
Abstract
Background
Woodwind and brass instrumentalists have a high sensomotoric demand of their orofacial region while playing their instrument. Orofacial problems (OFP) have an influence on the body perception in this area.
Purpose
The aim of this study was to assess and compare the body awareness of the orofacial area in musicians (woodwind/brass) and non-musicians and investigate to what extent OFP may affect the instrumentalists’ body awareness.
Methods
Primary outcome parameters include Two Point Discrimination, Facial Emotion Recognition, Lateralization, and the Tongue and Mouth Imagery Questionnaire (TMIQ). Secondary outcome parameters are colored body drawings and the Central Sensitization Inventory. Musicians additionally filled in the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians – German version. A one-way ANOVA was conducted to assess group differences among the assessments. Body drawings were analyzed qualitatively.
Results
A total of 75 participants were recruited for the study and divided into three groups (control group: CG; musicians without OFP: M − OFP; musicians with OFP: M + OFP). Statistically significant between-group differences were found for both music groups in the TMIQ total-score (M + OFP vs. M − OFP : −6.577, p = .028) and the kinesthetic subscale (M + OFP vs. M − OFP : −3.971, p = .034). Other primary outcome parameters did not show significant differences. For the secondary parameters, statistically significant differences in the CSI were found between affected and non-affected musicians (M + OFP vs. M − OFP : 9.258, p = .004) as well as between the affected musicians and the control group (M + OFP vs. CG: 7.133, p = .043). The qualitative analysis of the body drawings did not show clear group-specific differences.
Conclusion
Based on the results of this study, body awareness of the orofacial region does not significantly differ between musicians and non-musicians. Differences between musicians with and without OFP are small. This project is a valuable contribution to the development of numerous further research projects in the area.
Keywords
Background
Woodwind and brass instrumentalists make up a considerable proportion of the population in Austria and Germany. In both countries, brass music bands are very popular (BDB Akademie Staufen, 2021; Öbv, 2022). In music schools, brass and woodwind instrumentalists make up the majority of students, with even more enrolled students compared with stringed instruments (Statistik Austria, 2023). In a professional orchestra, the counts of instrumentalists in the bowed string instrument section and the wind and brass section are quite balanced; however, no official statistics are accessible to verify exact figures.
To perform on a woodwind or brass instrument, very high fine motor control of the facial muscles and tongue are necessary. To produce a tone, including pitch and sound regulation as well as articulation, accurate synergy of these muscles is required (Barros et al., 2018; Stahl, 2023; Yeo et al., 2002), which is known as “Embouchure.” This process is supported by and complemented by the breath, or more accurately, breath control (Woldendorp et al., 2016).
Playing woodwind or brass instruments places significant sensorimotor demands on the orofacial region, stressing the temporomandibular joint and the masticatory and facial muscles. This can lead to musculoskeletal issues. Various studies have explored the prevalence and factors contributing to temporomandibular dysfunctions (TMD) in woodwind and brass instrumentalists (Campos et al., 2021; Lee et al., 2013). The definition of TMD as well as an assessment protocol are accessible online (International Network for Orofacial Pain and Related Disorders Methodology, n.d.; Ohrbach, 2016). According to these, TMD include restricted range of motion with or without clicking noise and/or pain as well as pain in the masticatory muscles (Ohrbach et al., 2013; Schiffman et al., 2014).
Ongoing pain may influence body perception and consequently impact on the somatosensory cortical fields (Moseley & Flor, 2012). Changes to the somatosensory network of the facial area may be revealed by less accurate scores of the Two Point Discrimination (TPD) test as well as lower scoring in Facial Emotion Recognition (FER) and Lateralization testing (LAT) (Taxer et al., 2024; von Piekartz & Paris-Alemany, 2021; von Piekartz et al., 2015).
Body perception is also influenced by the utilization and involvement in movements of the corresponding body region. Given the intense engagement of the orofacial area when learning to play a musical instrument, one might assume that body awareness of the orofacial area is different in woodwind and brass musicians compared with non-musicians. A systematic literature review performed in December 2022 and repeated in June 2023 did not reveal any publication that addresses differences in body awareness of the orofacial area of woodwind and/or brass instrumentalists with or without orofacial problems compared with healthy non-musicians. Therefore, the aim of the study was to investigate whether body awareness of the orofacial area of woodwind and brass instrumentalists is different to non-musicians. Additionally, the impact of orofacial problems on body awareness of the orofacial area in brass/woodwind musicians was explored.
Methods
Ethical Approval
This research was approved by the local Institutional Review Board (“Ethics Board”) of the University of Applied Sciences Osnabrueck in January 2023 (approval number: WiSo_MA_OMT_SoSe23_1_2).
Research Questions
Based on the study aim, two research questions were formulated.
Is body awareness of the orofacial area in healthy woodwind and brass instrumentalists different to healthy non-musicians? Is body awareness of the orofacial area in woodwind and brass instrumentalists with orofacial complaints different to woodwind and brass instrumentalists without orofacial complaints?
The hypotheses were deduced from these questions referring to the primary and secondary outcome measures in a three-group comparison. In general, H0 constitutes equality of each group, whereas H1 constitutes a difference in at least one of the groups.
