
Abstract
Previous research suggests that the conductor's choice of preparatory gesture affects choral singers’ breathing behavior as well as the corresponding loudness and sound quality. As these gestures are in choral practice often combined with instructions on the desired breathing technique, the aim of this study was to explore whether congruent and incongruent combinations of preparatory gestures with breathing instructions affect the breathing behavior and resulting loudness in choral singers. In our within-subjects study design, 18 healthy choral singers were asked to sing a tone in response to 4 different video stimuli, consisting of two congruent and two incongruent gesture-instruction combinations. We recorded chest wall kinematics via three-dimensional motion capture and voice samples. The results show that the used preparatory gesture has an influence on the predetermined inhalation type. Particularly, the most common inward-upward gesture combined with an abdominal inhalation results in a significantly reduced chest wall expansion and loudness of the resulting tone. Furthermore, the moment of maximum inhalation and onset are delayed after inward-upward gestures. Consequently, in choral practice, it is essential to generally consider that the selected preparatory gesture has significant influence on the resulting sound and should therefore be chosen according to the desired type of inhalation.
Keywords
Introduction
An active control of specific breathing techniques is considered to be an essential factor in classical singing. For solo singers, a distinct breathing strategy is individually chosen by each singer and depends on the intended singing style, loudness, and sound quality (Griffin et al., 1995; Iwarsson & Sundberg, 1998; Sundberg, 1992; Thomasson, 2003; Thorpe et al., 2001). However, choral singers usually follow the verbal directions and visual cues of a conductor to achieve a temporally and technically uniform inhalation and tone production, which is a prerequisite for a homogeneous choral sound. During rehearsals, the conductor usually gives instructions concerning the desired sound quality and – especially in the case of non-professional singers – also on how choristers should inhale. For example, at the beginning of each piece, the conductor uses the so-called preparatory gesture to coordinate mutual inhalation and onset time.
The majority of the conducting literature (e.g., Ericson et al., 1974; Hamann and Cooper, 2016; Kahn, 1975; Seaman, 2013; Thomas, 1967) suggests that the gesture depends only on the trajectory of the beat pattern and could be any movement within the pattern, as long as it shows a full beat before the starting point. This common description can lead to quite contrasting movement forms and directions: In the case of a start of a musical piece on beat one, an inward-upward movement of the arms would be used; when having a piece with an “up-beat”, for example a start on the fourth beat of a 4/4 measure, the preparatory gesture will be an outward movement (for a detailed review on the description of preparatory gestures in conducting handbooks, please see Platte et al., 2021).
In the 1980s, researchers began to explore the impact of conducting gestures on musicians. Sousa (1988) studied high school and university band members’ understanding of 55 conducting gestures. He discovered that not all conducting gestures are universally understood, and musicians need to learn them, which leads to increasing recognition rates with age and experience. Serrano (1993) analyzed the predictability of conducting gestures using light point animations, finding that gestures with increasing speed in downward movements are the most predictable. Luck and Sloboda (2007) used motion capture to study the synchronization between conductors and musicians, revealing that musicians with conducting experience achieved the best synchronicity, and synchronization decreased as tempo reduced. Only few studies investigated the conductor's gestural and mimical influence on singers. In her master's thesis, Stefan (2017) used a video grid overlay to measure the anterior abdominal expansion of teenage singers in reaction to two different preparatory gestures (one straight downward and one straight upward gesture), executed with the right arm. The participants (N = 30) were singing the song “America” by Samuel F. Smith and followed a prerecorded conducting video, showing the conductor's full body and breathing with open mouth. The results indicated no significant differences in abdominal expansion between the two conditions. A study by Manternach (2012) showed that the head and shoulder movements of choral singers changed while following different combinations of head, shoulder, and preparatory movements of the conductor. In a second study, the same author examined the muscle activity of several muscles of the singing apparatus and the “voicing behaviors” in response to different gestures and head movements of a conductor: an upward or downward moving arm, combined with upward moving or neutral head positioning and fisted hand or open palm. The results showed significant differences in muscle activity in the differing conditions and a higher amplitude of the tone in the fisted hand condition compared with the open palm condition (Manternach, 2016). In a recent study by us, we investigated whether the type of preparatory gesture has a direct measurable influence on the inhalation and tone production of choral singers (Platte et al., 2022). A total of 18 participants were asked to sing a tone in response to four different video stimuli. These consisted of two conducting videos with different preparatory gestures (Figure 1) and two control conditions with an animated bar. For the two conducting videos, the singers were asked to sing according to the conductor's gestural cues without any instruction concerning inhalation type or timing. In the case of the two animated stimuli, the singers were asked to use the inhalation type indicated by a yellow arrow (i.e., abdominal breathing ↓ or clavicular breathing ↑). We applied three-dimensional (3D) motion analysis to investigate the singers’ breathing behavior und recorded voice samples for audio analysis.

