
Abstract
Inducible laryngeal obstruction (ILO) is an upper-airway disorder involving a heightened sensitivity of the larynx, obstructing airflow and potentially leading to breathing difficulties. Speaking can trigger, and be affected by, ILO symptoms. This research explored the feasibility of singing-related workshops for people with ILO. The aim was to increase participants’ vocal confidence by combining relaxation with improved control, tone, and projection. Five participants consented to participate in the research. The workshops were led by a voice teacher (VT) and a speech and language therapist (SLT), focusing on posture, breathing techniques, and singing techniques. Ten weekly workshops took place online, with the final session being hybrid where most participants attended in person. Data collection included weekly response forms with Likert scales to rate speaking and singing confidence and feedback on the workshops; interviews with VT and SLT; workshop observations; and a participant reflection questionnaire following the program. Participants reported a significant improvement in speaking and singing confidence as the workshops progressed. Thematic analysis revealed four themes: improvements in confidence, specifically in speaking and singing; the value of social support and meeting others with the condition; specific techniques and approaches that were beneficial; and benefits and disadvantages of the online format. This research demonstrates the feasibility of group singing workshops for people with ILO who do not have a background in singing, using an online format. It confirms the potential benefits of using singing-related techniques for this condition, supporting confidence in speaking and singing. Further research would be useful to extend the findings from this initial project and to provide a firm basis for introducing further programs using singing-related techniques for people with a range of upper-airway disorders. Future developments could include introducing these techniques in clinical settings and using them alongside (or as part of) speech and language therapy.
Keywords
Introduction
Inducible Laryngeal Obstruction (ILO) is an upper-airway disorder involving a heightened sensitivity of the larynx. It is “an inappropriate, transient, reversible narrowing of the larynx” (Halvorsen et al., 2017, p. 1), which leads to breathing difficulties caused by airflow obstruction at the glottic and/or subglottic level. This occurs in the absence of any structural or neurological abnormalities (Haines et al., 2021). ILO is also known as paradoxical vocal fold movement (PVFM). Symptoms include coughing, wheezing, and a choking sensation, usually on inspiration, caused by a tightening of throat muscles that obstructs airflow in the throat. Common triggers are exercise, irritants, and emotional stress (Daly, 2020), so ILO can have a notable impact on many aspects of an individual's life. As ILO is a relatively rare condition, it can be diagnosed late or misdiagnosed as (for example) asthma (Murphy, 2019), which can lead to incorrect medication and advice, triggering further physical problems. Furthermore, psychological and emotional effects commonly arise from feeling misunderstood and uncertainty around diagnosis. The condition can lead to social isolation and loss of work from the reduced ability to communicate with ease, particularly in stressful or challenging situations. These effects can adversely affect relationships with family, friends, and colleagues, who might not understand the condition.
Speech and language therapy holds many benefits for those with upper-airway disorders, including providing correct diagnosis, reducing frequency of symptom attacks, reducing admissions to hospital, and decreasing dependency on medication (Murphy, 2019). Speech and language therapists (SLTs) help the individual to manage their symptoms by providing advice on upper-airway function and ways to optimize care of the larynx, and by introducing strategies and techniques to support laryngeal function. This includes, for example, nose/pursed-lips breathing to filter out irritants, reduce the air temperature changes in the throat, and reduce airflow speed in the larynx, and emergency strategies known as “rescue breathing” where the individual deploys a quick sniff or a pursed-lips inhalation (Murphy, 2019). The employed techniques work to normalize laryngeal function, release inappropriate laryngeal constriction, optimize respiratory rate, and improve the coordination of breathing and voicing.
Seeing commonalities between objectives of singing-related techniques and strategies to regulate laryngeal function, the voice teacher (VT; third author) and SLT (fourth author) worked together to explore the feasibility of singing-related workshops to support vocal confidence in people with ILO. A research project was designed to capture the experiences of the participants and document the outcomes of the workshops. The workshops aimed to increase confidence in opening the upper airway and, in particular, regulating breathing patterns by using the voice for speaking and singing. The VT taught appropriate singing techniques to emphasize the importance of using the voice correctly and carefully, including maintaining good posture when speaking and singing to minimize vocal workload. Activities are deliberately referred to as “singing-related” to refer to the broad spectrum of techniques associated with the program, including posture, breathing, and relaxation of the face and body, movements and stretches, hums and open vowel sounds, and learning of songs. The research focused on regular self-report data collection measures, which then informed the direction, pace, and intensity of the workshops.
This research may be valuable for ILO patients and their clinicians, and may also be applicable to other respiratory conditions with similar symptoms to ILO, including asthma, chronic obstructive pulmonary disorder (COPD), and chronic cough.
Literature Review
Social Bonding
There is longstanding evidence on the benefits of singing in group settings and the effects this may have on elements of physical, mental, and emotional wellbeing (Clift & Hancox, 2001; Daykin et al., 2018). Adopting singing for people with ILO may offer a platform to combine benefits of speech and language therapy with the holistic affordances of group singing.