Study Design
This study is an observational study using a case-control design. The study population consists of brass and woodwind instrumentalist with and without orofacial problems (M + OFP and M − OFP, respectively) and a healthy non-musical control group (CG). For this study, the term “orofacial problems” was chosen on purpose to not be limited to TMD-patients exclusively but include participants with muscular discomfort or general discomfort in the jaw area or facial pain too and allow for higher participation rate.
To evaluate orofacial body perception, several assessments were chosen. Primary outcome parameters include TPD, FER, LAT, and the Tongue and Mouth Imagery Questionnaire (TMIQ). Secondary outcome parameters were body drawings (BD) and the Central Sensitization Inventory (CSI). Additionally, a clinical examination of the temporomandibular joint was performed in accordance with the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) axis I criteria. Musicians were additionally given the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians – German version (MPIIQM-G). Musicians who scored ≥ 4 points on the Craniofacial Pain and Disability Inventory (CF-PDI) and presented with positive findings in the DC/TMD axis I protocol were allocated to the M + OFP group.
All examinations were performed by the first and second author, who are both physiotherapists with certificates for orthopedic manual physiotherapy. The certification program includes the standard examination (and treatment) of the temporomandibular and orofacial areas. Literature shows that self-instruction of the DC/TMD protocol yields sufficient reliability in diagnostic accuracy but benefits from a two-day course and calibration session (Vilanova et al., 2015). In this study, the DC/TMD axis I protocol was self-instructed and practiced before it was demonstrated to and approved by the third author, who is a professor for physiotherapy and manual therapist highly experienced with examining and treating patients with orofacial complaints.
Data were collected at one point in time. Demographic data such as age and gender were collected from all participants. The musicians were additionally asked instrument-specific information, including main and secondary instrument, weekly playing time and overall time of playing, genre/style of music, and educational background (all for the main instrument). All participants were clinically examined including a brief patient history on musculoskeletal and other complaints to screen for possible exclusion criteria. The physical examination of the orofacial area included measurement of range of motion in all planes of the temporomandibular joint (TMJ), pain reproduction upon palpation of the TMJ, and evaluation of the accessory movements of the TMJ looking for range of motion or pain reproduction. Palpation was also performed for the masticatory muscles, including the masseter, temporalis, sternocleidomastoid, and adjacent muscles such as the upper trapezius and obliquus superior for possible pain provocation. The standard DC/TMD protocol is in English (Ohrbach, 2016) and has been translated to German (Ohrbach, 2016), the version used in this study. The protocol is available online at https://ubwp.buffalo.edu/rdc-tmdinternational/tmd-assessmentdiagnosis/dc-tmd-translations/.
The detailed sequence of the appointment is described below.
The study was started in October 2022 and completed in July 2023. The datasets, examination forms, and body drawings generated and/or analyzed during the current study are available from the corresponding author on reasonable request (Lesjak, 2024).
Participants
Prospective participants were recruited with help of posters in physiotherapy practices in Gütersloh (Germany) and Graz (Austria); via social media including Instagram, Facebook, and WhatsApp; by email newsletters to brass bands, orchestras, music schools and universities; and by word by mouth.
Participation was voluntary, and all interested participants were given printed informed consent and data protection forms to sign before data were collected. With their signature they agreed to participation and the processing of their anonymous data but were able to withdraw at any point without reason.
Inclusion and exclusion criteria were defined for all participants regardless of possible group allocation with group-specific criteria added.
Inclusion Criteria
Participants had to be 18–65 years of age and fluent in German (speech and writing) to be considered for the study. For the music groups, only performers with their main instrument being a brass or woodwind instrument were eligible. Other main instrument groups were not included, and second instruments did not influence the in- or exclusion. Participants for the control group should be healthy and have no musical experience (present or past). Additionally, musicians presenting with orofacial or temporomandibular problems were included in the study. These candidates had to meet the DC/TMD recommendations of orofacial or temporomandibular problems, and furthermore a CF-PDI score of ≥ 4 was necessary to be considered for the M + OFP group.
Exclusion Criteria
Candidates were excluded if they presented with acute (within the previous three months) or chronic (longer than three months) pain (except for benign headaches or pain in the orofacial area). Studies investigating ongoing pain in the lower back area show that body perception may be influenced by the pain (Moseley & Flor, 2012). To avoid any carryover effects from altered body perception of a different body part to the orofacial area, participants with chronic pain were excluded. Also, patients were excluded if they suffered from rheumatic disorders or neurological or psychological diseases, in accordance with other studies (Treede et al., 2019). Frequent medication affecting body perception, anesthetics in the orofacial area within the previous 24 h, trauma to the face and/or head within the past three months, or orofacial surgery also disqualified participants.
Assessments
With exception of the body drawings (BD), all assessments have been validated for clinical and scientific use.
Body Drawings (BD)
The BD were specifically developed for the purpose of this study and are made up of two parts. First, candidates listened to a recorded body scan protocol of the head, face, and mouth before they filled in a standardized body chart. The second part comprises of a recorded body scan protocol of the mouth, tongue, and teeth, which candidates listened to before filling in another body chart. Each part of the body scan protocol lasted about seven minutes, editing time for the body charts was set at one minute. The intention of the short timeframe was to enforce a spontaneous response of the most present sensation in that moment and to avoid the editing process being based on reasoning or assumptions about an assumed correct solution of the task.
