
Abstract
Individuals with breathing difficulties such as asthma, chronic obstructive pulmonary disease (COPD), and long COVID often experience mood disturbances and isolation. Previous research on musical care has considered the potential of music and singing to support people with respiratory symptoms, but the possible benefits of group chanting have not been explored. Group chanting is a global practice involving controlled breathing through rhythmic vocalizations, but unlike singing or music participation it requires no musical skill. This study examined if 10 minutes of vocal chanting improves psychological wellbeing, social wellbeing, and breathing function. Participants were 41 Australian adults with dysfunctional breathing and 25 with normal respiratory function, who were randomly allocated to group chanting (n = 32) or group guided relaxation (n = 34), with measures taken before and after. Qualitative interviews were undertaken to support the findings and understand the phenomenology of chanting. The results showed that chanting increased positive mood more than relaxation. Both chanting and relaxation improved flourishing and social connection, while decreasing negative mood, with greater and more consistent benefits observed for participants with dysfunctional breathing. Non-attachment, autonomy, and breathing function improved similarly for all participants. These findings suggest that chanting and relaxation may provide psychosocial and breathing-related benefits, particularly for those with dysfunctional breathing. Despite reduced statistical power to detect group differences, the current findings offer promising evidence that warrants replication in future studies.
Breathing dysfunction is defined as irregular breathing patterns and/or the inability to breathe with comfort and ease (Vidotto et al., 2019). Reports have shown an increase in breathing dysfunction worldwide, with a 39.8% increase (544.9 million cases) from 1990 to 2017 (Kisa et al., 2020). Respiratory disorders, including asthma, chronic obstructive pulmonary disease (COPD), and emphysema, were reported to have the third highest mortality rate globally in 2017 (3.9 million). Individuals with respiratory disorders often report suffering from high anxiety, depression, and social isolation (Boulding et al., 2016). In 2021, 27.1% of the total deaths in Australia had underlying or associated issues of respiratory disorders, and in 2022, respiratory disorders comprised 7.3% of the entire disease burden in Australia, which is the eighth-highest leading disease group (Australian Institute of Health and Welfare, 2023).
Treatments for breathing dysfunction in Australia include self-management plans in conjunction with inhalers, pharmacological interventions, oxygen therapy, pulmonary therapy, physical therapy, or surgery, which are coordinated by general practitioners to manage the condition and prevent distressing incidents such as asthma attacks (Australian Institute of Health and Welfare, 2023). However, these treatments are not always effective, can have unwanted side effects, and often do not address the psychosocial issues that accompany and exacerbate breathing disorders, such as social isolation. Singing practices have emerged as a novel approach to improve cardiorespiratory function and psychological and cognitive health (Goldenberg, 2018; Good & Russo, 2022; Kaasgaard et al., 2022; Lewis et al., 2016; Wolff et al., 2023). Singing may be seen as a specific form of musical expression and is the act of producing musical tones with the voice through sustained phonation, controlled breathing, and intentional use of pitch, rhythm, and articulation (Kang et al., 2018).
Musical care—the intentional use of music, sound, and singing for therapeutic or developmental reasons—integrates practices such as singing to address specific health needs, such as breathing function (Spiro et al., 2023; Spiro & Sanfilippo, 2022). For example, singing has been found to support well-being and lung disease through the positive impact it has on mood and social connection (Dingle et al., 2021; Panigrahi et al., 2014). Further, engaging in singing has been found to enhance lung capacity and overall respiratory efficiency, likely through controlled breathing (required in singing), which promotes better circulation and strengthens respiratory muscles, leading to improved cardiovascular health (Bonilha et al., 2009; Kang et al., 2018). Singing has also been found to improve quality of life and pulmonary function in patients with chronic lung disease and breathing difficulties (Bonilha et al., 2009; Cooper et al., 2024; Gick & Nicol, 2015; Skingley et al., 2014). Such evidence is the basis for the SingWell initiative (SingWell.ca), an international cohort of researchers dedicated to exploring the benefits of group singing for individuals with breathing and communication difficulties, with a particular emphasis on its potential to improve respiratory health, speech, and overall well-being. Taken together, research and theory suggest that singing—particularly in group settings—may promote physiological, psychological, and psychosocial health for both healthy individuals and those with respiratory conditions.
It is important to note that singing interventions often involve more than just group singing and often incorporate additional components that enhance their effectiveness, such as posture improvement, breathing exercises, and vocal techniques (Gick & Nicol, 2015; Lewis et al., 2016). These additional “ingredients” play a critical role in achieving the intended physiological and psychological benefits. For example, studies have found that posture and a focus on breathing, integrated into singing sessions, can improve respiratory function and promote relaxation for individuals with breathing difficulties (Gick & Nicol, 2015). Further, Singing for Lung Health (SLH), where individuals with respiratory disease take part in singing groups, is distinct from other singing groups as it focuses on improving posture and breath control, using songs designed for improving respiratory function (Lewis et al., 2016). By focusing on posture and breathing, these interventions may be more impactful than singing alone. Such approaches demonstrate that singing may be used as a therapeutic tool making it an important aspect of musical care.
Health Benefits of Chanting
Chanting, a practice less researched than singing, may also be seen as a musical care practice. Chanting is a practice dating back thousands of years, and it has been used throughout many cultures, religions, and traditions for healing, emotion regulation, and as a form of worship and ritual (Perry et al., 2021; Perry & Polito, 2021). Chanting can be practiced as a group, individually, and vocally with music or without, but it always involves mental or vocal repetition of sounds, phrases, or specific syllables, such as “Om,” (Beck, 2019; Lynch et al., 2018; Perry & Polito, 2021). “Om” chanting, frequently conducted in groups, has been found to strengthen social bonds and reduce stress (Perry et al., 2016, 2023; Simpson et al., 2021). Chanting can be distinguished from singing in that it is more repetitive, more rhythmic, operates at a slower tempo, and is not practiced for aesthetic purposes but for its psychological, physiological, and spiritual impact. Chanting may be especially effective for individuals who feel culturally aligned with such practices and value their historical and cultural significance (Thompson et al., 2023). In culturally and linguistically diverse communities (CALD), individuals may find comfort and strength in chanting practices that affirm their ethnocultural and spiritual identities, in the same way that religious practices can provide a sense of belonging and meaning for those who identify with them (Malviya, 2023).