Group singing is found to increase social bonding and provide a sense of self and community through shared goals (Daykin et al., 2018). Kreutz (2014) used a naturalistic controlled trial to investigate links between group singing and social bonding. Comparing changes over time between a group singing condition and a chatting condition showed that participants in the group singing condition had an increase in the hormone oxytocin, associated with positive social bonding. This suggests that group singing may facilitate stronger social bonding compared to talking-group therapies. Similarly, Bullack et al. (2018) explored psychobiological effects of singing through measuring social connectedness in groups of singers who partook in either a 30- or 60-min rehearsal. A longer rehearsal time contributed to increases in social connectedness, demonstrated by higher self-report ratings of feelings of belonging and group cohesion. Pearce et al. (2015) found group singing to be particularly effective as an “ice breaker” for encouraging and expediting social participation and feelings of “belonging.”
Wellbeing
Research has shown that musical participation, and singing groups in particular, can improve feelings of wellbeing and have positive emotional effects. Robens et al. (2022) found higher ratings of mental wellbeing were reported among people who had frequently engaged in group singing and that ratings of mental wellbeing increased in accordance with the amount of time they engaged in the activity. Furthermore, increased ratings of wellbeing positively correlated with healthy singing habits and vocal warm-up exercises. A large sample size of 847 and a wide age range among participants suggests some generalizability of these results.
Judd and Pooley (2014) also explored the reported benefits of singing for regular participants in choral singing. Interviews revealed that psychological, physical, social, and musical factors played a role in people's experience of group singing. References were made to the group ethos and social dynamics, past experience of singing, type of choir, and the musical and interpersonal skills of the musical director. Several participants noted singing as beneficial during recovery from illness, coping with life transitions, and managing work-related stress.
The aforementioned studies involved participants who regularly engaged in choral singing. Therefore, to obtain a well-rounded view of the benefits of group singing, we must consider the perspectives of those not regularly involved in group singing. Cohen (2009) found improvements in emotional stability and happiness of adult prisoners (previously non-singers) who had participated in group singing sessions. Corvo et al. (2020) measured the outcomes of introducing regular community singing to a group of older adults. Following the singing experience, participants showed decreases in levels of anxiety and depression. Although adults who sing in community choirs often report improvements in mental wellbeing and mood, these studies are usually cross-sectional or lack a control condition, and therefore the exact causality of the outcomes cannot be fully determined (Johnson et al., 2015).
Singing for Physical Health Problems
Research on group singing for people with physical health problems, including respiratory conditions, has shown it to boost confidence, improve control of breathing, and facilitate a sense of community, thus providing valuable social and physical health support (Lord et al., 2012; Thomas et al., 2015). The majority of studies exploring this topic include people affected by cancer (Warran et al., 2019) or COPD (McNaughton et al., 2016), among other respiratory conditions. Skingley et al. (2014) found that group singing improved wellbeing in people living with COPD by providing a sense of purpose, boosting general confidence, and providing coping strategies. Although participants reported their condition sometimes limited their ability to participate, Lord et al. (2012) found singing workshops improved breathing and increased breath control in those with COPD, alongside providing support from others with the same condition. Similarly, Clift and Hancox (2001) found that singing improved self-reported lung capacity and breathing regulation, further justifying the potential of singing for improving respiratory conditions. More recently, research by Cahalan et al. (2022) showed group singing to help reduce breathlessness, lower fatigue, and improve voice quality.
The above studies provide evidence that group singing and singing interventions for people with respiratory problems can be effective and demonstrate social, mental, and physical benefits. The current project draws on the approaches and areas discussed by the studies above. ILO is a complex and lesser-known condition, so there has been a lack of prior research into musical interventions, including singing support, for people with ILO. This project examines the benefits and challenges of singing for those with disorders affecting laryngeal function and suggests recommendations for future research and the development of accessible singing interventions.
Method
Participants
The participants were NHS outpatients with a diagnosis of ILO and were recruited by the SLT to participate in the workshops. Separately, they were asked whether they would voluntarily participate in the associated research. Ten participants took part in the workshops and were undergoing or had taken part in therapy with the SLT. Five participants consented to also participate in the research. All ILO participants were female, and ages ranged from 42 to 68 (mean = 57.6). Data analysis focused only on participants who had consented to participate in the research. Workshop attendance fluctuated from two to eight participants per session due to holidays and illness. Additionally, the VT, who led the workshops, and the SLT, who works as a clinical consultant in voice and respiratory disorders, participated in the research. The VT had a diverse portfolio of work as a performer, teacher, conductor, and workshop leader with experience in dealing with people with vocal problems. The SLT specialized in treating individuals with conditions affecting laryngeal function, specifically ILO and clinical voice disorders, and had a singing and musical background, which she had found influenced her therapeutic approach with some patients. She had noted that voice- and singing-related techniques had appeared to contribute to improvements in symptoms and confidence, and wished to further explore the potential of this approach in a group setting. The VT and SLT carried out pre-workshop familiarization sessions (informal interviews) with each participant to understand their individual situations, the status of their condition, and its effects on their lives.
