
Abstract
Saxophonists experience a high rate of performance-related injuries and wellbeing concerns, with limited research on player perspectives and lived experience to inform preventive or interventional methods. To address this gap, a cohort study was conducted with 14 saxophonists from around Australia, to gather perspectives and experiences on playing-related pain, injury, health, and wellbeing. A baseline survey and semi-structured interviews were used to gather a range of qualitative and quantitative data to provide a holistic overview of the cohort and their lived experience. Results indicated that the lifetime prevalence of a performance-related musculoskeletal disorder (PRMD) for saxophonists in this cohort was 64%, with a point prevalence of 15%. Performance-related pain or injury was prevalent in the following locations: hands, wrists, forearms, back, shoulders, and embouchure, as is consistent with comparable studies. Prominent themes were identified from qualitative data that covered participants’ lived experience and perspectives of injuries and pain, performance anxiety, and education. This included sub-themes of accessing recovery, physical conditioning, health literacy, and education for music teachers, occupational concerns, health education during tertiary study, and accessing healthcare. Future research that explores the efficacy of methods for health promotion, performance anxiety, injury prevention, and saxophone performance may be useful in addressing concerns and improving the health and wellbeing of saxophonists.
Introduction
Supporting performance health and wellbeing is essential to safeguard the sustainability of musicians’ careers. The lifetime prevalence of PRMDs has been reported up to 93% for musicians (Kok et al., 2016) and 76% for saxophonists (Shanoff et al., 2019). Several performance-related musculoskeletal disorders (PRMDs), associated risk factors, prevalence, and management options have been identified in musicians (Ajidahun et al., 2019; Kok et al., 2016; Rodríguez-Gude et al., 2023). However, there have been very few studies examining this area specifically for saxophonists.
Some studies have investigated orofacial problems (OFP) and pain in saxophonists (Clemente et al., 2023), wind, and brass instrumentalists (Leonardi et al., 2020; Lesjak et al., 2024). Interestingly, Lesjak et al. (2024) found small differences between motor imagery and body perception in the orofacial region between those with OFP and without. Shanoff et al. (2019) explored PRMDs and postural complaints among saxophonists, with top pain locations including the wrist, neck, mouth, and jaw, identifying a correlation between postural habits and playing-related pain. In a pilot study on the influence of neckstraps and carrying devices on the spine, Piatek et al. (2018) found several differences that affect body positioning. An interesting study by Moura and Serra (2024) explored saxophonists’ perceptions of body movement with findings on its impact on performance quality and musical aspects, influencing factors on movement, and how it is used in practice and pedagogy. Their paper also touches on health literacy concerns, an absence of scientific and biomechanical instruction in music pedagogy and the need to reform aspects of tertiary music curricula. Further research is required to investigate practical strategies for supporting saxophonists’ health, wellbeing, and injury prevention. This could include interventions within training institutions and professional networks to offer impactful and sustainable methods of addressing their performance health.
Professional musicians experience injury risks similar to elite athletes (Ajidahun et al., 2019; Mastnak, 2017; Schoeb & Zosso, 2012). Effective management of risk factors may lead to both the prevention of the onset and recurrence of PRMDs (Ackermann et al., 2011; Watson, 2009). Risk factors and perceived causative factors for physical injuries can include; age and gender, playing load, insufficient warm-up and sudden increase in playing time, repetition, stress and insufficient recovery, poor technique, posture and/or technical considerations, low mood and perfectionism, instrument ergonomics/weight, muscle fatigue/tension, and a lack of health awareness (Ackermann et al., 2012; Ajidahun et al., 2019; Lee et al., 2012; Rodríguez-Gude et al., 2023). In addition, the prevalence of musicians’ performance anxiety (MPA) is high, with up to 70% experiencing MPA to a moderate level and between 15–25% to a severe level (Osborne et al., 2020; Stern et al., 2012; Studer et al., 2014; Yoshie et al., 2008). The impact of MPA can be debilitating, including somatic and cognitive symptoms that affect performative skills, outcome quality, and psychological wellbeing (Kenny et al., 2014; Osborne et al., 2020; Stern et al., 2012). Some have suggested that anxiety and perfectionism are attributed to MPA (Kenny et al., 2014) and that this may increase the risk in developing a PRMD (Yoshie et al., 2008) or focal dystonia in musicians (Altenmuller & Jabusch, 2009). There is need for further research into pragmatic approaches which can holistically address both the physical and psychological demands of saxophone playing.
To address this need and contribute much-needed research in this area from a performer’s perspective, this cohort study focuses on moderate to highly experienced saxophonists’ perspectives, experiences, and wellbeing, particularly in relation to understanding performance-related pain, injuries, and challenges. This approach draws from phenomenological inquiry such as is outlined in van Manen (1997). Research on the lived experience of participants may provide a depth of understanding and insight outside of theoretical knowledge or solely quantitative means and may be particularly useful in pedagogical research (van Manen, 1997). By capturing qualitative and quantitative data, the results from this study are intended to inform, contextualize, and provide direction for future research, where practical methods may be applied and evaluated for potential supportive effects on performance, health, and wellbeing.
Methodology
Fourteen participants from Australia who met the following criteria were involved in the cohort study: age ≥ 18 years old; graduate or current university saxophone students, performers, and/or educators; and currently had a self-identified regular practice routine. Participants were representative of moderate to highly experienced saxophone players.
Qualitative and quantitative methods were used to capture a broad range of data from this cohort. As has been done in similar studies with musicians (Guptill, 2011; Schoeb & Zosso, 2012), phenomenological inquiry through semi-structured interviews was used, with many questions focused on participants’ current difficulties, their perspectives, and their lived experience of performance-related pain. Qualitative data relating to injury prevalence, practice load, and demographical information was captured through a baseline survey, a method similarly used in other studies on musicians’ wellbeing (Ackermann et al., 2011; Kenny et al., 2014) and saxophone-specific investigations (Shanoff, 2020; Shanoff et al., 2019). Ethics approval was granted by Edith Cowan University's Research Ethics Committee, approval number 2021-02576-DEMANDOLX. Participants were recruited through the authors’ professional musical networks, via email to tertiary music institutions, and via social media. All participants were provided with a participant information letter and completed an informed consent form prior to participation.