To fill in the charts, candidates were given colored pencils in different shapes. Each color represented a quality of felt sense, including “warmth,” “cold,” “tension,” “relaxation,” “pleasant,” “uncomfortable,” and “intensity of sensation.” The shape of the pencil represented the perceived intensity of each sense on a scale of 0 = “no sensation,” 1 = mild sensation,” 2 = “moderate sensation,” and 3 = “intense sensation.”
This assessment has been developed based on pain drawings, which have been used in studies before. In TMD patients, pain drawings show high test–retest reliability (Pitance et al., 2021).
In other studies, pain drawings have been used to differentiate between neuropathic and non-neuropathic pain in patients presenting with lower back pain with and without radiating pain to the lower extremities. The diagnostic accuracy of the pain drawings yielded a sensitivity of 80.1% and a specificity of 80.6% compared with standard clinical diagnostics and, furthermore, showed a high agreement between evaluators (Sehgal et al., 2021).
Craniofacial Pain and Disability Inventory (German Version) (CF-PDI-G)
The Craniofacial Pain and Disability Inventory (German version) is a self-report questionnaire comprising of 21 items evaluating pain, disability, and functional status of the mandibular and craniofacial regions. The score ranges between 0–63, with higher values meaning higher levels of pain and disability. It shows excellent test–retest reliability (La Touche et al., 2014) and a high (La Touche et al., 2014) to excellent (von Piekartz et al., 2021) internal consistency. The cut-off value to discriminate between patients and healthy controls is ≥ 4, with a sensitivity of 85% and specificity 88% (von Piekartz et al., 2021). In present study, the CF-PDI and DC/TMD serve as indicators for allocation to the M + OFP group.
Central Sensitization Inventory (German Version) (CSI-G)
The (German) Central Sensitization Inventory is a self-report questionnaire made up by two parts. In the first part, items associated with central sensitization processes are prompted yielding an overall score of 0–100. Higher values correspond with a higher level of central sensitization. The cut-off value to discriminate between healthy control and patients is 40 points. The inventory shows excellent test–retest reliability and 81% sensitivity and 79% sensitivity (Klute et al., 2021; Neblett et al., 2013).
Diagnostic Criteria for Temporomandibular Dysfunctions (DC/TMD) Axis I
The clinical examination of the temporomandibular joint followed the protocol from the Diagnostic Criteria for Temporomandibular Dysfunctions (DC/TMD) axis I. The protocol assesses range of motion and palpation and presence of pain or articular irregularities. Also, the “TMD pain screener” and “symptom-related questionnaire” were handed out and filled in by the participants. For all documents, German versions were used (Ohrbach, 2016). As proposed by the protocol, palpation was performed using an algometer (Wagner Instruments). Testing position for patients was upright sitting with a neutral head position (La Touche et al., 2011).
The German version of the axis I protocol shows high inter-rater reliability and high sensitivity and specificity for diagnosing myalgias, myalgias with radiating pain, and arthralgias (Schiffman et al., 2014).
Facial Emotion Recognition (FER) and Lateralization (LAT)
FER and LAT can both be tested using the My Face Training software (My Face Training, 2018). In both modalities, 42 pictures are shown for 10 s, including men and women from adolescent to adult age. For the emotion recognition testing, the candidate needs to identify the emotion displayed from one of six basic emotions. The options are “anger,” “disgust,” “joy,” “astonishment,” “fear,” and “sadness.” In the LAT testing, the candidate has to decide whether the depicted face shows a change in mimic on the right or left side of the face. Only correct answers are counted, yielding a score of 0–42 (von Piekartz & Paris-Alemany, 2021). People presenting with facial pain score lower on average on both tests compared with healthy controls (von Piekartz et al., 2015). The testing modalities of the My Face Training software are based on the facially-expressed-emotion-labelling-assessment, which shows a moderate internal consistency in healthy participants (Kessler et al., 2002).
MPIIQM-G
The musicians were given a self-report questionnaire that has been specifically developed for orchestral musicians, the Musculoskeletal Pain Intensity and Interference Questionnaire (German version). It assesses the extent of pain intensity while playing one's instrument and any interference with musical performance. The “Pain Intensity” subscale includes four items, and the “Pain Interference” subscale includes five items. Each of these is rated on a numeric rating scale (0–10, where 10 is the maximum), resulting in a score of 0–40 for “Intensity” and 0–50 for “Interference” (Berque et al., 2014).
The German version shows high test–retest reliability and a high degree of internal consistency (Möller et al., 2019).
Tongue and Mouth Imagery Questionnaire (TMIQ)
The Tongue and Mouth Imagery Questionnaire (TMIQ) is a newly developed tool to assess motor imagery (MI) of the orofacial area. It is made up of two subscales, the “kinaesthetic MI” (kMI) and the “visual MI” (vMI). Taken together, these scores amount to the overall score (Alvarado et al., 2022).