Ethical Considerations
This project was granted ethical approval in accordance with the University of Sheffield ethics procedures. Participants provided consent via an online information sheet and consent form. They were informed that they could withdraw from workshops or the research at any time without consequences, data would be kept confidential and secure on the university’s Google Drive, personal data would be deleted after project completion, and quotes or data used in the writing up of the research report would remain anonymous. As participants were considered clinically vulnerable, particular care was taken to ensure workshops were entirely focused on how the individuals were feeling each week, on the self-reported condition of their voice and confidence levels, on providing a safe space for them and their condition, and on encouraging and supporting progress and development of voice confidence. Participants were encouraged to take a break if they felt physically or vocally tired and to abstain from any exercises with which they were uncomfortable. Individual advice was also given on how to avoid strain and reduce fatigue. Collaborating partners in this project (VT, SLT, technician, and organizer) are included as co-authors as they provided key expertise enabling the conception and realization of the project. However, the main research was done independently by the first author under supervision of the second author.
Research Materials
Qualitative research methods were adopted to gain a deeper understanding of participants’ experiences of the workshops and their condition, with support from quantitative data. Triangulation was achieved by using four different data collection methods: interviews, observations, reflective notes, and questionnaires. The VT and SLT participated in a semi-structured conversational interview with the first author before the program of workshops began, and a similar interview following the program. This provided information on organizational aspects of the workshops, reflections on participants’ progress, and commentary on the challenges and successes of the workshops. During the workshops, the first author made observational notes regarding how participants responded to the techniques delivered, including spoken quotes and typed quotes from the online chat box.
The online delivery of workshops was facilitated with the support of an audio-visual technician and allowed observation and note taking concurrently using a split-screen function. During each online session, the structure of the workshop; participant attendance; and the exercises used for improving posture, relaxation, breathing, and vocal tone were noted in the first author's research journal. Online Padlet forms for writing down reflective notes were used as a method of “checking-in” at the start of each session and reflecting at the end. Padlet forms included both qualitative and quantitative questions requiring ILO participants to provide written answers and rate voice confidence ratings on a five-point Likert scale. Questions included: How confident do you feel using your voice for speaking and for singing? Which techniques have you used since the last workshop? Which techniques do you find most beneficial? For written Padlet responses to be included in the research, participants consented by adding a “Y” for “yes” at the end of their response. Following the program, four participants completed an online reflective questionnaire (Google Form) to provide feedback on the workshops, with space to discuss how the workshops affected their voice and ILO condition.
Workshop Procedure
The workshops were organized and supported by ‘charity name’ at X Teaching Hospitals NHS Foundation Trust. The research was designed to be observational, minimizing interference with the workshop procedures. Before data collection, all participants were given information about the program and gave written informed consent to participate in the research. There were 10 weekly workshops (each lasting for one hour), which were conducted by the VT between February and May 2022. Workshops were conducted online using Microsoft Teams, with the exception of the final session, which was held in-person in the Department of Music at The University of Sheffield. The login details for the Microsoft Teams online workshops were only shared with those who had signed up to the sessions and required a PIN.
During the online workshops, participants were encouraged to keep their cameras on and, periodically, to turn on their microphones during vocal exercises and discussion. There was a “raise hand” function and a chat box so participants could comment or ask for help at any time. Information was provided prior to commencement of the workshops on how to use Microsoft Teams. A technician was present to help with any technical issues, such as internet connectivity, and to support participants in using the online platform. The VT provided a “culture document” defining the ground rules for the workshops. These included statements such as “there is no pressure to achieve perfection” and “only participate if you feel comfortable with an exercise.” The development of the sessions followed a collaborative emergent approach as the VT and SLT continually responded to participants’ feedback to adapt and/or improve the sessions.
The workshop structure was as follows: welcome and check-in written reflection, posture check and relaxation exercises, breathing exercises, humming and vowel sounds, singing exercises, learning lyrical phrases/short songs, and written reflection and an opportunity to socialize. All written reflections were recorded by participants using a password-protected platform called Padlet.
Data Analysis
Qualitative data was thematically analyzed according to principles established by Braun and Clarke's (2006) method for identifying, analyzing, and reporting patterns within data. Interviews were recorded and transcribed using Scribbl. Quotations from interviews, written reflections, and the final questionnaires were organized thematically. Measurement of individual progress was not possible as all data was provided anonymously. The data did not follow a specific distribution. Therefore, nonparametric tests were used to observe trends in median ratings for each week for speaking and singing. Written reflections were completed at the beginning and end of 8 out of the 10 workshops. Microsoft Excel and Statistical Package for the Social Sciences (SPSS) were used to create line graphs and perform nonparametric tests.
Findings
Quantitative Data – Confidence in Speaking and Singing
Median confidence ratings of participants reported at the start and end of workshops are presented in Figure 1 for the eight weeks in which data was collected. The number of attendees and research participants per week fluctuated, with the lowest being two participants.