Interviews
Semi-structured interviews were 30–60 min in duration depending on participant responses. Open-ended questions were centered on participants’ experiences and perceptions of saxophone practice, performance, pain or injury, stress, and health and wellbeing. The interviews were audio-recorded and transcribed using Microsoft Teams, Microsoft Word, and an iPhone application “Voice Memos”. All interviews were checked and edited by the lead author to ensure the transcript matched the audio recording.
Survey
Participants completed a 37-item survey designed to capture injury and pain history and experiences, demographic information, and saxophone-specific data. The development of the survey was based on the following questions from Ackermann and Driscoll (2010) (1, 7–10, 18, 20, 21, 23, 24, 26–34), which covered themes of physical activity, injury and pain history, and playing load. Items omitted were considered irrelevant to the study aims, with additional inclusions for the purposes of the study.
Data Analyses
Reflexive thematic analysis (Braun & Clarke, 2022) was used to identify key themes from the interviews and survey. NVivo 12 Plus (Lumivero, Denver, USA) was used to code, generate, and review themes. The lead researcher (ND) coded the data, using the process outlined in Braun and Clarke (2022) through the lens of critical realism and the research team reviewed the codes (JN, MS, LH) consistent with the critical friends approach (Smith, 2018). This was selected due to its suitability for the research which was based in understanding lived experiences and perceptions of wellbeing in saxophonists, potential contributors to injury or pain and representing participants’ “realities” including any perceived causations which may guide future research pathways. This was a six-step approach, through which there was familiarization with the data, initial generation of codes which were data-led (repeated several times), generation of themes, refining and developing codes and themes, then defining and placing the themes within their overarching concept, to be formally written in the final phase. Qualtrics and Microsoft Excel were used in analyzing quantitative baseline survey data.
Results
The following results are representative of the moderate to highly experienced tertiary saxophone student or educator-performer, with a classically trained background. They provide a snapshot of this cohorts’ perspectives and experiences. This first section includes the results from the questionnaire data, separated into four sections: demographics, saxophone-specific statistics, past history, and perceived contributors. The second section will explore the themes identified within the interview data.
Questionnaires
Demographics
Demographic data for the cohort participants are presented in Table 1, describing cohort statistics such as age, occupation, and injury prevalence.
Cohort descriptive statistics.

Saxophone-Specific Statistics
Saxophone-specific statistics from the cohort are presented in Table 2. It is important to note that the survey was conducted at the beginning of the university semester, where the playing load may be lighter than during a recital or exam season.
Saxophone-specific statistics.
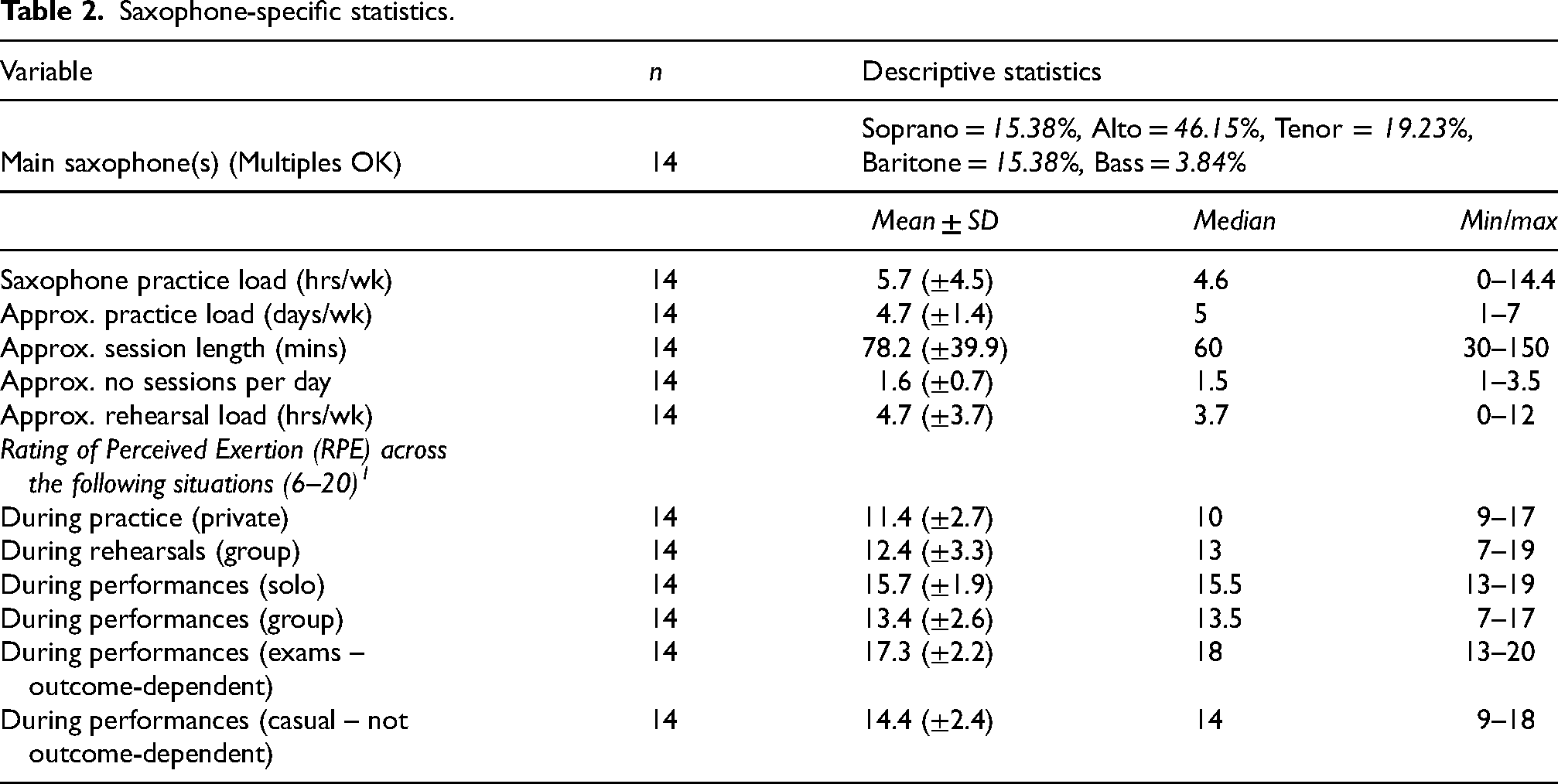
Participants used a variety of carrying systems, utilizing options such as harnesses or neckstraps. As this supports the weight of the saxophone, it can be an important consideration when looking at playing-related injury or pain. In this cohort, 61.5% used a carrying-system where the weight is re-distributed away from the neck or is specifically designed with neck/upper body pain in mind, such as the “Jazzlab,” “Breathtaking,” or “Cebulla” neckstraps. A standard neckstrap was used by 38.5% of participants.