The assessment is made up of five different movement instructions (items). The patient is sitting in an upright position, and the examiner reads the instructions out loud. The participant first performs the movement and then imagines the same from a first person perspective. Afterwards, the participant immediately rates on a scale 1–5 how clearly they visualized the movement (vMI) and how intense the movement was in their imagination (kMI). After this, they rate the extent of pain while performing or imagining the movement on a scale 0–10. This is repeated for each movement. Therefore, scores range from 5–25 for kMI and vMI, 10–50 for MI overall, and 0–50 for pain. Higher MI scores represent clearer/more intense MI; higher pain scores equate to higher intensity of pain (Alvarado et al., 2022).
The assessment shows good reliability and validity for both TMD patients and healthy controls (Alvarado et al., 2022).
Two Point Discrimination (TPD)
In the present study, TPD has been taken from the mandibular nerve (V3) area (mandible right and left) and additionally from the orbicularis oris area and the lips (see Figure 1). The orbicular area and the lips were each divided into four areas: upper right/upper left orbicularis oris, lower right/lower left orbicularis oris, upper lip right/left, and lower lip right/left. Overall, ten sites were evaluated.

Two point discrimination (testing sites).
In accordance with previously conducted studies, a “two-point discrim-a-gon” (Baseline) tool was used for the testing (von Piekartz & Mohr, 2014). This tool is made from plastic and is a round wheel with spikes that are set at a specific distance starting at 25 mm, then 20 mm, and then in a 1 mm decrease from 15 mm to 2 mm. The patients lay supine with their eyes closed. The assessment tool touched the tested skin perpendicular for one second three consecutive times before the tested person had to reply whether they felt one or two contact points. They were also given the option to declare “I don’t know,” which was equated to “one point.” To obtain one measurement, two calculation values are necessary. First, distances are tested in descending manner until only one contact point is felt (or the tested person was not sure), representing the first calculation value. Then, the same area is tested with increasing distances until two points are felt again, which is the second calculation value. The mean of both calculation values yields the first measurement value. For each testing area, three measurement values are taken in alternating manner (first right, then left). The mean of all three measurements represents the final TPD value.
TPD has been performed in the facial area in studies before, obtaining measurements from the V1, V2, and V3 areas. Patients presenting with temporomandibular or orofacial problems show less accurate TPD measurements compared with healthy controls. Intra-tester reliability for TMD patients is moderate and inter-tester reliability for healthy participants is moderate-to-good (ICC 0.64–0.80) (La Touche et al., 2020).
Data Collection
Data collection was done in person following a set protocol.
Signing informed consent & data protection forms Patient history Clinical examination of the temporomandibular joint including range of motion, palpation, and passive accessory movement Two Point Discrimination Body scan & body drawings FER & LAT TMIQ Assessments: CF-PDI and CSI (all); MPIIQM-G (musicians only)
Data collection and entry into the statistics program was done independently. After all participants were tested and all data entered, the analysis was performed by collaboration of the first and second authors.
Once the data collection process was started, participants were given an identification number to ensure data protection and minimize traceability. The process was semi-blinded as investigators independently collected data of only one participant at a time but therefore knew the results of this participant.
If group allocation was not clear, the other investigator reviewed the anonymized data collection and assessment forms to help decide. Uncertain cases were only included upon consensus between the investigators.
Data Analysis
Data analysis was performed using IBM SPSS Statistics 28 software for windows (IBM, Armonk, NY). Descriptive statistics were used to present demographic information as well as instrumental characteristics such as time spent playing the instrument and overall years of playing (musicians only).
A one-way ANOVA was conducted to compare the three groups measured by the numerical outcomes of the primary and secondary outcomes. Significant between-group differences were further analyzed using the Bonferroni post hoc test. Correlations between categorical data were analyzed using cross-tabulation and chi-square-tests if necessary. These data are available in the supplements.
Qualitative analysis was implemented on the body drawings. Criteria of the analysis were the chosen color, where each color was coded with a different quality of sensation, its scale (representing the intensity of sensation from 0–4), and the body parts that were colored. The body charts of the head and mouth were divided into a rough grid (forehead, nose, eye and orbital area, upper jaw, lower jaw, upper or lower lips, upper or lower teeth on either the right or the left side of the face, right or left side of the tongue, tip or base of the tongue). The results are reported in frequencies (color and body parts) and scores (scale of color).
Level of significance for all tests was set at p ≤ 0.05.
Results
Sample
Participants were recruited and tested within a set time frame (March to May 2023). The total sample size is n = 75. Of these, n = 32 make up the M − OFP group, n = 15 the M + OFP group and n = 28 were allocated to the CG. Overall, 48 women and 27 men participated, with a mean age of 37 years. Distribution of gender and age within each group can be found in Table 1.
Population characteristics.

Note. CG: control group, M − OFP: musicians without orofacial problems, M + OFP: musicians with orofacial problems, n: number of participants, w: women, m: men, SD: standard deviation, “mandatory”: work related playing time, “additional”: not work related or recreational purpose.
The weekly amount of time spent playing the instrument is on average 13.5 h (M − OFP) and 5.5 h (M + OFP). Detailed information on mandatory and additional playing time in each group can also be found in Table 1.