Median of speaking confidence ratings (left) and singing confidence ratings (right) (1 = not confident – 5 = highly confident) from weeks 2–10 of workshops (average of the ratings at the beginning and end of workshops).
Speaking confidence started at a higher level than singing confidence, which was minimal at the beginning of the project. Confidence fluctuated across weeks due to contextual situations, such as reports of COVID or flu in Week 9. Nevertheless, an overall improvement in confidence can be seen in the second half of the program in both speaking and singing, with moderate to higher median levels of confidence. A Wilcoxon signed-rank test confirmed that the self-reported confidence in the second four weeks was significantly higher than in the first four weeks, for both speaking (Z = −3.098, p < .002) and singing (Z = −2.994, p < .003).
Qualitative Data
Qualitative data from the questionnaires, interviews, and written reflections were analyzed as a single data set. Thematic coding led to identification of four main themes capturing participants’ reflections on participation in the workshops, which related to confidence, social aspects, the workshop approach, and the online/in-person format. The following abbreviations are used: FWn = Reflection Week (number), FQ = Final Questionnaire. Table 1 gives an overview of main themes and subthemes.
Structure of themes and subthemes.
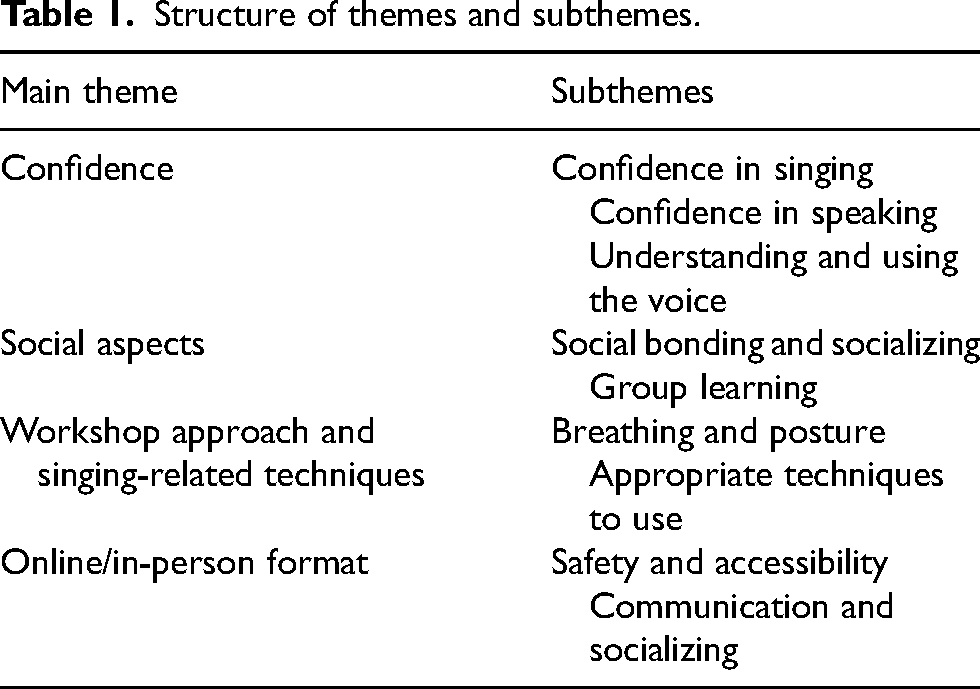
Theme 1: Confidence
The first theme relates to voice confidence in speaking and singing. During the pre-program interview, workshop leaders discussed improving confidence as a main aim, through the collaborative group nature of the workshops, and focusing on how singing together may increase voice confidence and control of the upper airway: I hope participants will feel more confident and optimistic about the future […] using music to […] feel better and to continue that increased control and confidence in the upper airway and voice box (SLT). It’ll help them to hear other people with a similar problem (VT).
During Week 6, a noticeable increase in confidence was observed through a rise in levels of vocalization, interaction, and engagement between participants. By Week 7, the SLT commented how impressed she was with progress being made, with participants’ voices sounding less restricted. By Week 9, participants were observed singing with others, including simple harmonizing and call and response exercises, in addition to using their voices individually. This was an encouraging development for the participants, supported by participant quotes from the written weekly reflections: My confidence is definitely improving with each session (RW8). The idea that I notice my voice more than other people has been helpful (RW5). Workshops gave me an understanding of my voice and ILO (FQ).
One participant in her final questionnaire response said the workshops had increased her confidence through socialization with others following the COVID-19 pandemic. [they have] given me more confidence not only in my voice but in my singing voice and in me personally […] without the workshops I would have remained separated at home after shielding (FQ).
This is similar to Judd and Pooley's (2014) findings, in which participants stated choir participation was beneficial during recovery from illness, supporting their confidence and helping them cope with life transitions.