Still image of the conducting video of our previous study in start position with added movement-directions of the two distinct preparatory gestures (A and B).
The results of this study showed that the volume of the abdomen significantly differed between the two contrasting gestures, which could be validated by the control measurements asking participants for deliberately executed abdominal and clavicular breathing actions. An outward preparatory gesture (Figure 1 – gesture B) evoked an abdominal breathing type, while an inward-upward movement (Figure 1 – gesture A) elicited an inhalation with a higher portion of clavicular breathing. Furthermore, significant differences in timbre and loudness of the produced tone could be observed: Besides differences in formant frequencies, spectral flatness, and spectral spread, the maximum sound pressure level of the outward preparatory gesture was significantly higher than in case of the inward-upward movement.
However, in choral rehearsals, conducting gestures are usually combined with verbal instructions, for example, on the desired breathing technique. Hence, the combination of verbal breathing instructions with preparatory gestures – the latter intuitively elicit specific reactions in singers’ inhalation type – could lead to either congruent or incongruent task combinations. Existing research in the field of experimental psychology has shown that incongruent task combinations lead to longer processing times and a higher error rate (e.g., Fennell & Ratcliff, 2019; Grégoire et al., 2013; Stroop, 1935). The same effect could be observed in experiments including motor tasks. For example, Wexler and colleagues (Wexler et al., 1998) conducted an experiment where participants had to perform the Cooper-Shepard mental rotation task while simultaneously rotating a joystick in a given direction at a predetermined speed. The results showed a shorter response time and fewer errors in case of compatible rotation directions. In an experiment led by Zwaan and Taylor (2006), participants rated sentences describing hand rotations (e.g., “He turned down the volume”) by turning a knob either clockwise or counterclockwise. In the case of compatible rotation directions, that is, when the rotation described in the sentence matched their response rotation, participants responded more quickly. A similar stimulus-response compatibility approach is used exploring the phenomenon of automatic imitation (Heyes, 2011). In studies on this phenomenon, participants are asked to execute motor tasks (e.g., movements of fingers, hand, arm, or foot) while simultaneously observing videos or photographs of the same or a different action. Responses are reported to be faster and often more accurate and fluent in the case of compatible pairs (Brass et al., 2001; Kilner et al., 2003; Stanley et al., 2007; Stürmer et al., 2000). In a study by Bach and Tipper (2007), for example, participants executed either a foot or a finger-key-press action while watching a video of a person kicking a ball or typing on a keyboard. The results showed that actions are faster and more accurate when combined with videos of the same action-type.
In the light of these findings, the aim of the present study is to investigate whether observing a preparatory gesture while executing inhalation tasks elicits a similar stimulus-response compatibility effect. From our previous study we know that an outward preparatory gesture intuitively evokes an abdominal breathing type, while an inward-upward gesture elicits an inhalation with a higher portion of clavicular breathing. These findings lead to two congruent and two incongruent gesture-task-pairings to be tested in our experiment:
Abdominal Incongruent (AIn) = abdominal breathing + inward-upward gesture (gesture A) Abdominal Congruent (ACo) = abdominal breathing + outward gesture (gesture B) Clavicular Incongruent (CIn) = clavicular breathing + outward gesture (gesture B) Clavicular Congruent (CCo) = clavicular breathing + inward-upward gesture (gesture A)
Based on the reported research in experimental psychology (e.g., Bach and Tipper, 2007; Brass et al., 2001; Grégoire et al., 2013; Zwaan and Taylor, 2006), where incongruent pairs of tasks were found to delay the reaction time and lead to weaker results, we hypothesize to find reduced chest/abdominal wall expansion in the case of incongruent gesture-task combinations. Furthermore, we expect a delay of breathing action and onset in case of incongruent gesture-task combinations.
Methods
This study was part of a larger investigation that also measured other data, which have been published elsewhere (Platte et al., 2022).
Participants
Eighteen vocally and physiologically healthy choral singers (9 female/9 male, mean age 26.7 (SD 9.8)) participated in a laboratory experiment. The participants represented all main choral voice registers with seven sopranos, two altos, four tenors, and five basses. All participants were active singers in choirs led by a conductor, such as chamber choirs, symphonic choirs, and church choirs. The extent of prior experience in vocal training ranged from no voice training to voice lessons at a university; their choral experience ranged from less than 5 years as chorister through more than 20 years of choral experience. All participating singers were familiar with the required breathing types and were able to deliberately perform them. Prior to taking part in the study, all participants were informed about the purpose, procedures, and possible risks associated with the experiment and gave written informed consent.
Video Stimuli
During the laboratory experiment, each participant was asked to watch videos containing four different stimuli. Each stimulus consisted of a video of a conductor performing one of two different preparatory gestures: Gesture A displayed an inward-upward movement as used when a piece starts on beat 1, while gesture B was an outward movement exemplifying a start on beat 4 in a 4/4-piece. Both gestures had an ictus point but differed in form and direction of the trajectory, ending in an ensuing visual point of articulation. The degree of arm-stretching, the form and anatomic position (with regard to supination/neutral/pronation) of the hands, and the distance from the body and the starting point (measured from the floor) were identical. For gesture A, a fermata with a length of four seconds started on beat one; for gesture B on beat four. All video stimuli ended with a finishing gesture indicating the end of phonation. The conductor had a metronome for orientation during the recording to ensure exactly the same tempo for both conditions. The participants had no additional tempo information; they only saw the preparation gesture, fermata, and finishing gesture. To minimize possible influences on the participants’ reaction originating from the conductor's head movements, mimics, and chest movements during his own inhalation, the videos were modified in such a way that only the conductor's arms could be clearly seen. In addition to the shown gesture, a yellow arrow was projected on the conductor's chest (Figure 2), instructing the participant to either perform a clavicular inhalation (↑) or to breath abdominally (↓). These breathing instructions were then combined with the two different preparatory gestures, resulting in two pairs of stimuli: two clavicular inhalations (↑) combined with gesture A or B (Figure 2 – clavicular incongruent and clavicular congruent), and two abdominal inhalations (↓) combined with gesture A or B (Figure 2 – abdominal incongruent and abdominal congruent).