Past Performance-Related Injuries and Pain
The lifetime prevalence of a PRMD in this cohort of saxophonists was 64.3%, with a point prevalence of 15.3%. Hands, wrists, and forearms were the most frequent injury location, followed by back, shoulder, and embouchure.

Lifetime prevalence of injury.
Participants were asked to describe performance-related pain and how it felt when they were experiencing it. They used the following words: stabbing, tightness/tension, burning, aching, stiffness, fatigue, tender, pain, cramping, pulling, discomfort, shooting, and knots.
The following health professionals had been consulted, with participants saying they had mixed results on efficacy and relief. For previous performance-related complaints: massage therapist (n = 1), acupuncturist (n = 1), and a physiotherapist (n = 6) were seen. For current performance-related complaints, a doctor (n = 1), physiotherapist (n = 3), and massage therapist (n = 2) were consulted.
Contributors to PRMD Incidence, Perceived Stressors, and Experiences
Participants perceived overload in practice hours, mental and physical fatigue, stress, muscle tension, and sudden increase in load to be the top contributors to a PRMD.
In addition, participants were asked to identify their physical and psychological stressors about playing the saxophone. Across the cohort, it was perceived that the top three physical stressors for saxophonists are muscle fatigue, muscle tension, and repertoire demands. Performance anxiety, performing, and repertoire preparation were the top three mental stressors. For a full list of answers, please see Figures 2 and 3 below.
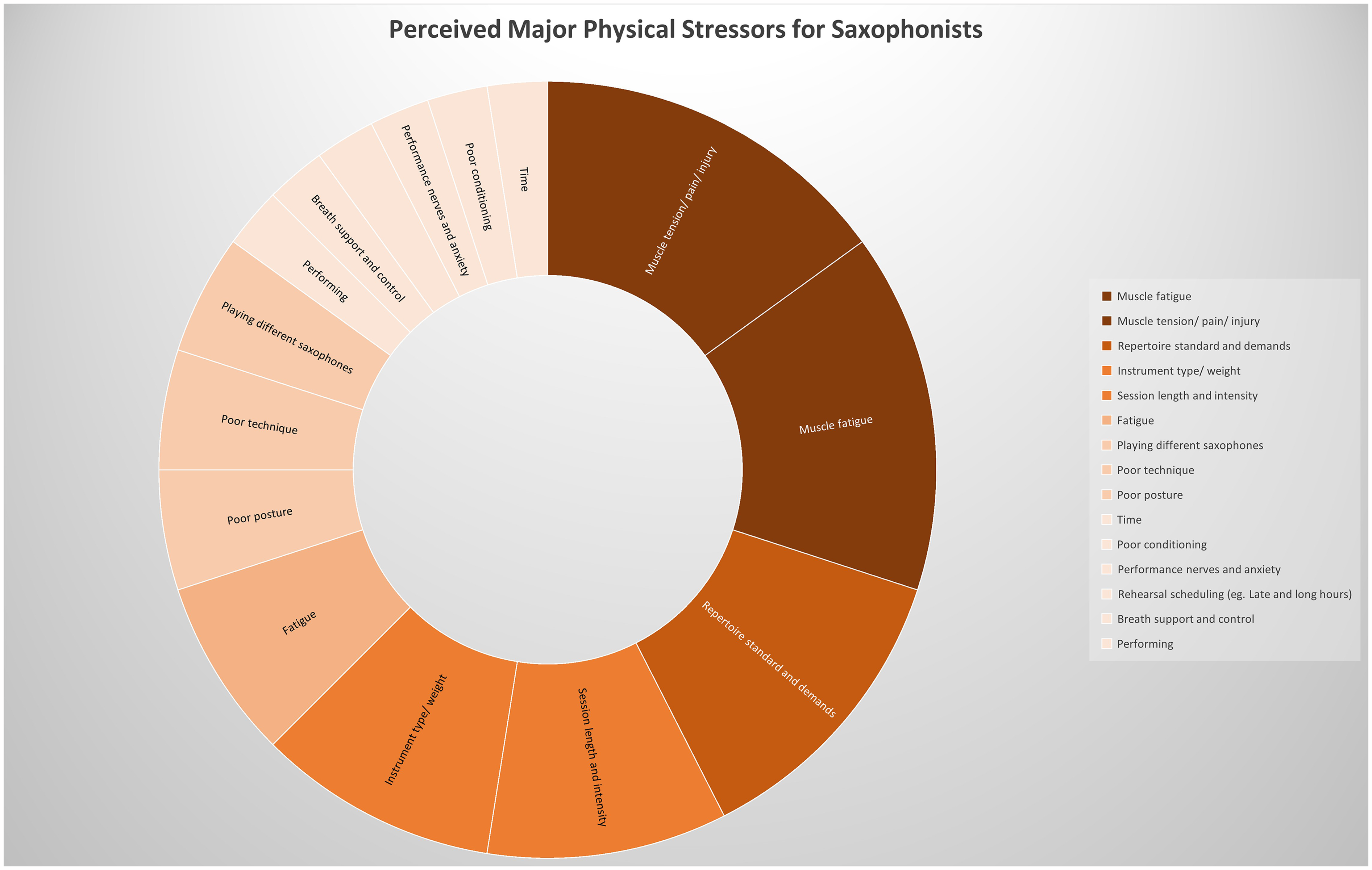
Perceived major physical stressors for saxophonists.