Psychological and Social Benefits of Chanting
Chanting “Om” has been linked to increased
Chanting may also promote emotional stability through its association to positive mood and by promoting
The active engagement required in vocal chanting may also foster a sense of
Autonomy and connectedness are also key aspects of
The synchronized group activity involved in chanting, whether in live or virtual settings, may also promote
Chanting and Breathing Dysfunction
It is currently unknown whether the benefits of chanting extend to individuals with breathing difficulties and whether such benefits might relieve symptoms of breathing disorders, such as breathing effort, social isolation, and low mood. Compared to other relaxation techniques, vocal chanting may be more effective due to its rhythmic and repetitive vocalizations. Unlike receptive contemplative practices such as guided relaxation, chanting is an active practice, potentially making it more engaging and accessible. Indeed, previous research has found participants reported feeling more engaged in a vocal chanting practice compared to a listening task (Perry et al., 2016). Tanzmeister et al. (2022) found that paced singing can enhance cardiovascular coherence and heart rate variability, similar to paced breathing techniques. Therefore, chanting (a form of paced, rhythmic singing) may lead to better adherence and greater overall benefits for those seeking to improve breathing function and overall well-being.
Chanting may help alleviate the psychological problems experienced by people with breathing disorders. As reviewed, chanting has been found to improve positive mood and reduce stress, anxiety, and negative emotions in healthy and clinical populations (Bormann et al., 2006; Oman & Bormann, 2015). Even brief sessions of chanting can elevate mood and diminish negative feelings (Perry et al., 2016; Simpson et al., 2021). Moreover, chanting may foster a sense of flourishing—an optimal state of psychological well-being characterized by positive relationships, purpose, and competence (Diener et al., 2010; Kemper & Rao, 2017; Seligman, 2011). Such an impact might arise from the communal dimension of chanting, which is likely to strengthen social bonds and increase perceived social support.
Chanting may also benefit breathing function through its physiological effects. Preliminary evidence suggests that chanting may influence physiological responses by promoting regulated breathing and enhancing parasympathetic activity. The sustained exhalations involved in “Om” chanting are associated with slower, rhythmic breathing, which might support autonomic regulation and reduce stress markers (Bernardi et al., 2000). Similarly, guided relaxation emphasizes body awareness and muscle relaxation, which could contribute to decreased physical tension. While these mechanisms show promise in supporting respiratory function and relaxation, further research is required to clarify the extent of these effects and to determine the specific physiological pathways involved.
The Current Study
The aim of this investigation was to determine whether 10 minutes of group chanting improves psychological well-being and perceived breathing function for individuals with and without dysfunctional breathing. The chanting and guided relaxation session involved listening to a recording and either chanting along with the recording (active chanting condition) or relaxing muscles around the body (receptive relaxation condition). Given the prevalence of breathing dysfunction as well as the easy accessibility of chanting, this study aims to provide insights and evidence into the potential benefits of chanting for addressing breathing dysfunction.
Chanting was chosen as an intervention due to its potential to provide psychological and respiratory well-being through active, controlled, and rhythmic vocalization. The rhythmic and repetitive nature of chanting resembles paced breathing techniques, which have been shown to improve cardiovascular coherence and heart rate variability (Tanzmeister et al., 2022). As a form of paced, rhythmic singing, chanting may promote relaxation, adherence, and greater overall benefits for individuals seeking to improve breathing function and overall well-being.
The relaxation condition was included to ensure ethical treatment, as providing no intervention was deemed inappropriate, particularly for individuals experiencing breathing difficulties. Additionally, relaxation techniques are commonly recommended for managing breathlessness by reducing muscle tension and inducing calm (Brighton et al., 2019). Comparing chanting with a relaxation condition allowed us to assess whether chanting offers unique benefits beyond those associated with traditional relaxation practices.
Ten-minute interventions were chosen as previous research has demonstrated that short (8–10- min) meditation practices, including chanting, can positively impact social connection, stress, and anxiety in novice and experienced meditators (Mrazek et al., 2012; Perry et al., 2016; Simpson et al., 2021). Further, this duration aligns with typical session lengths offered by popular meditation apps, making it practical for real-world applications.
The study compared dysfunctional breathing groups with healthy breathing groups to examine whether the immediate benefits of chanting and relaxation are specific to individuals experiencing breathing difficulties or applicable across both populations. By including a healthy breathing group, the study could identify whether chanting uniquely supports dysfunctional breathers in improving respiratory function and psychological well-being or if its effects are broadly beneficial. This comparison also helps to clarify whether improvements in dysfunctional breathers result from their greater capacity for change or if chanting provides universal benefits regardless of baseline respiratory health.
It was hypothesized that 10 minutes of group chanting will have several beneficial effects, immediately following a 10-minute group chanting session, which may match or even exceed the benefits of guided relaxation. Specifically, it was expected that group chanting would increase positive affect and decrease negative affect. Additionally, it was expected that chanting would increase autonomy, flourishing, social connection, and non-attachment. Lastly, given that active vocalization is associated with chanting but not with guided relaxation, it was expected that chanting would improve perceived breathing function more so than a guided relaxation. We also investigated the benefits of chanting and relaxation for individuals with and without breathing difficulties, to provide insight into the potential benefits of chanting and relaxation. To understand the phenomenology of chanting and relaxation, we also conducted qualitative interviews. This approach allowed us to gather personal reflections and perspectives on chanting and relaxation that quantitative measures may not capture. These interviews were intended to complement the quantitative findings, offering a deeper understanding of experiences with chanting and relaxation. Figure 1 illustrates the conceptual study design, conditions, and outcome measures that were implemented.

Illustration of the study design.