Still images of the four video stimuli including the yellow arrows on the conductor's chest indicating the demanded breathing type in each stimulus. The added trajectories of the conducting gestures are only shown here for clarification (in contrast to the yellow arrows, they were not part of the video stimuli).
Each video was composed as follows: At the beginning, a white screen triggered a light sensor for a synchronized start of data acquisition. Subsequently, the playback of two pure tones (D5 and A4) ensured the participants’ recalling of the pitch. After this, the participants were asked to fully exhale while watching an animated bar guiding the exhalation. The animated bar was filled with blue color mimicking the remaining amount of air in the lungs. From above, the black overlay increasingly covers the blue bar in a steady motion, thus animating the participant to fully exhale (for details see Platte et al., 2022). This step was needed to ensure that all participants had exhaled before the stimulus began. Subsequently, one of the four different stimuli (Figure 2) was shown.
Task
The participants were asked to inhale as indicated by the yellow arrow (i.e., abdominal breathing ↓ or clavicular breathing ↑) while following the conductor's preparatory gesture. After the inhalation, they were asked to sing a tone suitable to their voice register (Bass: A3, Tenor: D4, Alto: A4, Soprano: D5) on the vowel a [aː], accompanied by a fermata cue for four seconds, which was finished with a gestural cue.
Data Acquisition
For evaluation of the breathing behavior, chest wall kinematics were measured with the participants being seated in an upright position. Volumes of three different chest wall compartments (Figure 3 – AB, ARC, and URC) and areas of four different levels (Figure 3 – L1, L2, L3, L4) were assessed by a 3D motion analysis system with 12 cameras (Vicon Motion Systems, Oxford, UK). Thirty-seven reflective markers with a diameter of 14 mm were placed on the participants’ skin using double-sided fixing tape according to Massaroni et al. (2018). In addition to the measurements of chest wall kinematics, we attached two markers to the shoulders and three markers on the participants’ faces (right + left forehead and chin) in order to measure possible differences in shoulder height or mouth opening under the different conditions (Figure 2). The marker positions were recorded with a sampling frequency of 200 Hz and an accuracy of 0.017 mm. Vicon Nexus software (version 1.8.5, Oxford Metrics Ltd., UK) was used to assign labels to marker positions in a global coordinate system. Voice samples were recorded with a Tascam DR-680 Audio Recorder with two microphones (Stereo, 48,000 Hz, 32-bit).