Perceived major psychological stressors for saxophonists.
Interview Data
This second section includes the two main themes identified from the interview data. The first theme is experiences of performance-related pain and performance anxiety. The second theme is participants’ perspectives on health, wellbeing, and affecting change. Sub-themes include prohibitive factors to accessing recovery, occupational concerns, physical conditioning, health literacy and education for music teachers, health education during tertiary study, and accessing healthcare.
Theme 1: Experiences of Performance-Related Pain and Performance Anxiety
Participants who had been injured or experienced playing-related pain had important insights into the mental, physical, occupational, and social impacts that have arisen from their experiences. Often, they were aware of personal contributing factors to their previous injuries such as practice intensity or overload: “(P11) I don’t have pain right now, but I definitely had that wrist problem last year. I know as soon as the intensity picks up, I know it’ll probably come back.” This information is valuable in understanding the phenomenon of playing-related injuries, including how participants respond to symptoms and feel about PRMDs.
Those with previous PRMDs or performance-related injuries expressed that this led to feelings of uncertainty, anxiety, self-doubt, stress, and/or re-injury concerns. These responses can occur amidst a performance, when a PRMD or injury recurs, as in one participants’ account: “(J10) I was like oh my gosh, am I going to get through this? Am I going to get through this? And then, yeah, it [recurrence] happened.”
Lived experience indicated that stress related to performing, and musician's performance anxiety (MPA) was perceived to contribute to lower levels of saxophonists’ wellbeing. Participants had a variety of somatic and psychosomatic MPA symptoms that they said often affected their performance or wellbeing. These were described as stress, negative self-talk, increased heart rate, shaking, sweating, difficulty with breath control, feeling unprepared, post-performance rumination, difficulty concentrating, generally feeling ill or fatigued, and a loss of trust in the control of one's own body. One participant described it as “(F15) I feel sick and I shake and I just can’t concentrate.” Sometimes the cognitive experience did not always match the somatic symptoms, for example, body shakes when the participant did not perceive they were nervous: “(L7) Walking on stage, I’m calm, but I will have the physical symptoms of being stressed. So my heart rate will be up. Usually my hands are a bit sweaty. Often my breathing's a little shallower or faster…but my mental state is quite calm.” Interestingly, although participants could often identify symptoms and potential causative factors to MPA and PRMDs, there were few participants that had any management strategies to counteract the symptomatic impacts on performance.
Participants identified a few things that increased their performance anxiety, such as peer judgment, outcome dependency, solo performances (much more than group), past negative experiences, and not knowing how to deal with the performance anxiety and associated symptoms. When asked if there were any areas they would like to see improvements, many expressed a desire to know about dealing with performance anxiety and managing symptoms: “(H2) Maybe just like nerves up to a performance and stopping that having an effect on the physicality of performance…I think maybe if I make a mistake and sort of not letting that ruin the performance.”
Theme 2: Perspectives from Within the Saxophone Community on Health, Wellbeing, and Affecting Change
When discussing general attitudes to performing arts health, participants perceived that performance health and wellbeing needs were often dismissed or not a priority until someone becomes injured, and even then, there can be an attitude of suffering in silence, not knowing who to turn to for help: “(K13) I don’t know if everyone just doesn’t talk about it and is suffering in silence or because there's an expectation of oh, well, just get on with it. So this is your life.”
Others were used to playing-related pain, with minimal relief or recurrent pain that had not yet been fully managed: “(L7) I kind of always have constant aches and pains because of the saxophone. So I want to try and make that not just something I have to live with and actually deal with them.”
In addition to physical components of performance health, participants identified mental health aspects such as negative self-talk or comparisons to others, as elements of wellbeing they wanted to improve: “(P11) Definitely negative self-talk, yeah, that's definitely me. Comparing myself to others, that's probably my biggest issue. I’m always thinking, where do I sit from previous years? Where was [name]…am I the same level as him?” Another's experience is similar: “(L7) I think I have a lot of negative self-talk…it doesn’t help when it then manifests into my music. Cause that’s the part that I should or would like to not hate on.” Others describe negative self-talk as a response when changing to less familiar saxophones: “(D3) Yeah, I think I have a lot of negative self-talk…especially when switching saxophone size, I’m just kind of not believing that the sounds would come out.”
These responses indicate that negative self-talk is a concern for participants, potentially impacting aspects of their practice and self-perception.