Materials and Method
Participants
Participants were recruited via two methods: The Bond University psychology participant pool and social media. Those recruited through the participant pool received course credit, and those recruited via social media were not incentivized. These recruitment strategies resulted in 66 participants (42 females and 24 males) with ages ranging from 18 to 80 years (M = 32.64, SD = 15.93). Of these participants, 41 had breathing dysfunction (classified as scoring over 19 on the Nijmegen Questionnaire or reporting they have a breathing disorder), and 25 had normal respiratory function (scoring less than 19 on the Nijmegen Questionnaire and not reporting a breathing disorder). The Bond University Human Research Ethics Committee approved the current study (GP00045). G*Power 3.1 was used to determine the appropriate sample size for a 2 × 2 × 2 mixed-design repeated measures ANOVA. To obtain .80 statistical power, a medium effect size ηp 2 = .25, and an alpha of α = .05, the required sample size was n = 136 (n = 34 per group) to detect a between-factors effect, n = 36 to detect a within-factors effect, and n = 48 to detect an interaction. Thus, the obtained sample size of n = 66 is adequate to test the within-factors and interaction effects.
Materials
Positive and Negative Affect Scale
The Positive and Negative Affect Scale (PANAS; Watson et al., 1988) was used to measure mood. The PANAS is a 20-item measure, with 10 positive and 10 negative mood items rated on a 5-point scale, ranging from 1 (very slightly or not at all) to 5 (extremely). An example item is “proud” on the positive affect scale and “ashamed” on the negative affect scale. For the current study, the phrasing of the PANAS was modified from “point in your life” to “in the present moment” to capture the immediate feelings of participants. The PANAS has excellent internal consistency of between 0.90 and 0.92 for both positive and negative mood (McAllister et al., 2015).
Perceived Choice and Awareness of Self Scale
The Perceived Choice and Awareness of Self Scale (PCASS; Sheldon & Deci, 1996) was used to measure autonomy and self-awareness. The PCASS is a 10-item measure with 2 statements (Statement A and B) per item rated on a 5-point scale, ranging from 1 (only A feels true) to 5 (only B feels true). Statements are related to autonomy (items 1, 3, 5, 7, and 9) and self-awareness (items 2, 4, 6, 8, and 10). Example statements to choose from for autonomy are (A) “I feel pretty free to do whatever I choose to” and (B) “I do things that I don’t choose to do”. Example statements to choose from for self-awareness are (A) “my body feels like a stranger to me” and (B) “my body feels like me.” In the current study, the PCASS instructions were modified from “in the past week” to “in the present moment” to capture the immediate feelings of participants. The PCASS has good to excellent internal consistency (Cronbach's α = .85 to α = .93; Sheldon & Deci, 1996).
Flourishing Scale
The Flourishing Scale (Diener et al., 2010) was used to measure participants’ sense of purpose, positive relationships, and competence. The Flourishing Scale is an 8-item measure rated on a 7-point scale ranging from 1 (strong disagreement) to 7 (strong agreement) with total scores ranging from 8 to 56. An example item on the flourishing scale to rate is “I lead a purposeful and meaningful life.” Higher scores indicate higher perceived flourishing. The flourishing scale has good internal consistency (Cronbach's α = .87; Fassih-Ramandi et al., 2020).
Non-Attachment
The Non-Attachment Scale (NAS-7; Elphinstone et al., 2015, 2020) assessed non-attachment, defined as a psychological state that allows individuals to engage with their experiences without undue emotional reactivity or attachment to specific outcomes (Sahdra et al., 2010). This scale is a short form of the 30-item measure developed by Sahdra et al. (2010). The NAS-7 is a 7-item measure with a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). An example item is “when pleasant experiences end, I am fine moving on to what comes next.” Total scores range from 7 to 49, with higher scores indicating greater levels of non-attachment. The NAS-7 has good internal consistency (Cronbach's α = .84; Elphinstone et al., 2020).
Inclusion of Other in Self Scale
The Inclusion of Other in Self Scale (IOS; Aron et al., 1992) was used to measure social connection. The IOS included four individual questions using seven Venn diagrams (see Figure 2) to represent feelings of closeness to others. The current study used a variation of the original questions and asked: “Referring to the image, indicate which circle best describes your relationship with (1) your immediate family and friends, (2) your larger community, (3) people from all cultures worldwide, (4) people in the group with you on the Zoom call now.” This adaptation (including four questions rather than just one as in the original IOS) was chosen to assess connections to different relational groups. Scores were averaged across questions to form a total social connection score.

Aron's Inclusion of Other in Self Scale with numbers representing the score of each option (Aron et al., 1992).
Nijmegen Questionnaire
The Nijmegen Questionnaire (NQ; Van Dixhoorn & Duivenvoorden, 1985) is a self-report, 16-item questionnaire measuring respiratory distress and dysfunction and was used to determine participants who had breathing difficulties, distinguishing between two groups (healthy breathing and breathing dysfunction). The NQ is an ordinal 16-item measure with statements rated on a 5-point scale, ranging from 1 (never) to 5 (very often). An example item includes responding to how often symptoms occur such as chest pain and shortness of breath. A score over 19 suggests breathing dysfunction (Looha et al., 2020; Van Dixhoorn & Folgering, 2015). Therefore, any participant with a score of over 19 was included in the breathing dysfunction group (as well as those who reported a formal breathing disorder diagnosis). The NQ has been shown to have good internal consistency (α = .79 to α = .92) over several populations (Grammatopoulou et al., 2014; Pakdee & Piya-Amornphan, 2022).