The most popular instrument in both the M + OFP and the M − OFP group is trumpet or flugelhorn. If one is played, second instruments fall into brass instrument or drum kit groups. The distribution of main instruments can be found in Figure 2.

Main instrument by popularity.
Retrospectively, the data revealed that the group of musicians presenting with “orofacial problems” could be further subclassified into “temporomandibular disorders” (TMD). None of the participants in the M + OFP group reported symptoms that would justify using the term “orofacial,” but all rather showed a clear TMD presentation. As the variables and groups had been defined a priori, the description “OFP” is kept in the analysis and report.
Research Questions
The omnibus test of the one-way ANOVA revealed that groups showed statistically significant differences in the TMIQ overall and TMIQ kMI scores (TMIQ overall: F(2.72) = 3.731, p = .029 and TMIQ kMI: F(2.72) = 3.837, p = .026) as well as in CSI scores (F(2.72) = 5.630, p = .005).
Post hoc Bonferroni tests show group-specific differences. On average, the TMIQ kMI and TMIQ overall scores were lower in the M + OFP group compared with the M − OFP group. The CSI is statistically higher in the M + OFP group compared with the CG and is higher on a non-statistically significant level compared with the M − OFP group. The average between-group difference and level of significance for these assessments can be found in Table 2.
Between-group differences (ANOVA post hoc).

*Bonferroni post-hoc test; level of significance p ≤ .05.
Results of group scores and between-group differences are average scores. Bold scores represent statistically significant differences between groups.
Notes. CG: control group, M − OFP: musicians without orofacial problems, M + OFP: musicians with orofacial problems, CSI: Central Sensitization Inventory, TMIQ: Tongue and Mouth Imagery Questionnaire, kMI: Kinesthetic motor imagery.
Other assessment scores did not show statistically significant between-group differences. The scores of all numerical primary and secondary outcomes are displayed in Table 3.
All assessment scores.

Notes. CG: control group, M − OFP: musicians without orofacial problems, M + OFP: musicians with orofacial problems, N/A: not applicable. CSI: Central Sensitization Inventory, FER: Facial Emotion Recognition, LAT: Lateralization, MPIIQM-G: Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians – German version, TMIQ: Tongue and Mouth Imagery Questionnaire, TPD: Two Point Discrimination. SD: standard deviation.
Based on these results, research question 1 is to be negated: Healthy woodwind and brass musicians do not show differences in their body perception of the orofacial area compared with healthy non-musicians.
Research question 2 can be partially approved: Woodwind and brass musicians with orofacial problems show differences in their body perception of the orofacial area regarding kinesthetic and overall motor imagery compared with musicians without orofacial problems.
Body Scans
Visual revision of the body drawings did not show distinct differences between the groups. Completion of coloring the body chart was very heterogenous. Some participants would only draw crosses where a specific sensation was recognized, whereas others would circle the area, and still others would fully color the area.
Most commonly, the body drawing was uncolored, which refers to “no sensation” of a quality. In the M + OFP group, the most common chosen sensation was “tension,” in the M − OFP group “relaxation,” and in the CG “tension.” Table 4 lists the absolute and relative numbers of drawn sensations.
Body-drawing sensations.
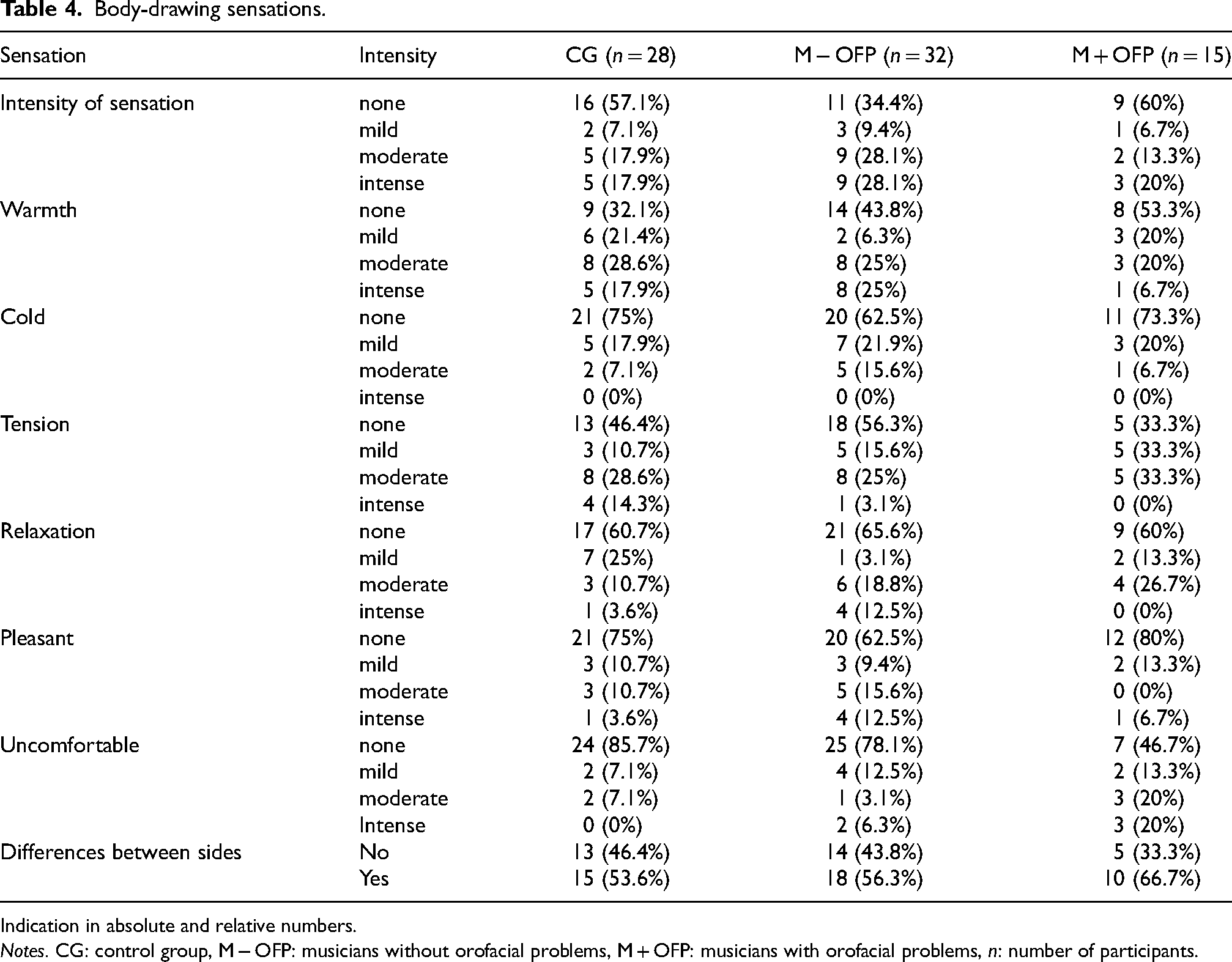
Indication in absolute and relative numbers.
Notes. CG: control group, M − OFP: musicians without orofacial problems, M + OFP: musicians with orofacial problems, n: number of participants.