Prohibitive Factors to Accessing Recovery
Throughout the responses, it appeared that recovery was not an active component of these saxophonists’ practice routines. The cost of accessing resources, yoga classes, healthcare providers, or other forms of recovery was identified as a prohibitive factor in recovery accessibility. One participant describes that whilst being a student, associated costs may prevent their involvement in a recovery activity they would otherwise be interested in participating: “(J10) I’m excited to actually start doing yoga…I don’t have the money to do that as a student.” Education was another important factor. One participant describes the difficulty of applying injury prevention knowledge, when they received infrequent or ill-fitting instruction during university: “(K13) apart from possibly small little workshops in that workshop week, it will be stuff like the Alexander technique and one session, geared entirely towards string players and everyone else just had to sit there…cool, how can I round about apply this to my own [playing] without any kind of instruction?”
Occupational Concerns
A prominent occupational demand of concern to participants was the need to “double” on other woodwinds other than saxophone. Among saxophonists, it is common practice that one be proficient enough to teach and/or perform on clarinet and flute for example, and for those in musicals, one might also be required play double reeds (oboe and bassoon). The primary concerns were about preventing playing-related pain from the doubling instruments (pain that did not occur when playing the saxophone) and maintaining skill level across all “doubled” instruments, while still maintaining a sense of balance in their practice routine. Concerns centered on the need for additional resources on posture, technique, and switching quickly between instruments (sometimes just within a few beats), and how this might be incorporated into a practice routine. (A9) I know from experience, especially when you’re the low reed doubler, it's pretty taxing on the body when you play in musicals where you have fast changes from all three [instruments]…maybe more exercises that could help that, and then I dunno about embouchure, but maybe more in your physicality and stuff, just for anyone who doubles I think that would be useful.
Physical Conditioning
Participants who had a role as a music teacher expressed concern for their students and the need for physical conditioning education for musicians: (K13) I think everybody needs awareness of that it is a physical activity that needs health in your body and body conditioning…they do strength and conditioning training for their sport without a second thought about it…they think it goes together because it's sport but they don’t think of music that way…the whole thing is physical.
Participants regularly mentioned physical conditioning, often using the terms “endurance,” “fatigue,” and “strength” to describe areas they wanted to improve in their saxophone playing: “(Z6) I’ve had a lot of trouble with my embouchure and just having a lot of strength there and I think that is something that I would like to have more consistent practice with is just strengthening those muscles.” “Playing fitness” seemed to be predominantly about improving technique and sound quality rather than injury or pain concerns.
Health Literacy and Education for Music Teachers
Participants offered clear perspectives about education for music teachers, in order to prevent harmful or incorrect advice, and to embed performance health instruction that is sufficient for instrumental tutoring and risk mitigation. This was considered important for several reasons. In the past, participants had received incorrect advice, teachers and peers were the first point of call when performance pain arose so there was an element of responsibility, and for those considering moving into education, it was important to them to upskill in this area for their students’ wellbeing.
Music students and educators had the following to say about upskilling: “(J10) I feel like I definitely need to upskill,” “Yeah, I definitely need to know the injuries that are brought on by playing the saxophone. I never knew that just from something so tiny can spread so far if you leave it untreated,” and “(R16) I think its really important to know more…so I can tell my students, that way they don’t get injuries or things like that because they might not have as much of a body awareness as we might have.”
Some had received well-intended advice that changed their habits, but that may not have been correct or informed: “(F15) scoliosis…it's the big one that I’ve been hounded with since I’ve started playing which is why I practice [with my saxophone positioned] in the middle now, instead of to the side because my teacher was always like ‘you’re going to get scoliosis!’”
Health Education During Tertiary Study
All participants were currently or previously studying a music or music education degree at university and had some important insights regarding preparation for a career as a musician, and significant knowledge gaps that could be better attended.
One participant describes how tertiary students arrive from different life experiences, and there are invisible expectations that are harmful or limiting: (K13) There was some weird expectation of you arrive at uni[versity] and you don’t need all of this. Especially now being a music teacher you see how different [education experiences] are …I teach at private schools…lots more resources and in cities, there's lots more resources. If you’re coming from elsewhere in Australia from some little country town that had…one saxophone in the band…that's where I came from in primary school…my teacher wasn’t the saxophone player…you get to uni and they think you magically know this stuff. So I think it's really important to put classes in or have resources for people to actually be able to learn and implement it into their lives and education.
Others described that tertiary institutions do not provide enough applicable knowledge or practical strategies to address performance health and wellbeing and saw this as vital for their development as a well-rounded musician and by extension, should be a part of tertiary training for musicians. With seemingly limited efforts to incorporate performing arts health instruction, perhaps complicated by timetable availability some said it tended to be offered inconsistently at points throughout the year, and was therefore less impactful and less of a priority. Others relied on seeking information out when they needed it, but they felt current health education could be embedded into the tertiary curriculum more effectively: (D3) It wasn’t the most effective way to learn, I think. I think very casually, our lecturers and tutors will mention things during workshops. And I have approached mentors and stuff too, little problems I’ve had…there probably could be more…I think more practical ways to apply, to build it into your practice so that the knowledge can be transferred to actual practice.
Another said: (J10) we have on a Friday, two classes dedicated to JUST listening to people perform and there could easily be a class slotted in that's about fitness and mental strength and what it is to be a performer, you know like the lifestyle that you have to maintain being a performer.
Results directly from lived experience in Australian tertiary institutions indicate that there is a need to improve how we equip students with the knowledge and practical skills to be able to have autonomy over their performance health.
Accessing Healthcare
Knowing where to access healthcare was a concern for some saxophonists. Provider attitudes, specialized knowledge, and understanding were all considered to be factors in participants’ decisions to seek help. Many responses reflected a tendency for these healthcare providers to deal specifically with symptoms such as muscle tension or pain, with none describing any proactive solutions such as adjustments to practice habits or their saxophone playing. There was some distrust over the lack of specialized musical knowledge and understanding that had been experienced when participants sought help for performance-related pain: (L7) People in these sorts of professions need to be aware that musicians do get injured and that that's a common thing. That is something they need to be aware of if they want to treat musicians and they need to actually have an understanding of how that happens because we are less likely to go and seek help if people don’t know how to help us.