Visual Analog Scale for Breathing Effort and Distress
The Visual Analog Scale for Breathing Effort and Distress (VAS-E/VAS-D; Hayes, 1921; Lansing et al., 2003) was used to measure perceived breathing effort and distress. The VAS-E is a single item measuring breathing effort, and the VAS-D is a single item measuring breathing distress. Both the VAS-E and the VAS-D are rated on a 10-point scale, ranging from 1 (far below average) to 10 (far above average). Higher scores represent higher levels of breathing effort and distress. Although some scales in this study use a 1–100 range, we opted for a 1–10 scale for the VAS-E and the VAS-D to enhance usability and minimize participant burden. The 1–10 scale simplifies the response process, particularly for individuals experiencing respiratory distress, who may find it challenging to make fine-grained distinctions on a 1–100 scale. The revised 10-point scale is available at [OSF] at doi: 10.17605/OSF.IO/VT43S
Qualitative Interviews
In addition to the quantitative measures, semi-structured qualitative interviews were conducted to gain deeper insights into participants’ experiences with the chanting and guided relaxation interventions. Ten semi-structured interviews explored participants’ emotional, cognitive, and physical experiences of the chanting (n = 5) and relaxation (n = 5) interventions. We made efforts to avoid confirmation bias by using open-ended, non-leading questions that allowed participants to freely express both positive and negative experiences. Questions were neutrally phrased and included opportunities to discuss challenges or critical feedback. The interview questions were as follows:
Could you tell me about your experience with the chanting/guided relaxation today? Were there any specific moments that stood out for you? How did you feel throughout today's chanting/guided relaxation session? Emotions? Feelings? Physical sensations? Were there any challenges participating in the chanting/guided relaxation activity? How did the session today relate to your connection with others? How did the chanting/guided relaxation session offer insights or shifts in perspective? How did the session impact your breathing? Could you describe your overall quality of life? How much opportunity do you have to engage in leisure activities?
Chanting and Relaxation Recordings
The chanting recording began with instructions for posture and relaxation, guiding participants to sit comfortably with a straight spine and closed eyes. It then transitioned to overlapping voices encouraging participants to chant the sound “Om” during their natural exhalations. The recording included variations in rhythm and tone to help participants synchronize their breath and voice with the chanting.
The guided relaxation recording also began with instructions for posture and closed eyes, mirroring the chanting recording. It then provided detailed guidance for systematically relaxing various parts of the body. Both recordings followed the same introductory format to maintain consistency across conditions, and full audio files and transcripts are available at [OSF] at doi:10.17605/OSF.IO/VT43S
Procedure
Participants were invited to attend either an online chanting or relaxation session using video conferencing software. Participants were randomly assigned to either chanting or relaxation (done by alternating chanting and relaxation sessions). Each session had a minimum of three participants (and the researcher) to keep consistency of groups. When participants arrived at the online session, they completed a consent form and demographics, followed by dependent measures (which took around 10 minutes). They then participated in 10 minutes of either chanting or guided relaxation through a recording that was played by the researchers. Thereafter, participants completed the dependent measures again (10 minutes). After completion of the last survey, participants were invited for a 15-min one-on-one interview at a convenient time. Most interviews were conducted directly after the session to understand immediate experiences of chanting or relaxation. However, if the participant wanted to choose another time, they could do so within a week of their participation in the study. Interviews were conducted using video conferencing software and transcribed for qualitative analysis. The total study duration was around 30 min, or 45 min if participants agreed to do a 15-min interview after the Zoom session, with interventions conducted between 4pm and 6pm.
Design and Analyses
To assess group differences in each of the eight dependent variables—Positive Affect (PANAS-PA), Negative Affect (PANAS-NA), Autonomy (PCASS), Flourishing (Flourish), Inclusion of Self (IOS), Non-attachment (NAS-7), breathing effort (VAS-E), and breathing distress (VAS-D)—a series of 2 × 2 × 2 mixed analyses of variance (ANOVA) were used, with one within-subjects factor of change over time (before vs. after intervention) and two between-subjects factors, including intervention type (chanting vs. relaxation) and breathing dysfunction (healthy vs. dysfunctional breathing).
Prior to conducting analyses, all assumptions were tested. Outcomes of Shapiro–Wilk's test of normality on unstandardized residuals indicated violations in negative affect (before (p = .005) and after (p < .001)), flourishing (before (p = .018) and after (p < .001)), non-attachment (after (p < .001)) and breathing distress (before (p = .012) and after (p < .001)). Levene's tests for equality of error variances revealed violations for breathing distress (after (p = .013) and negative affect (before (p < .001) and after (p = .026)). Although ANOVA is robust to minor violations of normality, and the sample size was sufficiently large (Tabachnick et al., 2013), non-parametric testing was conducted to confirm main effects on variables with violations in normality and homogeneity of variance. Wilcoxon signed-rank tests confirmed significant effects of time in negative affect (p < .001), flourishing (p < .001), non-attachment (p < .001), and breathing distress (p < .001). Mann–Whitney U tests detected significant differences between dysfunctional and healthy breathing groups for negative affect before (p < .001) and after (p = .012), flourishing before (p < .001) and after (p = .017), non-attachment before (p < .001) and after (p < .001), and breathing distress before (p = .024) and after (p = .016). As such, the planned 2 × 2 × 2 ANOVA was retained as the analysis approach to explore potential interactions across within- and between-subjects factors.
Planned contrasts were used to investigate the effect of intervention separately for healthy breathing and dysfunctional breathing groups. Two factors informed the decision to use planned contrasts in the absence of a significant interaction. First, when recruiting participants with health-related dysfunction, ethical considerations call for a detailed assessment of interventions that may be beneficial, whereas dismissing potential effects for a dysfunctional breathing group could be viewed as unethical. Second, the use of planned contrasts is consistent with APA guidelines, which recommend their use when there is a clear theoretical basis for the contrasts and tests are driven by a priori hypotheses rather than exploratory analyses. Table 1 outlines all key demographic variables, while Table 2 outlines a summary of 2 × 2 × 2 ANOVA results for outcome variables.
Frequencies of demographic variables (N = 66).

Summary of 2 × 2 × 2 ANOVA results for outcome variables.

Note: degrees of freedom for all analyses (1,62). * is used to indicate values significant at an alpha level .05.
Qualitative interviews were transcribed and assessed using the six-phase thematic analysis approach outlined by Braun and Clarke (2006). First, the primary coder familiarized themselves with the interview transcripts and independently coded features across interviews, collating codes into potential themes. A second coder then reviewed the identified themes to provide feedback and ensure themes were coherent, relevant and accurately reflected in the data. Reliability was verified through discussions between the coders to resolve any discrepancies in theme interpretation. Finally, both coders collaboratively defined and named themes and examples were extracted and related back to research questions and literature. Throughout the process, both coders engaged in reflexive discussions to minimize bias and ensure consistency in theme identification and interpretation.