In all groups the most common areas to be colored were the upper lip, the tongue, and the lower lip. Within these areas, some distinct differences between groups are noticeable. The upper lip was predominantly colored in the M − OFP group, the tongue predominantly in the CG, and the lower lip again was most popular in the M − OFP group. In the M + OFP group, no body part was clearly preferred.
Additional Analysis
Further exploration of the dataset revealed that in the M + OFP group more women than men were included (w = 13, m = 2), whereas the gender distribution in other groups was balanced (see Table 1). The χ2-test showed that gender distribution in the M + OFP group is statistically significant (χ2(1) = 4.977, p = .026, ϕ = −0.325). The odds for women to be included in the M + OFP group in this sample is 5.73 times higher compared with men.
For the music groups, a correlation analysis was performed for the primary outcome parameters that showed significant group differences in the ANOVA and the additional parameters. Some variables show statistically significant correlations.
There was a moderate negative correlation between age and FER (r = −.467, p < .001) and LAT (r = −.456, p = .001). With increasing age, FER and LAT scores decrease.
FER was moderately correlated with playing experience (years of playing the instrument) (r = −.474, p < .001), weekly mandatory playing time (r = −.418, p = .003), weekly additional playing time (r = −.345, p = .18) and overall playing time (r = −.437, p = .002). LAT scores do not show correlations to playing time or playing experience.
For motor imagery, playing experience is not correlated to any of the subscales or the overall TMIQ score. The Visual MI score was moderately correlated to overall weekly playing time (r = .314, p = .031). For kMI, moderate correlations were found for mandatory weekly playing time (r = .378, p = .009), weekly additional playing time (r = .317, p = .03), and overall weekly playing time (r = .4, p = .005). Overall TMIQ scores showed moderate correlation with weekly mandatory playing time (r = .365, p = .012), with additional weekly playing time (r = .334, p = .022), and with overall playing time (r = .4, p = .005). According to these results, motor imagery scores increased with increasing playing time.
In the music groups, CSI was moderately negatively correlated with TMIQ vMI (r = −.395, p = .006) and the TMIQ overall score (r = −.363, p = .012).
Results of the correlation analysis and chi-square test can be found in the Supplemental Material.
Discussion
In the present study, body awareness of the orofacial area of woodwind and brass instrumentalists with and without orofacial problems was assessed and compared with healthy non-musicians. Musicians with orofacial problems show significant differences in motor imagery, and especially kinesthetic MI, compared with musicians without orofacial problems. Body awareness between healthy instrumentalists and non-musicians does not show significant differences.
Regarding the research questions, question 1 should be negated: Healthy woodwind and brass musicians do not show differences in their body perception of the orofacial area compared with healthy non-musicians. And research question 2 can be partially approved as woodwind and brass musicians with orofacial problems show differences in their body perception of the orofacial area regarding both kinesthetic and overall motor imagery compared with musicians without orofacial problems.
Taking a closer look at the results for the TMIQ (Table 5), the average scores of the TMIQ and both subscales are higher in the M + OFP group compared with non-instrumentalist patients with TMD from the original study. Also, average scores of all scales of the M − OFP group and CG in the present study are higher compared with the original study, except for the kMI score in the CG (Alvarado et al., 2022).