Discussion
This cohort study represents some of the experiences and perceptions of moderate to highly experienced, tertiary and early-career saxophonists from within Australia. There is minimal research on the perspectives and experiences of saxophonists on health, wellbeing, and performance. The results from this cohort study begin to address this gap, and provide insight and access to student, performer, and educator perspectives, a valuable component in responding appropriately to their concerns, as saxophonists, for saxophonists.
In looking at PRMD incidence, and pain locations, the results from this cohort are similar to comparable studies on saxophonists from North America (Shanoff et al., 2019). Given the small sample size (n = 14) and sample characteristics (mostly educators and students), it may be beneficial for a larger cohort study to be conducted, similar to those in other countries, where full-time performer and expert Australian saxophonists are represented. This may allow for a more robust overview of saxophonists’ experiences and contribute to the current transnational research on musicians’ health and wellbeing.
The lifetime prevalence rate of 64.3% may be cause for concern, considering that the participants’ playing experience are only a mean of 10.57 ± 4.2 years, and it could be reasonably ascertained that over their career, they may expect to play for another 30 years or more. High occupational injury rates so early in a career may indicate a need for further research in investigating sustainability in performance and teaching careers. However, caution is needed when interpreting these results, as there was some inconsistency among practice habits and little evidence of health-conscious practice routines, such as implementing warm-ups, and therefore these rates may be inflated due to other factors. One avenue for consideration within sustainability and wellbeing may be to research interventional and preventive methods for saxophonists to reduce PRMDs. Several impactful studies have involved the use of exercise prescription, yoga, or other methods in reducing musicians’ injuries and improving health outcomes (Ackermann et al., 2002, 2014; Butzer et al., 2016; Chan et al., 2013), but many of these have focused on orchestral musicians or have had limited involvement with saxophonists. Further research exploring practical methods for saxophonists to improve performance health and wellbeing may be useful in addressing risk factors while working in tandem with the existing performance pedagogy and tradition.
Some of the participants were concerned about negative attitudes towards performance injuries having led to a “suffering in silence” in the past, as well as a lack of general awareness of injury management or prevention, which may deter the timely intervention of recovery methods. Recovery is a well-known component to encouraging wellbeing and improving health, with a growing body of research in the performing arts and sports exploring the integration of recovery in existing high-performance disciplines (Blevins et al., 2021; Kellmann, 2010). Methods such as periodization use recovery to offset load and symptoms associated with overload and overuse (Wyon & Allard, 2022). Insufficient recovery is often considered a risk factor for PRMDs (Wu, 2007), therefore evaluating current barriers, tools, and efficacy is a natural next step in improving health and wellbeing for saxophonists.
Participants identified significant barriers to the access and implementation of recovery methods due to cost, understanding, and health literacy, which indicates there may be further work to do in terms of increasing awareness and understanding of health promotion and wellbeing within a performance context. Many of their PRMD symptoms and locations are consistent with the literature on musicians’ PRMDs (Shanoff, 2020). Based on these results, there is concern that, without injury prevention education, early warning signs for PRMDs or other playing-related issues may be missed, until symptom severity or playing interference is increased. Researchers, educators, and performers alike can all play a role in transforming the situation, with several participants having identified areas for improvement that may address the problem. The lack of effective health instruction during their tertiary education was one of the areas identified by participants, that needed addressing in order to improve the performance health of saxophonists. In addition, there was some misinformation around performance-related injuries that had been given to participants by their teachers, causing them to adjust to postures that were not ideal. Advice like this may interrupt more comfortable, dynamic playing postures, especially for larger instruments, and although well-intended, may continue to be disseminated as those students educate others. Similarly, this was described in Moura and Serra (2024), who highlighted the “no pain, no gain” attitudes, absence of health instruction, and detrimental behaviors passed down in some cases through teacher-directed learning. Improved access to resources and the early implementation of specific and consistent health education in musical training may assist in taking positive steps towards improving musicians’ health and wellbeing. Music researchers are increasingly calling for better health education and health literacy for musicians and instrumental teachers (Evans et al., 2024; Guptill et al., 2022; Wijsman & Ackermann, 2018), a notion supported by the results from this study.
During interviews, participants communicated a view that tertiary education should provide sufficient information to address occupational concerns on a consistent basis, as part of the curriculum, and that it was important not only for performers but for educators as well to be taught this knowledge. Some even considered it not just desirable, but a responsibility, as part of the role of a training institution, to provide a holistic education that reflected the needs and true nature of the profession they were entering. Similar sentiments are expressed in a study by Moura and Serra (2024), that saxophonists have a distinct lack of saxophone-specific scientific knowledge in their training, and that change in university curricula is needed.
With improved education, may come increased health literacy and autonomy over health promoting behaviors in saxophone practice and performance, as well as timely responses to PRMD warning signs and risk factors. During the interviews, it was found that many participants did not consider playing-related pain to be an injury or a PRMD, even if it was chronic or frequently recurring, which was unexpected and concerning. They would discuss the pain, its limitations and challenges, but would then answer in the negative when asked if they had an injury. This may be a consideration in current and future research, where health literacy may have a flow on effect of under-reporting of injuries, potentially influenced by the health literacy of the cohort and the definition used to record injury incidence (e.g., time loss, medical attention) as is described in Clarsen & Bahr (2014).