Sample Characteristics
The final analysis consisted of 66 participants in total with ages ranging between 18 and 80 years old (M = 32.64, SD = 15.93). A total of 32 participants were assigned to the chanting condition (22 with dysfunctional breathing, 10 with healthy breathing), while 34 were assigned to the relaxation condition (19 with dysfunctional breathing, 15 with healthy breathing). A chi-square test revealed no significant differences between breathing dysfunction and healthy breathing groups in terms of gender distribution (χ2(1, N = 66) = 1.01, p = .314). However, an independent samples t-test revealed a significant difference in age between the groups, t(64) = -2.89, p = .005. Table 1 outlines all key demographic variables. Further, descriptive information (i.e., means and standard deviations of all variables for all groups) can be found in [OSF] at doi: 10.17605/OSF.IO/VT43S
Results
Psychological Benefits
Positive Affect
Results of the ANOVA revealed no effect of time F(1,62) = 1.32, p = .254, dysfunction F(1,62) = 0.59, p = .446, or intervention F(1,62) = 0.24, p = .629. A two-way interaction was found for time and intervention F(1,62) = 4.53, p = .037, ηp2 = .068. Planned comparisons revealed that following chanting, only those in the dysfunctional breathing group increased in positive affect (p = .012). Figure 3 outlines mean positive affect scores for healthy and dysfunctional breathing groups across interventions.

Mean Positive Affect scores for healthy and dysfunctional breathing groups across chanting and relaxation interventions at before and after. Note: Error bars represent ± 1 standard deviation. * is used to indicate values significant at an alpha level .05.
Negative Affect
Results of the ANOVA revealed an effect of time F(1,62) = 28.48, p < .001, ηp2 = .315, with negative affect decreasing after (M = 12.86 SE = 0.69) compared to before (M = 17.68, SE = 1.12). Results also revealed an effect of dysfunction F(1,62) = 12.43, p < .001, ηp2 = .167, with the healthy group scoring lower in negative affect on average (M = 12.42, SE = 1.28) than the dysfunctional group (M = 18.12, SE = 0.99). There was no effect of intervention F(1,62) = 0.79, p = .377. A two-way interaction was found for time and dysfunction F(1,62) = 10.67, p = .002, ηp2 = .147. Planned comparisons revealed that following chanting, only those in the breathing dysfunction group decreased in negative affect (p < .001). Following relaxation, only those in the breathing dysfunction group decreased in negative affect (p < .001). Figure 4 outlines mean negative affect scores across interventions in healthy and dysfunctional breathing groups.

Mean Negative Affect scores for healthy and dysfunctional breathing groups across chanting and relaxation interventions at before and after. Note: Error bars represent ± 1 standard deviation. * is used to indicate values significant at an alpha level .05.
Autonomy
Results of the ANOVA revealed an effect of time F(1,62) = 29.14, p < .001, ηp2 = .320, with autonomy increasing after (M = 39.22, SE = 0.87) compared to before (M = 34.63, SE = 0.77). Results also revealed an effect of dysfunction F(1,62) = 14.91, p < .001, ηp2 = .194, with the healthy group scoring higher on autonomy on average (M = 39.65, SE = 1.12) than the dysfunctional breathing group (M = 34.20, SE = 0.86). There was no effect of intervention F(1,62) = 2.35, p = .130. Planned contrasts revealed increases over time in autonomy following chanting for healthy breathing (p = .031) and dysfunctional breathing groups (p < .001). Following relaxation, increases in autonomy were observed in healthy breathing (p = .046) and dysfunctional breathing groups (p = .005).
Flourishing
Results of the ANOVA revealed an effect of time F(1,62) = 22.19, p < .001, ηp2 = .264, with flourishing increasing after (M = 45.97, SE = 0.86) compared to before (M = 42.30, SE = 1.14). Results also revealed an effect of dysfunction F(1,62) = 9.84, p = .003, ηp2 = .137, with the healthy group higher in flourishing on average (M = 47.04, SE = 1.47) than the dysfunctional group (M = 41.22, SE = 1.13). There was no effect of intervention F(1,62) = 0.08, p = .785. An interaction was found for time and dysfunction F(1,62) = 4.87, p = .031, ηp2 = .073. Planned comparisons revealed that following chanting, only those in the breathing dysfunction group increased in flourishing (p < .001). Following relaxation, only those in the breathing dysfunction group increased in flourishing (p = .001). Figure 5 outlines mean flourishing scores across interventions in both healthy and dysfunctional breathing groups.

Mean Flourishing scores for healthy and dysfunction breathing groups across chanting and relaxation interventions at before and after. Note: Error bars represent ± 1 standard deviation. * is used to indicate values significant at an alpha level .05.
Non-Attachment
Results of the ANOVA revealed a main effect of time F(1,62) = 99.01, p < .001, ηp2 = .615, with non-attachment scores increasing after (M = 35.66, SE = 0.60) compared to before (M = 28.33, SE = 0.63). Results revealed a main effect of dysfunction F(1,62) = 20.94, p < .001, ηp2 = .253, with the healthy group scoring higher in non-attachment on average (M = 34.26, SE = 0.78) than the dysfunctional breathing group (M = 29.73, SE = 0.60). There was no main effect of intervention F(1,62) = 0.001, p = .970. Planned contrasts revealed significant increases over time in non-attachment outcomes following chanting for healthy breathing (p < .001) and dysfunctional breathing groups (p < .001). Following the relaxation, increases over time in non-attachment were observed in healthy breathing (p < .001) and dysfunctional breathing groups (p < .001).
Psychosocial Benefits
Social Connection
Results of the ANOVA revealed a main effect of time F(1,62) = 21.15, p < .001, ηp2 = .254, with social connection increasing after (M = 14.18, SE = 0.57) compared to before (M = 11.93, SE = 0.47). There was no main effect of dysfunction F(1,62) = 0.11, p = .746, and no main effect of intervention F(1,62) = 1.03, p = .314. A two-way interaction was found for time and dysfunction F(1,62) = 9.19, p = .004, ηp2 = .129. Planned comparisons revealed that following chanting, only those within the breathing dysfunction group increased in social connection over time (p < .001). Following relaxation, only those in the breathing dysfunction group increased in social connection (p = .003). Figure 6 outlines the mean social connection scores across interventions in healthy and dysfunctional breathing groups.