TMIQ Scores.

Notes. TMDorig: patient group of the original study of the TMIQ assessment (Alvarado et al., 2022), CGorig: control group of the original study of the TMIQ assessment (Alvarado et al., 2022), M + OFP: musicians with orofacial problems, M − OFP: musicians without orofacial problems, CG: control group (non-musicians), vMI: visual motor imagery, kMI: kinesthetic motor imagery, TMIQ: Tongue and mouth imagery questionnaire, overall score, All scores in means
*
Also, significant positive correlations were revealed between overall weekly playing time and all TMIQ scores in the music groups (data published in the supplements). Our study indicates that body awareness and motor imagery in the orofacial area are more accurately developed in musicians that have a higher weekly playing times. This could be explained by the fact that practicing or playing a woodwind or brass instrument requires control of the facial muscles, tongue, and breath. Consequently, higher playing or practicing times equate to longer or more intense engagement with these body areas.
The average scores of the TPD V3 area (mandible) of the M + OFP group are slightly lower compared with results from studies on non-musician patients with TMD (La Touche et al., 2020). This too may indicate that playing a musical instrument, specifically woodwind or brass, may help to develop a more accurate epicritic sensation in the orofacial area, despite TMD.
Due to the better scoring of the M + OFP compared with non-musicians with TMD in the TMIQ and TPD, it might be advisable to study this population further. This is especially true where the intention is to establish reference scores for these assessments to avoid false-negative evaluation of musicians presenting in clinic.
Regarding secondary outcome parameters, the body drawings did not reveal striking differences between the music groups and the CG. The data analysis was exploratory, and during the examination process, a great variance in handling the task was observed. Evaluation and interpretation were left to the judgment of the responsible investigator. In this study, the intention was to observe whether this assessment is applicable and accepted by the participants and to explore whether differences in body perception are represented by these drawings. They were included due to encouraging findings from other studies, which indicated that colored pain drawings are an effective method for classifying pain in the orofacial region (Pitance et al., 2021). A more sophisticated method of evaluating colored body charts might be with help of a grid, which has been applied in other studies, in both digital drawings (Pitance et al., 2021) and paper drawings (Herpel et al., 2023).
Although additional data on instrument-specific information was collected, an in-depth investigation of possible associations with OFP was not performed in this study due to time constraints. Similarly to our findings, results from systematic reviews suggest that playing time (Campos et al., 2021) and the female gender (van Selms et al., 2020) seem to be associated with the presence of TMD in musicians. Female musicians in general seem to be more likely to report performance-related musculoskeletal pain compared with men (Paarup et al., 2011). Furthermore, women in general seem to be more likely to develop TMD compared with men (Bueno et al., 2018). The results of this study confirm those trends, but, as highlighted by Taxer et al., (2024), who did a systematic review on body disturbances in patients with orofacial complaints, comparability of results is limited due to lack of additional information or missing statistical models investigating secondary parameters or additional variables in regard to the primary outcome. This confirms that future research dedicated to better understanding OFP in musicians is needed and that statistical models analyzing instrument-specific information, as well as demographic data and its possible associations with OFP, should be performed thoroughly.
Limitations
Some limitations need to be acknowledged.
First, this study is based on a case-control design with a limited time frame of recruitment. Hence, assumptions on prevalence of orofacial or temporomandibular disorders cannot be drawn from this data. Also, the sample size needs to be larger to reach a higher power. Calculations performed with G* power show that for a three-group comparison to reach 80% of power with a moderate effect size and a significance level of α=0.05, at least n = 180 participants are needed (Faul et al., 2009). Also, distribution between the groups is not equal, as the M + OFP group is smaller compared with the M − OFP and the CG. Furthermore, influences on the assessments cannot be fully excluded. First, the overall duration of the examination took up 70 to 90 min, and fatigue or loss of concentration might have negatively influenced the assessments performed toward the end of the session. Additionally, TPD measurements may be different in men with or without a beard. Although within all groups the men had a mix of beards and no beards, a difference between those candidates was not controlled for. The TMIQ assessment was translated from English to German by the assessors of the study. No validation study was conducted prior to using the assessment in German, and linguistic misunderstandings might impact the performance in the assessment. Regarding the body drawings, it needs to be considered that the time to fill in the body charts was about one minute and therefore very short. Some of the participants had initial difficulties completing the charts and may have needed more time to illustrate the full scope of their perceptions.
Most importantly, future research may focus on instrument-specific influence. For example, thorough subgroup analysis between instrumental groups or even single instrument types may yield more specific information on differences due to instrument played. Also, weekly time playing the instrument and overall experience (years playing one's instrument) show correlations with some of the main outcome parameters and should be considered as covariables in the statistical analysis. Furthermore, future research might investigate whether a systematic approach to teaching embouchure in comparison with an intuitive approach impacts on body perception. Also, the groups of interest might be extended and include musicians with other disorders and diseases, such as focal dystonia (embouchure dystonia), or musicians who are not actively performing (anymore). Also, other age groups should be considered for future research. In larger study populations, subgrouping of amateur and professional players might be advisable to collect other possible influencing factors on the development of playing-related disorders.