Due to the spectrum of experiences, diagnosed or undiagnosed pain and injury history, it appeared important to include results on participants’ lived experience with playing-related pain, to further understand the complex nature between musicians and pain and how the cohort understands and responds, particularly as health literacy and experience in engaging with health providers was often low. From these responses, it is necessary to acknowledge some dissatisfaction that exists within the community. Many saxophonists had sought help from medical professionals, saying they were less likely to return or seek out future assistance after bad experiences. These results indicate some frustration in past experiences and a potential to limit patients from seeking further help, contributing to the cycle of performance-related pain. In order to have meaningful change to pain cycles, appropriate performance health education needs to be offered to all relevant stakeholders (for example students, teachers, performers, health professionals, music industry partners) with healthcare providers that understand the occupational demands of musicians so they can intervene effectively. Of those that sought help for a PRMD among this cohort, not one received any saxophone-related practical advice or adjustments from a health professional (such as an altered practice routine or reduced session length/intensity), which was surprising. The results from this research echo many of the experiences held by injured musicians worldwide where there is a need for informed treatment from health professionals (Guptill, 2011) that is sympathetic, and not contradictory with practice requirements. This highlights a potential gap in provider understanding of occupational demand, and possibly a need for musician-led solutions or partnerships between institutions and health providers, wherein targeted, holistic recovery plans may be confidently devised, which include addressing the cause of performance-related pain and not just the symptoms.
Participants desired to know more about health and wellbeing, which was an encouraging result from this cohort study. A willingness to incorporate these perspectives into their playing may positively impact compliance and so finding methods that are easily integrated in their normal routine, that are accessible for the level of health literacy and engaging, may be a place to start when trialing a proof-of-concept or feasibility study with group participants. As a next step, addressing prominent concerns this cohort identified, such as performance anxiety, muscle tension and fatigue, education and playing-related pain, should be considered when designing musician-led interventions that address the needs of saxophonists whilst evaluating health promotion effects.
Responses from within the cohort indicate that playing and performance quality could be affected by psychological and physical health. Part of the pedagogy of saxophonists’ musical training is heavily centered on the refinement of technique, musicality, and skill acquisition (Australian Music Examinations Board, 2020; Michat & Venturi, 2010; Rousseau, 2002). This cohort’s perspectives indicate that there is a need and a desire for poor wellbeing and its negative performance effects to be addressed, with simple strategies to combat the fatigue, MPA or “constant aches and pains” that plague their playing. It was believed that access to trustworthy and accessible sources for performing arts health information, for a variety of different groups such as teachers, students, and professionals, should be a priority for education and the music industry going forward.
Performer-driven research could provide some unique insight on playing-related pain, that has not yet played a significant role in PRMD research for saxophonists, particularly in practical application to technique, cultural, and pedagogical history that comes from player perspectives. Collaborative relationships with health providers, may bridge gaps in understanding as we perform, research and educate one another to consider a range of methods to improve. As mentioned, this cohort has had some experiences with health providers that have led to distrust, misunderstanding, and a lack of confidence in advice offered, not dissimilar to other lived experiences. Therefore, multi-disciplinary research projects that seek to trial interventions should remain in consultation with saxophonists, so that relevant and meaningful solutions can be found that meet cohort needs, and respect pedagogical and performer tradition.
Participants reported factors prohibitive to saxophone development. This cohort expressed that there were several physical and psychological stressors perceived by participants to affect both health and wellbeing as well as their playing ability, such as performance anxiety, muscle fatigue, and tension. This may be a place to begin the aforementioned subject-led interventions. Interestingly, when looking at the stressors for saxophonists, participants voted performing as a mental stressor, along with performance anxiety and repertoire preparation. However, muscle fatigue, muscle tension, and repertoire demands were the perceived physical stressors.
When asked to rate the exertion of different playing contexts, to provide insight on the effort and fatiguability of differing situations, there was a natural progression in exertion with clear results indicating that performances of a solo or outcome-dependent nature are more intense than rehearsals or practice. Although this may seem like common sense, specific training for performance, wherein the training conditions can match the physical and mental requirements of performance, may be a useful avenue for future research.
Given that the rating of perceived exertion (RPE) was regarded as “very hard to very very hard” during solo and outcome-dependent performances, investigating the reason for such high RPE scores (performance anxiety, pain, fitness demands, repertoire level) may be a factor in reducing occupational injury whilst improving sustainable performance outcomes. These results indicate that psychological factors may play a potential role in the exertion level of a performance. Understanding contributing factors to high RPE scores may enhance specific training to decrease performance-related exertion, and reduce PRMD frequency or pain. Matei and Ginsborg (2020) found that bodily pain (impacting performance) and frequency of PRMDs were both related to RPE (but not PRMD severity). Anxiety was not specifically measured in relation to RPE. Similar sentiments from existing research suggest that RPE is not an independent measure, and that several influencing factors such as sociological, personal, or environmental may affect a given score (Haddad et al., 2017), although few other studies have found no correlation between anxiety and RPE during exercise (Coquart et al., 2012), although not specifically tested within a musical cohort. Training to manage these stressors along with physical or psychosomatic symptoms may assist saxophonists in performance practice and wellbeing, and future research investigating psychological factors and their influence on RPE in musical performance may be useful.
Given the relatively high exertion levels, and the regularity of their weekly exercise (mean 6∼ hrs), it may be of interest to conduct research where specific strength and conditioning interventions are trialed and compared for their efficacy in reducing exertion level. Gabbett (2020) describes load progression in relation to sports performance, with the concept of the “floor,” “ceiling,” and “time” to sustainably prepare athletes from their current condition (the floor) to the performance condition (the ceiling) and how training load is increased over time. Similarly, musicians may find it beneficial to progressively work towards “performance condition” in a way that maximizes technical and artistic performance, balanced with the physical demands required. Some studies have already examined this on a case-study level for flutists for the performance of contemporary repertoire (Borkowski, 2011, 2016); however, nothing has been trialed for a cohort of saxophonists. Specific training for physical and psychological demands of performance may be a clear avenue forward for research, in the pursuit of improving performance health for saxophonists. The development of specific guidelines may streamline pedagogical teaching in this area, strengthened with baseline injury prevention education, as a promising preventive measure based on the requests of current saxophonists.