Marker model seen from the front with 37 markers placed on face, shoulders, and chest wall.
Experimental Setup and Procedure
All experiments were conducted under consistent conditions in the same laboratory with identical setup and procedures for all participants. Each participant attended one session, reacting to 10 sets of videos each consisting of the 4 stimuli in randomized order to prevent order effects.
The experimental procedure is shown in the flow chart in Figure 4: Upon arrival, the participants were informed about the purpose, procedures, and possible risks associated with the experiment and provided written informed consent. After the placement of the reflective markers, the participants were seated on a stool without a backrest in an upright position with the arms hanging relaxed at the sides. While seated on a stool, they could not lean against a backrest and remained in the same upright position throughout the experiment, ensuring an easy control of the participants’ posture and thus stable conditions throughout the course of the experiment. Subsequently, the singers were introduced to the videos with detailed explanations of all parts (playback of the pure tones, guided exhalation, and the four different stimuli), and they could practice their reaction to the four stimuli (once for each stimulus) to get familiar with the procedure. Before the main experiment started, we asked each participant to perform two maximum voluntary inhalations (one abdominal and one clavicular inhalation) for normalization purposes to allow a comparison of different participants. Finally, the main experiment started, wherein the choristers watched and responded to the 10 sets of videos, each consisting of the four different stimuli.