Mean Social Connection scores for healthy and dysfunction breathing groups across chanting and relaxation interventions at before and after. Note: Error bars represent ± 1 standard deviation. * is used to indicate values significant at an alpha level .05.
Chanting and Breathing Dysfunction
Breathing Effort
Results of the ANOVA revealed no main effect of time F(1,62) = 2.48, p = .121. There was no main effect of dysfunction F(1,62) = 3.09, p = .084, or intervention F(1,62) = 0.22, p = .638. There were no two- or three-way interactions reported. Planned contrasts revealed no significant changes over time in breathing effort scores.
Breathing Distress
Results of the ANOVA for breathing distress revealed a main effect of time F(1,62) = 31.33, p < .001, ηp2 = .336, with breathing distress decreasing after (M = 1.96, SE = 0.25) compared to before (M = 3.60, SE = 0.33). Results revealed a main effect of dysfunction F(1,62) = 4.05, p = .049, ηp2 = .061, with the healthy group scoring lower in breathing distress on average (M = 2.28, SE = 0.40) than the dysfunctional breathing group (M = 3.28, SE = 0.31). There was no significant main effect of intervention F(1,62) = 2.83, p = .098. There was no interaction between intervention and dysfunction F(1, 62) = 3.284, p = .075. Planned contrasts revealed decreases in breathing distress following chanting for healthy breathing (p = .042) and dysfunctional breathing groups (p = .001). Following relaxation, decreases in breathing distress were observed in healthy breathing (p = .047) and dysfunctional breathing groups (p < .001).
Qualitative Interviews
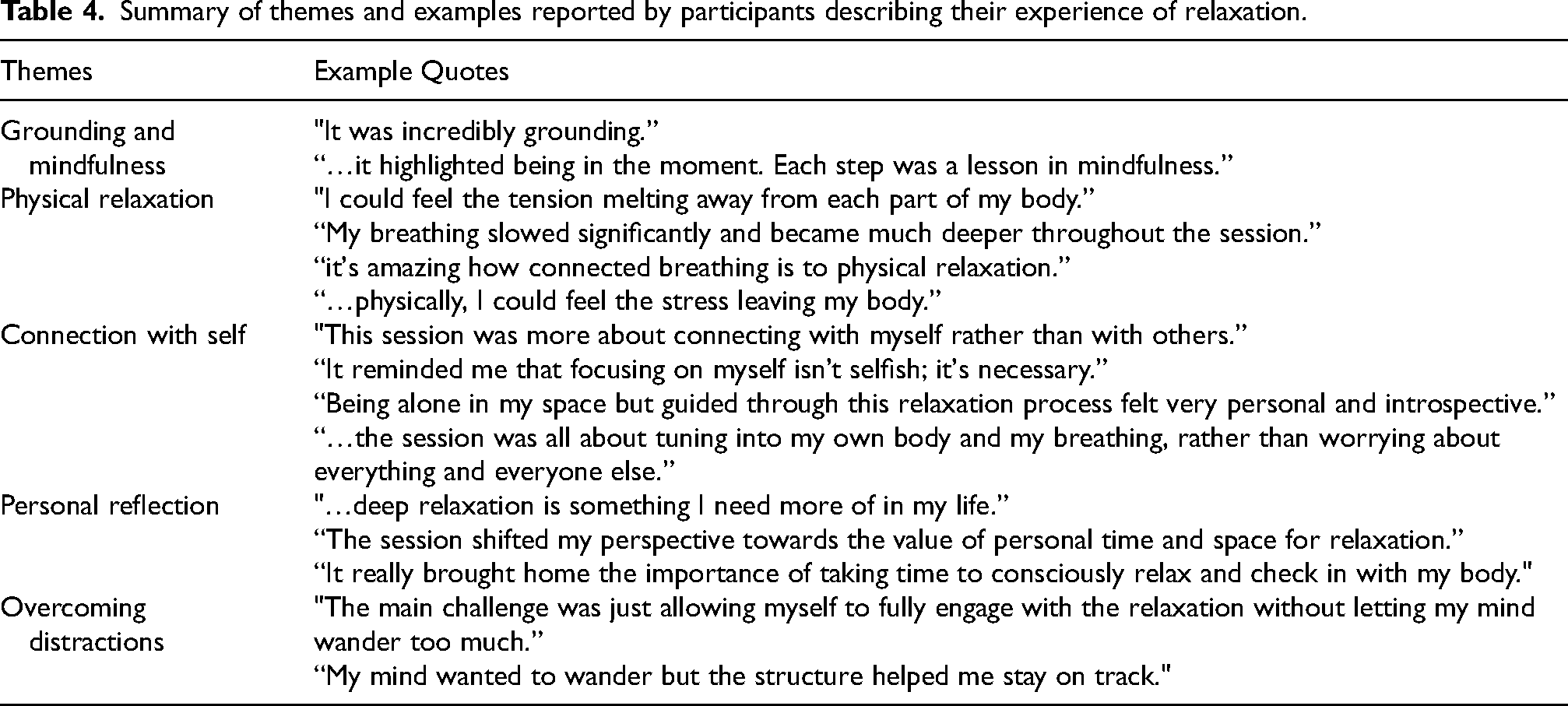
A Braun and Clarke thematic analysis (Braun & Clarke, 2006) was conducted on the qualitative data collected from interviews, to understand participants’ experiences with chanting and guided relaxation. This analysis aimed to corroborate and expand upon the quantitative measures while exploring any qualitative differences in the phenomenology of these practices. The results of the thematic analysis are detailed in Table 3, which summarizes themes when describing their experiences of chanting and Table 4, which summarizes themes when describing experiences of guided relaxation.
Summary of themes and examples reported by participants describing their experience of chanting.

Summary of themes and examples reported by participants describing their experience of relaxation.