Performance anxiety was a prominent concern for this cohort and, understandably, a desire was expressed for increased performance training and practical strategies for dealing with performance anxiety. Significant research exists on the negative impact of performance anxiety among musicians (Kenny, 2023; Kenny et al., 2004; Studer et al., 2014; Yoshie et al., 2008) and some researchers suggest that injury management and stress management are interlinked: “The ability to cope effectively with stress and anxiety has been found to be crucial in preventing injuries” (Levy et al., 2009, p. 138). Other studies involving saxophonists have suggested that MPA leads to reduced body movement and a lack of control, potentially affecting performance quality (Moura & Serra, 2024). Practical interventions such as yoga, breathing exercises, mindfulness, and meditation have had success in managing physical or psychological symptoms of MPA (Adams, 2012; Butzer et al., 2016; Khalsa & Cope, 2006; Stern et al., 2012; Zhukov, 2019). Papageorgi et al. (2011) found genre-specific differences in MPA prevalence and experience which may be useful for future research in examining this variance. The necessity of implementing practical strategies and health literacy surrounding MPA was an important finding from this study. Equipping them with these skills at the level of this cohort now, such as tertiary and early-career, may be appropriate and timely, where they will begin to develop sustainable habits for themselves and other musicians they teach.
Limitations
There were some limitations to this study. The sample size was small, and sample characteristics were of moderate to highly experienced saxophone players, with low to moderate practice hours which may have biased results. This paper is not intended to be representative of expert musicians’ experiences of injury or pain. Participants mostly resided in Perth or Queensland, Australia, so there was less geographical variance, the study was conducted early in the tertiary academic year, which may have influenced statistics on injury prevalence or practice habits, and participants were pre-professional students and early-career music educators and performers, limiting the inclusion of other perspectives from mid-late career professionals or from those undertaking full-time performance. Future research that involves larger cohort studies to enable by-group analysis of differences between pedagogues, music performance students, and music education students, a variety of career stages, and more full-time performers (such as those in service bands or freelance) may be useful in providing more diverse and robust perspectives.
Conclusion
Several points within the discussion may provide a useful direction for future research. PRMD incidence was comparable to other studies, although a larger cohort study involving Oceania region may provide more robust data. Practical methods for PRMD intervention and prevention that support career sustainability, health promotion and health literacy, and accessible and trustworthy recovery and education-based resources were key points for future research consideration. Performance conditioning and physical/psychological training to match occupational demands were another prominent area to support future music-making and saxophonists’ wellbeing, with research that is saxophone-led as a key finding for investigating practical and appropriate interventions. As these members of the saxophone community engaged in discussions on performance and wellbeing, they were quick to offer areas they believe can influence meaningful change. These areas may be a starting point for practical research investigating saxophonists’ wellbeing. A collaborative, performer-researcher led relationship that guides and navigates performance, health and wellbeing, that is able to flexibly respond to needs in a way that respects current pedagogical and performance practice, whilst holding a space for experimentation and reflection. Results from this study can be used to inform future studies, particularly those that trial the applicability of methods to mitigate common risk factors for poor performance health. An individualized approach using this cohort, may be a useful first step to evaluate practical methods that meet the performance health needs of saxophonists.
Supplemental Material
sj-docx-1-mns-10.1177_20592043251346328 - Supplemental material for Performance Health for Saxophonists: Saxophonists Perspectives and Experiences with Playing-Related Health, Wellbeing, Injuries and Education (Cohort Study)
Supplemental material, sj-docx-1-mns-10.1177_20592043251346328 for Performance Health for Saxophonists: Saxophonists Perspectives and Experiences with Playing-Related Health, Wellbeing, Injuries and Education (Cohort Study) by Nicola Demandolx, Joanna Nicholas, Luke Hopper and Matt Styles in Music & Science
Supplemental Material
sj-docx-2-mns-10.1177_20592043251346328 - Supplemental material for Performance Health for Saxophonists: Saxophonists Perspectives and Experiences with Playing-Related Health, Wellbeing, Injuries and Education (Cohort Study)
Supplemental material, sj-docx-2-mns-10.1177_20592043251346328 for Performance Health for Saxophonists: Saxophonists Perspectives and Experiences with Playing-Related Health, Wellbeing, Injuries and Education (Cohort Study) by Nicola Demandolx, Joanna Nicholas, Luke Hopper and Matt Styles in Music & Science
Footnotes
Action Editor
Elaine King, University of Hull, School of Arts; Peer Review; Nadia Moura, University of Coimbra, Faculty of Arts and Humanities; Raymond MacDonald, University of Edinburgh, Reid School of Music.
Author Contributions
Contributed to conception and design (ND, JN, LH, MS); the acquisition of research data (ND); contribution of knowledge (ND, JN, LH, MS); data processing (ND, JN); analysis (ND) and interpretation of research data (ND, JN, LH, MS) and drafting (ND) and revising the research output (ND, JN, LH, MS).
Consent to Participate
All participants were provided with a participant information letter and completed a written, informed consent form prior to participation
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethics approval has been granted by ECU Human Research Ethics Committee (2021-02576-DEMANDOLX).
Ethics Statement
Ethics approval has been granted by Edith Cowan University’s Human Research Ethics Committee, approval number 2021-02576-DEMANDOLX. All participants were provided with a participant information letter and completed an informed consent form prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ECU Higher Degree by Research (ECU-HDRS) scholarship awarded to the lead researcher (ND) during this period.
Edith Cowan University (grant number ECU Higher Degree by Research (ECU-HDRS) scholarship).
Data Availability Statement
Data generated and analyzed during this study are not available. Ethics approval was granted based on the requirement that data which contains identifiable and sensitive information is to be kept anonymous and seen only by the research team. Participant consent forms and information letter adhered to this condition.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.