Flow chart of the experimental procedure.
Data Analysis
All kinematic calculations were executed in MATLAB (The MathWorks R2018b). The kinematic trajectory data were low-pass filtered with a zero-phase fourth-order 8 Hz Butterworth filter. The optimal cut-off frequency of the filter was determined by a residual analysis (Winter, 2005, p. 49). Potential differences in mouth opening during inhalation were measured by calculating the distances between the midpoints between right and left forehead and chin. Volumes of the three compartments upper rib cage (URC), abdominal rib cage (ARC), and abdomen (AB), and areas of the four levels (L1–L4) were calculated for each stimulus through triangulation of the recorded coordinates and the use of Gauss's divergence theorem as demonstrated in Massaroni et al. (2018). All kinematic results (compartmental volumes and areas of L1–4) were then normalized according to the values of each participant's minimum and maximum voluntary inhalation, which was used to convert the results into values between 0% and 100%.
As for the audio analysis, we firstly calculated the onset-time and then discarded the first 500 milliseconds of each voice sample to avoid onset effects and used the subsequent 3 seconds for further analysis. We calculated the maximum and mean sound pressure levels of the sung tones in MATLAB using the MIR toolbox 1.7.2 (Lartillot et al., 2008) and Audio Toolbox 1.5 (The MathWorks R2021a). Overall, the collected data of 17 participants could be used for analysis. The audio data of one participant had to be discarded due to disturbing noise on the recording.
Statistical Analysis
This study was defined as a complete within-subject design with repeated measures on all experimental factors (condition and set). Data were analyzed using a 2 by 2 repeated measures analysis of variance (ANOVA) for all four conditions followed by Bonferroni corrected post hoc t-tests. The described repeated measures ANOVAs were performed to examine the differences in compartmental volume, area of the layers 1–4, mouth opening, and sound pressure level (Table 1) between the different conditions. For each statistical calculation, the measured value per stimulus served as the dependent variable. Additionally, we used Q-Q plots to determine if the data were normally distributed. For effect size measurements, we calculated partial eta-squared values, denoted as ηp2, for the repeated-measures ANOVA and Cohen's d for the post hoc t-tests. The level of significance was set at p < .05. The data were analyzed using SPSS (IBM version 27.0.1.0, 2020) and RStudio (version 1.3.1093).
Overview of the main parameters.

Results
Chest Wall Kinematics
An ANOVA of chest wall kinematics showed significant main effects for both breathing type and gesture. Significant interactions could only be observed for the compartmental volume ARC and the overall volume (Table 2). Post hoc tests show that differences between the clavicular conditions were only significant in the maximum area of Level 1 (T = 2.56, p < .02, Cohen's d = 0.62), the maximum volume of AB (T = 2.19, p = .044, Cohen's d = 0.53), and the overall volume (T = 2.66, p = .017, Cohen's d = 0.63), showing higher values for the Clavicular Incongruent condition in all three cases (Table 3). For the abdominal conditions, post hoc tests were significant for the areas of all levels as well as for all compartmental volumes. As shown in Figures 5 and 6, all measured areas and volumes were significantly higher in case of the Abdominal Congruent condition.

Dot plots with standard deviations showing the maximum volume of the three compartments and the total volume for the conditions Abdominal Incongruent and Abdominal Congruent, normalized to the maximum voluntary inhalation (n = 17). *p < .05.

Dot plots with standard deviations showing the maximum areas of level 1–4 for the conditions Abdominal Incongruent and Abdominal Congruent, normalized to the maximum voluntary inhalation (n = 17). *p < .05.
Overview of the statistical outcomes of the 2 × 2 ANOVA for all conditions (n = 17).

Overview of the descriptive statistics of all conditions (n = 17).

Figure 7 shows the mean change of total chest wall volume during inhalation and at the beginning of singing in all sets for all participants for the Abdominal Congruent condition (green line) and the Abdominal Incongruent condition (red line). Compared to the Abdominal Incongruent condition with a maximum value of 67.98%, the Abdominal Congruent condition not only reaches a significantly higher maximum value (74.68%), but the instant of the maximum is also reached earlier in case of the congruent condition, although the timing should be the same in both videos (see the two circles in Figure 7 indicating the moment of maximum expansion).