RW responses revealed fluctuations in speaking and singing confidence, sometimes due to situational factors such as chemicals in the workplace or weather conditions triggering ILO symptoms: Fairly confident [with singing] since not working around chemicals (RW2). [Today] I’m not confident with speaking or singing. I was exposed to cleaning fluids at the hospital, so my throat is very sore (RW3). None of them wanted to attend in person because it was too hot, the pollen count was high, there was a lot of pollution in the air […] I think it's lovely to have this option of running an online session (VT, Post-program interview).
Skingley et al. (2014) previously found that participants with COPD stated that their condition had sometimes limited their ability to participate in a singing program. Nevertheless, as with the current study, Skingley's participants reported that they still felt that singing had improved their condition and boosted their confidence.
During the post-program interview, the SLT attributed the growth in confidence to the contact the workshops facilitated with other participants with ILO, thus emphasizing the importance of peer support: They’ve got an affinity with the other participants because most of them haven’t come across anybody else with the condition. That's been a really powerful undercurrent to help with the progression of confidence (SLT). Very quickly […] I think they felt an identity as a group, and I think that's helped with their confidence (SLT, Post-program interview).
These findings have commonalities with findings of previous studies of in-person group singing. Swain and Bodkin-Allen (2017) studied teachers lacking singing confidence and found choir participation to increase confidence, partly through discovering other people with similar experiences. As stated by Bonshor (2016), “social learning processes play an important part in acquiring confidence-building mastery experiences within group singing activities” (p. 300). The current study suggests that this is also possible in online singing group settings.
Participants reported that participation offered opportunities to gain a deeper understanding of their condition and to practice effective management strategies. They could take what they learned into their daily lives, providing a resource that they could rely on: The workshops helped remind me of the benefits of these techniques and to practice them and reap the benefits again (FQ).
The powerful quote below exemplifies the importance of receiving a correct and timely diagnosis and the impact of support from the singing workshops on the confidence of this participant: After a long time waiting to get a correct diagnosis, [the workshops] have been a life-changing experience (FQ).
Theme 2: Social Aspects
The social aspect of these online workshops relied on participants using their cameras and microphones. This interaction was especially important during exercises where participants were required to make sounds or sing together. During Week 7, all participants had microphones on and were singing loudly and confidently. The SLT noted this may be due to a “masking” effect of singing with others. The term “masking” is used to mean situations in which patients, or participants, can hear their voices but have the auditory support of other voices in the initial stages. It can help them establish a comfortable and consistent vocal posture. The SLT had found that patients or coaching clients with voice issues are often under-confident about listening to their own voices. The very act of listening in real time tends to affect the way they use their voice as it can lead to reduced resonance or increased constriction as the singer may be under-confident and want to refrain from being heard. The SLT had found that distraction techniques or producing sound simultaneously with the patient could be effective in helping them to improve support, projection, and resonance placement. That masking effect is a really powerful one, so you’re not the lone voice in a dark cave (SLT). Making noise together automatically builds community […] we coordinate our breathing, then our heart rates are kind of regulated and we synchronize our movements [building] a sense of community (VT).
This confirms that singing together online can be a powerful tool for increasing confidence and strengthening social bonds between individuals, in a similar way to participating in person (Bullack et al., 2018; Kreutz, 2014).
During Week 3, the VT introduced arm movements and clapping alongside the singing, which also seemed to add to a sense of group cohesion. Online participants were observed nodding, moving in synchrony, and making more noise together as they felt increasingly comfortable with each other. Complete synchrony could not be achieved due to being online and latency issues. Nevertheless, participants appeared to be moving together. This finding is similar to previous research on movement synchrony and social bonding in in-person settings, in which experiment results revealed that synchronous movement increased bonding between people (Tunçgenç & Cohen, 2016).
The online workshops enabled participants to experience the benefits of meeting and socializing with others with ILO. Participants mentioned how helpful it was to meet others and see everyone enjoying themselves, and collectively hearing improvements in the voices of people with similar conditions: [It is] great to be able to meet others with similar issues and backgrounds (RW2).
Participants in our online setting reported feeling comfortable in sharing the impacts of their illness with people with similar experiences within a supportive environment. This has been found in previous research in group singing in in-person settings (Andreou et al., 2022; Lord et al., 2012; McNaughton et al., 2016).
In the pre-program interview, the voice teacher had expressed his hope for workshops to be a space for encouragement of socializing: As well as the social mingling that we would like to encourage, I think there should be a sort of community. It's a community of learners (VT, Pre-program interview).
Once the online workshops began, the ILO patients were quickly observed to be relaxing and open to sharing their experiences with each other. This had strong similarities with the “ice-breaker effect” that Pearce et al. (2015) reported in in-person group singing activities.
Theme 3: Workshop Approach and Singing-Related Techniques
The workshops followed a regular structure. Each workshop began with a reminder about deep breathing and good posture, which could be applied when standing or in a seated position. Participants were often seated due to being online. The VT used postural and relaxation exercises to encourage a relaxed but poised position, allowing core support for the diaphragm and abdominal muscles. This was followed by breathing techniques, which participants reported as calming. When asked which techniques participants had used from previous workshops, those associated with breathing were mentioned regularly: Breathing from the stomach area and sitting more upright has been a life-changing experience (FQ). Understanding breathing techniques is calming (FQ). Techniques help me relax and focus into my breathing, especially in nervous situations (FQ).
