessional Education on Musical Care: Expanding Clinical Psychology Trainees’ Therapeutic Repertoire
Supplemental material, sj-pdf-1-mns-10.1177_20592043251397336 for Multiprofessional Education on Musical Care: Expanding Clinical Psychology Trainees’ Therapeutic Repertoire by Melissa Forbes, Jeanette Kennelly, Renee Ireland, Samantha Brown and Meg Richardson in Music & Science
Footnotes
Acknowledgments
Our thanks to all the study participants at the University of Southern Queensland.
Action Editor
Katie Rose Sanfilippo, City St George's University of London, Department of Population, Health and Policy.
Peer Review
Giorgios Tsiris, Queen Margaret University Edinburgh.
One anonymous reviewer.
Author Contributions
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study was approved by the Human Research Ethics Committee at the University of Southern Queensland (ETH2023-0555).
Funding
The authors disclosed receipt of the following financial support for the authorship and/or publication of this article: This work was supported by a grant from the Centre for Heritage and Culture at the University of Southern Queensland.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.