Mean change of total chest wall volume during inhalation and at the beginning of singing in all sets for all participants for the congruent abdominal condition (green line / SD shaded in light green) and the incongruent abdominal condition (red line / SD shaded in light red), normalized to the maximum voluntary inhalation (n = 17). The two circles indicate the moment of maximum expansion in each condition. The two vertical lines show the beginning of the preparatory gesture (solid line) and the start of the fermata (dashed line).
Mouth Opening
For the maximum amount of mouth opening during inhalation, a significant main effect of gesture (F1,17 = 33.69, ηp2 = 0.68, p < .001) and an interaction effect between gesture and breathing type (F1,17 = 29.33, ηp2 = 0.65, p < .001) could be observed. Post hoc tests revealed that the maximum amount of mouth opening during inhalation does not differ significantly in case of the clavicular conditions, but a nearly 12% bigger opening (T = −7.33, p < .001, Cohen's d = −1.78) could be measured in the Abdominal Congruent condition compared with Abdominal Incongruent (Figure 8).
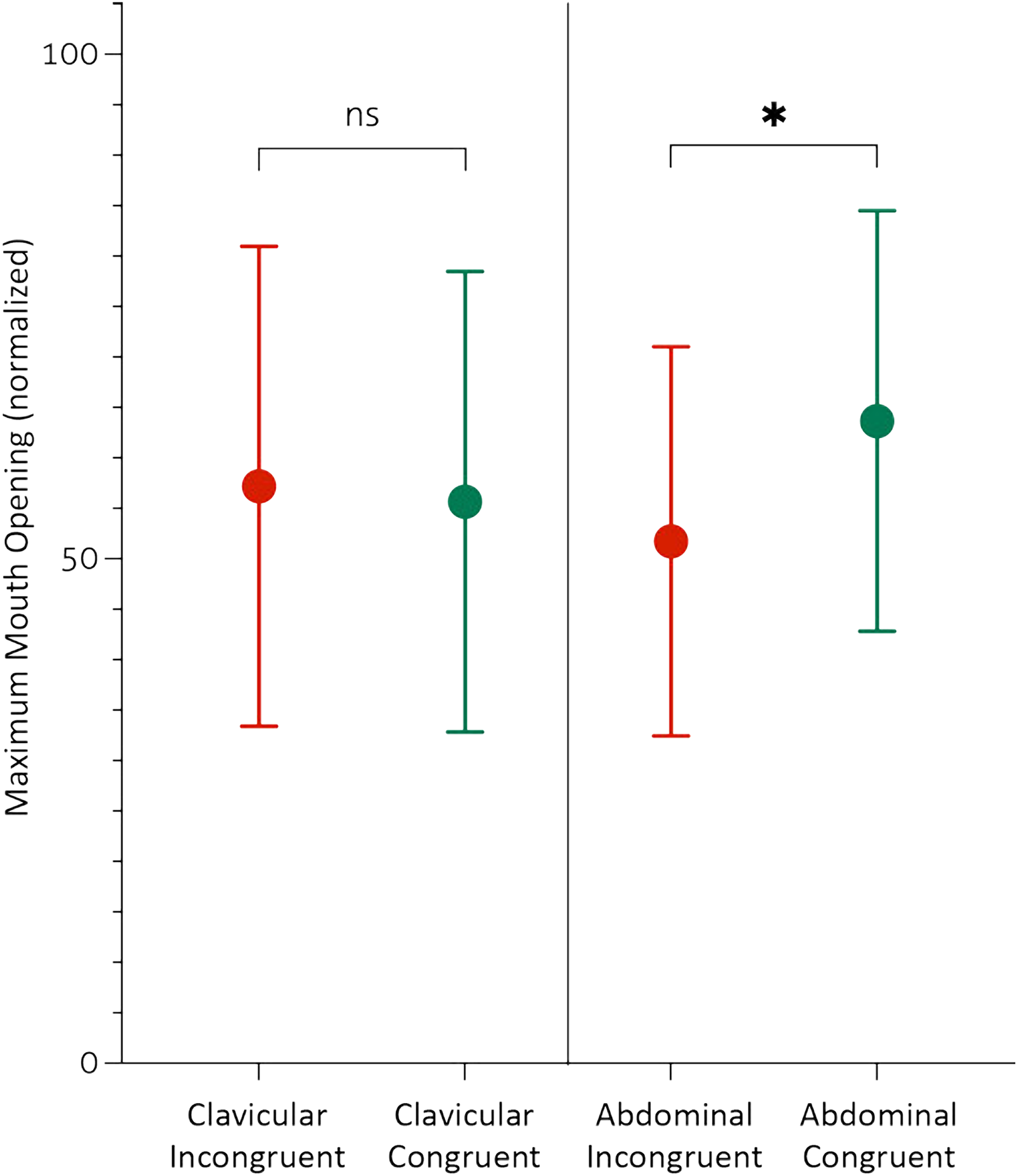
Dot plots with standard deviations showing the maximum mouth opening for both pairings of conditions, normalized to the maximum values during voluntary inhalation (n = 17). *p < .05, ns = not significant.
Onset-Time
In order to compare potential differences in the onset of the sung tone, we compared the combination of each preparatory gesture with the two breathing tasks. The onset time in the case of the inward-upward movement was significantly delayed by 20 ms (T = 3.21, p = .006, Cohen's d = 0.8) in the case of the incongruent combination (Abdominal Incongruent condition), while there was no significant difference for the outward-movement in combination with both breathing tasks.
Sound Pressure Level
The results of the measurements of mean and maximum sound pressure level showed a significant main effect of gesture and a significant interaction effect (Table 4). Both inhalation types elicited significantly higher mean and maximum sound pressure levels (Table 5 / Figure 9) when combined with the outward preparatory gesture (Table 6). The highest maximum and mean sound pressure levels resulted from the Abdominal Congruent condition – the maximum value was on average 2 dB higher than in the incongruent condition; the differences in mean sound pressure level were even higher at 5.5 dB, resulting in an audibly louder tone.