Discussion
This study examined the impact of chanting on perceived psychological and physiological benefits for individuals with and without breathing dysfunction by comparing 10 minutes of group chanting to a guided relaxation. Results showed that chanting increased positive mood more than relaxation, especially for those living with breathing difficulties. Additionally, negative mood decreased for those with breathing dysfunction regardless of intervention. Both chanting and relaxation increased flourishing and social connection, with greater benefits for those with breathing dysfunction. Non-attachment, autonomy, and breathing distress improved similarly for all participants across both interventions, regardless of breathing difficulty. It is important to note that the results demonstrated selective improvements in the breathing dysfunction group across different measures. Positive affect increased only after chanting, while negative affect decreased after both chanting and relaxation interventions. Flourishing and social connection showed increases in the breathing dysfunction group following both interventions. These findings highlight the differential effects of chanting and relaxation for individuals with breathing difficulties, with the most consistent improvements observed in negative mood, flourishing, and social connection measures. Although a main effect of time across both groups was observed for several outcomes, planned contrasts often showed significant improvements only among participants with dysfunctional breathing. This pattern suggests that while both chanting and relaxation can benefit general well-being, the effects may be more robust or clinically meaningful in individuals with breathing dysfunction. Future studies with larger sample sizes are needed to determine whether these group differences reflect true variability in responsiveness or insufficient power to detect changes in the non-dysfunctional group.
The study suggests that chanting and relaxation can be effective psychological interventions, offering perceived breathing and psychosocial benefits for individuals with and without breathing dysfunction. The study is novel in that it shows chanting may be as effective as relaxation. Given that chanting is prevalent across various cultures and historical contexts, this widespread use shows the importance of understanding the unique benefits of chanting, even when they overlap with those of relaxation. The cultural ubiquity of chanting suggests that it fulfills various psychological, social, and physiological needs that may not be fully replicated by other relaxation methods.
Mood
Results showed that chanting increased positive mood more than relaxation, with this effect driven by individuals with breathing dysfunction. This benefit of chanting is consistent with several previous studies showing that chanting can increase positive mood (Perry et al., 2016; Simpson et al., 2021). However, this research extends findings to individuals with dysfunctional breathing, for whom chanting might have provided a sense of relief leading to increased positive mood. In contrast, individuals without breathing difficulties might not have experienced the same level of immediate physiological and psychological relief, resulting in a less noticeable impact on their mood. When interpreting these findings, it is important to consider baseline differences between groups. For measures such as negative affect and flourishing, the breathing dysfunction group started from more impaired baselines compared to the healthy group, and while they showed significant improvements, they did not reach the baseline levels of the healthy group. This suggests the interventions promoted meaningful improvements rather than complete normalization of scores.
Negative mood decreased following both chanting and relaxation, consistent with research showing chanting and relaxation may decrease depressive symptoms (Pospos et al., 2018; Wolf & Abell, 2003). Further, the dysfunctional breathing group had more pronounced effects. Dysfunctional breathing refers to breathing patterns that are abnormal or inefficient, associated with conditions like asthma, chronic obstructive pulmonary disease (COPD), or anxiety disorders. Individuals with these conditions may experience heightened stress and negative mood due to their breathing difficulties (Goodwin et al., 2012). Therefore, contemplative practices such as chanting and relaxation may have both alleviated discomforts associated with breathing issues, leading to both a boost in positive mood and a decrease in negative mood. Taken together, these findings suggest that chanting may increase positive mood more than relaxation and that other contemplative practices (such as a guided relaxation) may be just as effective as chanting at reducing negative mood for individuals living with breathing difficulties.
Flourishing and Social Connection
Flourishing and social connection only increased for individuals with breathing dysfunction in both chanting and relaxation conditions. This is aligned with research that has found chanting and guided relaxation to promote mindful awareness, emotional regulation (Bormann et al., 2014; Malviya et al., 2023; Matko et al., 2021; Perry et al., 2022), and altered states of consciousness associated with profound feelings of peace and unity (Perry et al., 2021; Perry & Polito, 2021). Participating in group activities has also been found to promote social connection (Dingle et al., 2021; Hobson et al., 2018; Kniffin et al., 2017), which may further contribute to a sense of well-being and flourishing. This research extends previous findings by examining individuals with dysfunctional breathing, who may have derived greater feelings of flourishing and social connection from chanting and relaxation. In contrast, healthy participants did not show significant effects of flourishing and social connection, likely because they did not experience the same stress or anxiety related to breathing. Therefore, while both chanting and relaxation were effective for individuals with breathing challenges, they did not produce as noticeable improvements in flourishing and social connection among participants without breathing issues.
Qualitative interviews support findings of increased social connection, as can be seen in Table 3 in the theme of connection with others. While participants reported feeling more connected to the self in the relaxation group, as can be seen in Table 4 in the themes connection to self and personal reflection. These themes highlight distinct benefits of chanting and relaxation, emphasizing their respective roles in fostering social connection and self-awareness.
Autonomy and Non-Attachment
Autonomy and non-attachment were found to increase over time for both chanting and relaxation for all participants, irrespective of breathing function. Both group chanting and guided relaxation may have empowered participants by providing them with tools to change their emotional and physiological state. Engaging in chanting involves deliberate breathing and vocalization, providing a tool for self-regulation (Bernardi et al., 2000; Perry et al., 2023). Similarly, guided relaxation practices emphasize self-awareness and mindfulness, encouraging participants to take an active role in their mental state (Malviya et al., 2023). These findings are supported by qualitative responses in themes such as empowerment in the chanting group reported in Table 3. For individuals with breathing dysfunction, who generally reported lower autonomy levels, these interventions might have been particularly useful. The practices may have given individuals more confidence to manage symptoms. The increase in autonomy suggests chanting and relaxation are potential interventions to promote self-efficacy in populations with and without breathing difficulties.