These findings suggest that the online workshops had similar benefits to in-person group singing in terms of improving lung function, respiratory health, and breath control (McNaughton et al., 2016; Moss et al., 2018).
Some of the ILO patients in the current study reported reductions in chronic pain, which were attributed to the postural and breathing exercises: Enhanced knowledge of breathing and posture, not just for singing, helps with pain issues (FQ).
These findings about the online workshops reflect those by Hopper et al. (2016), who demonstrated that participating in a community choir helped people with chronic pain to self-manage symptoms. Joseph et al. (2022) also found that slow deep breathing, such as the exercises delivered during workshops in the current study, was associated with decreased pain.
During the workshops, singing techniques were introduced and practiced through a number of techniques including deep breathing; adopting an upright, poised but relaxed posture; encouraging resonance by humming; and using open vowels to reduce participants’ habitual focus on the voice box area, and to distract them from any problems they may be experiencing when speaking. During the pre-program interview, the SLT stated that nonsense words are sometimes used in therapy for distraction purposes. This idea was echoed in the VT's workshop delivery through the use of songs in different languages, or with nonsense syllables, which were gradually incorporated into sung and spoken words. Participants were able to focus on creating a clear tone by using open vowel sounds and resonant consonants rather than focusing too intently on more complex lyrics or spoken phrases.
During Week 6, the VT encouraged participants to gently touch their upper chest, lips, and cheeks while humming different notes so that they could feel resonance in their voices. Humming helped participants to experience different areas of sympathetic vibration, such as nasal or chest resonance. The importance of finding resonance was mentioned by several participants: Resonance and how to generate it has been very helpful to me in ‘resetting’ my speech when my throat gets sore (FQ). [It is] very useful to know where the sound comes from (RW2).
Participants also mentioned that practicing vowel sounds was important in their understanding of their voices and helped to maximize the resonating space in the vocal tract: Changing a vowel sound so it can be sung clearer [and] resonate where it should do (RW6).
A collaborative emergent approach was required for successful and considerate delivery of the workshops. The VT and SLT worked in response to the participants with ILO and were consistently mindful of participants’ needs to guide the direction and pace of the workshops. They were also aware and responsive to participants’ experiences of the workshops and of potential constraints of the ILO condition, encouraging them to indicate if they were unsure or uncomfortable about any technique or exercise. The VT provided a variety of approaches to boost engagement and confidence within the group. I’m used to working emergently as a teacher […] the rehearsal may take quite a different course to achieve a similar thing to what you or the group […] wants to achieve, […] you’re adapting all the time (VT). The singing was particularly enjoyed by participants, as demonstrated in these two powerful quotes: I enjoy the singing – I’ve never been told I CAN sing before (FQ) [I] wanted to race past the exercises to get to the singing (FQ)
The first quotation demonstrates that even people with ILO, who might perceive themselves as 2non-singers,” can benefit from using singing and singing-related techniques in group sessions. In earlier studies, benefits were observed in a broader context, with self-reported “non-singers” in the general population finding that group singing can be cathartic and emotionally uplifting (Richards & Durrant, 2003; Warran et al., 2019). However, studies involving participants with ILO have not previously been carried out, and the current study has promising implications for developing singing-related interventions for this population.
Theme 4: Online/In-Person
During the COVID-19 pandemic, technology was a lifeline for making musical and social connections between people (Pennill & Timmers, 2021). Technology allowed people to connect at a time when in-person gatherings were not possible, even though using online platforms do create barriers for those who are less technologically literate. Online provision was especially important in the singing world, as singing together was restricted for a considerable length of time. However, there were issues with latency when singing together online, along with internet connectivity problems, which can limit the enjoyment and satisfaction derived from group singing (Daffern et al., 2021). One issue with latency is the inability to be able to sing together in synchrony (Price et al., 2021). The VT used singing in rounds using free-flowing pentatonic exercises that sounded effective despite the latency, and call and response to ensure voices could be heard separately.
During the pre-program interview, the VT and SLT expressed concerns about the limitations of online delivery and possible lack of opportunity to socialize and hear each other singing. Responses from the post-program questionnaire indeed revealed that participants found it difficult to socialize with others online: They’re not going to get that physical feeling, because it's always a physical feeling when the sound is resonating around you (VT, Post-program interview). [I] wanted to socialize more with participants but [it was] difficult as most workshops were virtual (FQ).
During Week 9, participants expressed how much they were looking forward to the in-person workshop (Week 10): It’ll be so nice to meet people with the same condition face to face (O9).