Strengths
First, the study population is made up solely from woodwind and brass instrumentalists. In comparison with other instrumental groups, such as singers or stringed instrumentalists, these groups are not as strongly represented in research but rather make up a part of a study population in, for example, research on orchestral musicians. In future, one may subclassify the population based on single woodwind or brass instruments. The different shapes and types of mouthpieces and reeds may induce heterogeneity of data. A subclassification based on instrument played may warrant robust conclusions to be drawn from the studies. Also, participants gave positive feedback on the body drawings. They commented that with the help of the provided colors and the structured body scan, perceptions could be communicated and presented “directly,” “unfiltered,” and “systematically.” They felt able to overcome any difficulty in expressing personal perceptions due to lack of words or descriptors. Previous studies explored the association of pain drawings with functional limitations. The extent of colored area on the body chart is associated with level of central sensitization and headache disability (Pitance et al., 2021) as well as level of pain, depression, and anxiety (Herpel et al., 2023; Pitance et al., 2021). The marked surface area was not associated with functional limitations of the TMJ (Herpel et al., 2023). Conclusions and implications • A difference in body awareness between (healthy) musicians and (healthy) non-musicians could not be shown by the implemented assessments. While no discriminative assessment tool or test battery is identified that captures the unique demands of musicians, a thorough clinical examination is key to a specific and individualized treatment. • Further development of the assessment battery is necessary and highly encouraged to facilitate depiction of the musician's demands in a clinical context. • Considering interventions, the fact that musicians presenting with OFP show differences in motor imagery scores but not in FER or LAT leads to the assumption that body-dysmorphic disorders are very unlikely to be present in this sample. Therefore, suggested interventions for these patients should primarily aim at motor control and motor imagery exercises.
Studies also show that the painful area is not limited to the TMJ area but could spread to almost all parts of the face, but in general the drawings are very heterogenous (Pitance et al., 2021). Body drawings, therefore, may be a valuable tool not only to evaluate pain distribution and therefore support clinical diagnosis; clinicians may also gain further insight into subjective perception of the orofacial area, which may help navigate what body parts need to be addressed in interventions focusing on body awareness.
Supplemental Material
sj-pdf-1-mns-10.1177_20592043241288636 - Supplemental material for Body Awareness of the Orofacial Area in Wind and Brass Instrumentalists: An Observational Study
Supplemental material, sj-pdf-1-mns-10.1177_20592043241288636 for Body Awareness of the Orofacial Area in Wind and Brass Instrumentalists: An Observational Study by Sarah Lesjak, Lena Ostlangenberg, Harry von Piekartz and Christoff Zalpour in Music & Science
Supplemental Material
sj-pdf-2-mns-10.1177_20592043241288636 - Supplemental material for Body Awareness of the Orofacial Area in Wind and Brass Instrumentalists: An Observational Study
Supplemental material, sj-pdf-2-mns-10.1177_20592043241288636 for Body Awareness of the Orofacial Area in Wind and Brass Instrumentalists: An Observational Study by Sarah Lesjak, Lena Ostlangenberg, Harry von Piekartz and Christoff Zalpour in Music & Science
Footnotes
Acknowledgements
The authors would like to thank the management teams of the Praxis orange in Graz, namely Elisabeth Charusa, Silvia Eger-Marte, Karl-Heinz Klade, and Hubert Kriebernegg, as well as the management team of Mobile GMbH, namely Dr. Sebastian Mäueler and Benjamin Mäueler, for generously providing the facilities for the data collection. The authors also thank Prof. Nikolaus Ballenberger, PhD, for his advice on methodology and study design.
Action Editor
Eckart Altenmüller, Institut für Musikphysiologie und Musikermedizin, Hochschule für Musik, Theater und Medien Hannover.
Peer Review
Alexandra Türk-Espitalier, University of Music and Performing Arts Vienna, Musicphysiology. Eckart Altenmüller, Institut für Musikphysiologie und Musikermedizin, Hochschule für Musik, Theater und Medien Hannover.
Contributorship
HvP and CZ facilitated the idea, and SL and LO researched the literature, drafted and conducted the study, and performed the data analysis. HvP and CZ were involved in developing the study design, gaining ethical approval, and contributed clinical expertise to the examination protocol and interpretation of the data. SL wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This research was approved by the local Institutional Review Board (“Ethics Board”) of the University of Applied Sciences Osnabrueck in January 2023 (approval number: WiSo_MA_OMT_SoSe23_1_2).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data collected for the research project “Body Awareness of the Orofacial Area in Wind and Brass Instrumentalists. An Observational Study.” is available upon reasonable request. The corresponding author may reserve the right to deny access to data when needed. Sharing of data may be granted in case of sincere research interest or further development of the project (Lesjak, 2024).
Supplemental Material
Supplemental material for this article is available online.
Appendix
Name: Sarah Lesjak
Unterschrift:
Name: Lena Ostlangenberg
Unterschrift.
Datum 11.01.2023
Datenschutzbestimmungen beurteilen zu können.
Name: Prof. Dr. C. Zalpour (Mitglied der Ethik-Kommission)
Unterschrift:
Datum 15.01.2023
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.