Breathing Function
Engaging in both relaxation and chanting led to a significant decrease in breathing distress for all participants, regardless of breathing function. This is interesting, given that research shows listening to relaxing music has no impact on breathing function in COPD patients (Frischen et al., 2022). However, active muscle relaxation may be more effective than receptive listening as participants were actively relaxing parts of the body in the guided relaxation. This is supported by qualitative responses related to physical relaxation. These findings suggest diverse features of chanting and relaxation (like lengthening exhalations with vocalization during chanting or consciously releasing tension from targeted areas of the body during the guided relaxation) were effective in alleviating breathing distress. Unique aspects, such as the repetitive “Om” vocalizations in chanting, may not be essential for improving perceived breathing distress. Previous research has shown that chanting promotes beneficial breathing in healthy individuals (Bernardi et al., 2001; Mooventhan & Khode, 2014); however, again, this study extends findings to individuals with breathing dysfunction and indicates that relaxation can also alleviate breathing distress.
Qualitative Findings
The qualitative findings presented in Tables 3 and 4 reveal both similarities and differences in experiences of the practices, reflecting some distinct and some overlapping benefits of vocal chanting and relaxation practices. One similarity is in the theme of connection—with others in Table 3, related to vocal chanting, and with self in Table 4, related to relaxation. Chanting practices often foster a sense of unity and collective experience, which may be emphasized through synchronized vocalizations with the recording. In contrast, the guided relaxation seemed to provide more introspection, guiding individuals toward bodily awareness.
Another point of difference comes in the themes of empowerment in chanting and personal reflection in relaxation. Both reflect shifts in participants’ perspectives; however, one is around gaining control and the other personal insight. Chanting may emphasize overcoming challenges, such as vocalizing publicly, which could be related to overcoming challenge, another theme that came from vocal chanting. Overcoming challenges such as the discomfort of vocalizing may be contributing to feelings of strength and empowerment. Relaxation, in contrast, encourages personal reflection through more of an internal focus of relaxing parts of the body, leading to personal reflection rather than feelings of empowerment.
The themes of well-being and physical relaxation illustrate some similarities, as both practices support physical and emotional calm. Chanting's rhythmic nature and sound vibrations likely engage the nervous system to enhance these outcomes, while relaxation achieves similar effects through relaxation and body awareness. The differences in emphasis—chanting on collective connection and relaxation on solitary introspection—highlight the unique psychological and physiological experiences each practice provides.
Limitations and Future Research
This study provides some insights into the effects of chanting and relaxation; however, certain limitations warrant consideration. One limitation of this study is the repeated testing before and after interventions, raising the possibility that observed improvements in psychological and physiological measures could be due to a testing effect. Completing the assessments a second time might naturally result in improved scores as participants become familiar with the tasks, regardless of the intervention. Future studies should incorporate control groups tested only once or include additional control conditions to assess the potential impact of repeated testing on outcomes. Moreover, while this study demonstrated distinct benefits associated with chanting and relaxation, future research should explore the role of individual preference for these interventions. Preferences for chanting or relaxation may influence outcomes, as those who prefer a particular practice might experience greater engagement and consequently more pronounced benefits. Including preference assessments in future studies could provide further understanding of how personal inclination toward a specific practice might affect outcomes. On this note, many participants reported having chanted before and may have been familiar with the practice of chanting and/or experienced long-term benefits. This may have also impacted the results or may have led to response bias whereby participants report more favorably on a practice that they already believe works. This could have occurred for both the chanting and the relaxation groups.
It is important to acknowledge that the sample size in subgroup analyses may have limited the statistical power needed to detect differences between those with and without dysfunctional breathing. Planned contrasts confirmed the significant main effects for participants with breathing dysfunction but often failed to reach significance for those with normal respiratory function. Further research with larger samples should be conducted to confirm these group-specific findings.
Finally, further work is needed to examine the long-term effects of chanting and relaxation, as well as the potential for these practices to be integrated into routine health and wellness programs. Longitudinal studies would be beneficial in identifying whether the benefits observed here are sustained over time.
Conclusions
The benefits from chanting and relaxation for individuals with breathing difficulties highlight the potential of such contemplative practices to address the unique challenges faced by this group. This research enhances our understanding of how contemplative practices can be systematically applied to improve health outcomes, particularly for those with respiratory challenges. This may lead to practical applications, such as incorporating chanting and relaxation into comprehensive care plans for those with breathing difficulties. Recognizing and incorporating these techniques can benefit diverse cultural groups and hold promise for broader healthcare application, supporting both those with and without respiratory issues. Incorporating contemplative practices into traditional medical and psychological treatments may promote fast recovery, reducing symptoms associated with breathing difficulties. The implications extend to policy considerations, advocating for the inclusion of chanting and relaxation techniques in funded health programs. This study has expanded the understanding of chanting's benefits beyond traditional relaxation techniques. By confirming hypotheses that chanting enhances positive affect, autonomy, and perceived breathing function, this research contributes to understanding of how chanting particularly benefits individuals with breathing difficulties, offering valuable insights for targeted therapeutic interventions. The current research supports the need for broader recognition and integration of contemplative practices in healthcare, which may be welcomed by ethnocultural groups familiar with such practices. The potential for tailored contemplative practices to support individuals with and without breathing difficulties offers a promising direction for future research and practice.
Footnotes
Acknowledgments
We thank the Bond University and Macquarie University Music and Sound Research Group for feedback and support.
Action Editor
Neta Spiro, Royal College of Music.
Peer Review
Renee Timmers, University of Sheffield, School of Languages, Arts, and Societies; Natalie Peluso, The University of Queensland, Psychology.
Author Contributions Statement
Conceptualization, G.P. and W.F.T.; Data collection, J.S. and F.A.; Formal analyses, L.W., J.S., F.A.; Methodology, G.P. and W.F.T.; Writing, reviewing and editing, G.P., J.S., F.A., L.W., W.F.T. All authors have read and agreed to the published version of the manuscript.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Data Availability Statement
The data presented in this study are openly available in [OSF] at doi:10.17605/OSF.IO/VT43S
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Bond University (13Sep2023/GP00045).
Funding
This research was supported by a Discovery Project grant awarded to W.F.T. by the Australian Research Council (DP210101247) as well as a Partnership Development Grant funded by the Social Sciences and Humanities Research Council of Canada [www.singwell.ca] (890-2017-0130).
Supplementary Materials
Supplemental material for this article is available online: Qualitative interview transcripts and intervention recordings are openly available in [OSF] at doi:10.17605/OSF.IO/VT43S