Practical issues were raised, such as online workshops being difficult for those who are hard of hearing, problems with connection, and the inability of voices to be heard together via Microsoft Teams: I am deaf and rely on facial cues which are difficult to interpret on a screen (FQ). Struggling with connection was frustrating! (RW3)
Observed problems included reliance on having microphones on so voices could be heard and making sure participants felt confident enough to do so. Microsoft Teams separates a single voice from others, inhibiting the ability to hear everyone singing together. After a few weeks, the VT introduced call-and-response singing activities, and participants were almost immediately able to join in (and appeared to be very comfortable) with these, despite the drawbacks of being online. Singing simple harmonies was also practiced using notes from a pentatonic scale, which created consonant chords that were not adversely affected by the latency.
Benefits of online workshops can include increased accessibility for those with ILO and other physical conditions. For example, an online or hybrid model removes barriers and stresses that can accompany travel to in-person workshops. Online delivery also means that COVID-19, and other illnesses that can especially affect those with ILO, cannot be transmitted: We don’t have to worry about transmitting the disease (SLT, Pre-program interview).
Pitt et al. (2018) similarly found online group aphasia therapy conducted by speech and language pathologists to be accessible and flexible, allowing wider and/or more frequent participation. Although in-person workshops have some advantages, it is suggested that the online format, as used in the current study, has the potential to widen accessibility and provide valuable support.
Therefore, delivering and taking part in online workshops, in collaborations between VTs and SLTs, can be considered as safe and practical for both workshop leaders and participants in terms of accessibility, convenience, reduced transmission of illnesses, and the benefits of being able to participate in a familiar, home environment. However, as there are also many benefits of in-person singing workshops, such as opportunities for socializing and hearing voices together in real time, it could be suggested that a hybrid or alternate delivery of in-person and online singing workshops provides better opportunities for access and allows participants the option of engaging in the most appropriate way for them.
In the interests of equality and inclusivity, the existence of a digital divide between some demographic groups should be acknowledged. Accessibility to online sessions can be limited by availability of the necessary technology. For complete equity of access, avenues for providing technology support should be explored to ensure that digital inequality does not preclude participation.
Discussion
This research provides support for the use of singing-related technique workshops with people with inducible laryngeal obstruction (ILO) to improve confidence in speaking and singing; provide opportunities for social bonding with others with the condition; and learn strategies for self-management of the condition, such as breathing techniques and exploring vocal resonance. An increase in confidence was observed through quantitative analysis of Likert-scale measures, supported by qualitative data from reflections by the participants with ILO and workshop leaders, and workshop observations.
While the research indicates the use of singing to be feasible for people with ILO, it is of the utmost importance that workshop leaders are considerate, adaptable, and flexible in their approach to conducting workshops, to allow participants to feel comfortable and able to engage. Each participant was different with respect to the severity of their condition and how it manifested throughout the program of workshops. ILO participants noted that, while their condition sometimes prevented them from fully participating in workshops, overall the breathing and singing techniques were enjoyable. The exercises, activities, and interactions helped them feel calmer and more confident while speaking, and some participants reported enjoying the singing more than they expected.
This research provides important insights into a participant-focused approach to facilitating workshops and could be used to guide similar workshops in the future. It also highlights the potential for constructive collaboration between voice teachers, speech and language therapists, and other clinicians when devising support programs for patients with respiratory conditions that affect voice production, vocal confidence, and social engagement.
Limitations
This study was conducted with a small number of female participants receiving speech and language therapy within the Sheffield Teaching Hospitals. There was some variation in ethnicity in the participant group, but no gender variation. There were a range of different levels of disability, either due to ILO or other health conditions. Replications with a larger group of participants and different workshop approaches are required for the findings to be generalizable. As ILO comprises a complex set of symptoms, it can be misunderstood or misdiagnosed as other conditions. This means there was a relatively small pool of patients from which to recruit research participants, which affected the sample size in this study. The scarcity of available online ILO resources may be contributing to the lack of general awareness or knowledge of ILO and to the sense of isolation amongst those with the condition.
Workshops had to take an online approach, except for the final workshop, to maintain safety for those with respiratory conditions against the backdrop of the COVID-19 pandemic. COVID-19 and other illnesses unfortunately affected attendance of participants during the program of workshops, which may have negatively influenced the progression of confidence and control of the condition, although this was not explored in detail. While ever-changing restrictions necessitated adaptability in workshop delivery, there were accessibility benefits to the flexibility provided by this online approach.
Characteristics of the Workshops
Despite the small sample size, we see it as important to learn from this feasibility trial to promote awareness of ILO as a condition and to showcase opportunities for ILO patients to engage in workshops (online or in-person) that employ singing and singing-related techniques. Participants were not expecting to be able to sing, and their self-reported singing confidence ratings were low at the beginning of the program. However, all attendees participated and became involved in the singing, and reported improvements in their confidence generally as well in using their voices for speaking and singing.
There are several characteristics that are likely to have contributed to the success of the workshops, not all of which were explicitly mentioned by the participants. The first author (main researcher acting as observer) and audio-visual technician joined in the singing and so supported the sonic outcome. Participants were able to join in the exercises, take a break, or withdraw from the program if necessary. During the 10 workshops, participants built up a repertoire of techniques and songs, and online resources were provided as reminders of technical points and lyrics. Recordings were made, which were later developed into a sonic arts piece. This was published online and presented at a public engagement festival that also featured an explanation of the condition of ILO and an illustration of the workshop techniques. 1 This gave participants an opportunity (in the presence of an audience) to hear the immersive soundscape consisting of exercises, songs, and sounds they made during workshops, and to appreciate that they were part of a creative legacy from the project. This gave a goal to the workshops, although most participants seemed to join the workshops principally for the purpose of working with their voice and coping with their ILO symptoms.
The workshops offered a predictable structure that developed over the weeks. Posture, breathing, and body-relaxation exercises while standing or sitting were followed by working on sounds and later songs. The workshops had a light atmosphere, and there was enough time for social chat. The duration of the workshops was restricted to one hour to limit fatigue.
Recommendations for Future Workshops and Research
This research showed that participating in group workshops employing singing and singing-related techniques can offer benefits for people with ILO. These techniques can enhance what individual speech and language therapy can offer, even when delivered through an online format. Confidence was developed by participating in these workshops with other people with the condition and by trying out different techniques in a relaxed and enjoyable environment, where the focus was away from the individual. Participants could take what they learned into their daily lives, providing a resource that they could rely on.
This research contributes to a growing body of evidence of feasible and effective applications of group singing for clinical populations, and their potential for positive outcomes (Lord et al., 2012; Skingley et al., 2014). We deliberately chose to refer to the activities as “singing-related” to refer to the broad spectrum of techniques associated with the program, including focus on posture, breathing, and relaxation of the face and body; simple synchronized movements and stretches; hums and open vowel sounds; and learning of songs. This approach differentiates this study from research involving established choirs, where there is usually a strong focus on musical repertoire and public performance. This study shows parallels with, for example, the Singing for Lung Health (SLH) project, where new singing groups are established with a specific therapeutic focus, rather than existing choirs being used (Lewis et al., 2018). However, SLH focuses on people with COPD rather than ILO.
Future research with ILO participants is needed to further demonstrate the beneficial outcomes of participation in singing-related technique workshops with a larger and more diverse sample, for example, to explore whether there are any gender- or age-related differences that may affect the outcomes. Further research could trace voice developments individually and measure outcomes within and outside the workshops. Protocols for workshops may be precisely set to facilitate replicability, including setting ground rules such as in the current study through use of a culture document. The influence workshop participation has on other areas of the lives of those with ILO could be explored, such as the effect on length and duration of speech and language therapy required. This may have important implications for health services, as a reduction in the time required for therapy may result in a less overwhelming demand for therapy services, thus reducing wait times and financial strain on resources. Speech and language therapists may benefit from collaborating with an experienced voice teacher to allow them to facilitate singing sessions for patients on a waiting list.
Future applications of singing-related techniques for people with ILO may take the form of participation in specialist online workshops, such as was the case in our study. Alternatively, speech and language therapists and other clinicians may wish to explore integrating group singing therapy into their practices in collaboration with a voice teacher, as mentioned above. However, some clinicians may not be comfortable with this, depending on individual preferences and preferred working practices. Furthermore, community choirs and singing groups that focus on healthy voice production may create a space where patients with a range of respiratory conditions use their voice with confidence and enjoyment. It is strongly recommended that choir leaders work with SLTs to develop effective approaches for helping all singers, and particularly singers with respiratory conditions, to use their voices healthily.
Conclusion
In summary, this research provided evidence for the feasibility of the use of singing-related techniques to increase confidence in speaking and singing for people with ILO. This condition can have a severely negative impact on patients’ lives, as it affects the ability to communicate verbally in everyday situations and can affect social interaction and employment prospects. Alongside increasing voice confidence, the workshops were successful in creating better awareness and understanding of use of the voice, and the techniques learned could function as a resource to be used outside the workshops. The workshops created a group context and supportive online environment where people with ILO could participate with others in creative and enjoyable uses of their voices, practicing supportive singing-related techniques. They had opportunities to explore new avenues, including vocalizing different sounds, at different pitches, with varying intensities and rhythmic patterns, in an empathic group setting. This was experienced as empowering to the extent that some reported it to be “life changing.”
Footnotes
Acknowledgements
We are very grateful to the following funders: Sheffield Hospitals Charity, Arts Council England, Festival of the Mind, University of Sheffield. This work was supported by the Arts & Humanities Research Council (grant number AH/R012733/1) through the White Rose College of the Arts & Humanities.
Action Editor
Graham Welch, University College London, Institute of Education.
Peer Review
Gillyanne Kayes, Vocal Process. John Nix, University of Texas at San Antonio, School of Music.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This project was granted ethical approval by the Department of Music of the University of Sheffield.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Arts & Humanities Research Council (grant number AH/R012733/1) through the White Rose College of the Arts & Humanities.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.