Dot plots with standard deviations showing the mean and maximum sound pressure levels in dB for both pairings of conditions (n = 17). *p < .05.
Overview of the statistical outcomes of the 2 × 2 ANOVA for all conditions (n = 17).

Overview of the descriptive statistics of all conditions (n = 17).

Results of the post hoc tests for mean and maximum sound pressure levels for both pairings of conditions (n = 17).

Discussion
The aim of this study was to explore possible effects of congruent and incongruent gesture-task combinations on the breathing behavior and tone quality in choral singers. From our previous study, we know that an outward preparatory gesture intuitively evokes an abdominal breathing type, while an inward-upward movement elicits an inhalation with a higher portion of clavicular breathing (Platte et al., 2022). Based on these findings and the reported research in experimental psychology where incongruent pairs of tasks were found to delay the reaction time and lead to weaker results, we combined different breathing tasks with the two preparatory gestures to create two congruent and two incongruent gesture-task-pairings to be tested in our experiment. These pairings led us to hypothesize a weaker specificity of the demanded inhalation type in the case of an incongruent gesture-task combination and a delay of breathing action and onset in the case of incongruent gesture-task combinations.
Chest Wall Kinematics and Mouth Opening
Our hypothesis of a constraining effect of incongruent gesture-task combinations on the chest wall expansion could only be seen in the case of the abdominal breathing task. There, the maximum volume of all three compartments as well as the maximum areas of level 1–4 showed significantly lower values in the case of the incongruent gesture (Figure 1 – Gesture A). The inward-upward movement seems to restrain the singers’ overall inhalation, resulting in a loss of 6.7% in total volume. For the clavicular breathing task, the only significant difference could be measured in the maximum values of Level 1, showing even higher values for the incongruent condition (outward movement). Although the outward movement does not intuitively evoke a clavicular breathing type, it still does not constrain the desired clavicular breathing and even led to an increased expansion in the upper thorax (level 1). A possible explanation might be that the upward-inward preparatory gesture resembles a narrowing of the thorax, while the outwards gesture encourages a widening of the rib cage, thus leading to a bigger expansion during the breathing action.
Similar results can be found in the degree of mouth opening, which did not get affected by the outwards gesture when combined with a clavicular breathing type. However, significant differences appeared for the abdominal breathing task, with a 12% smaller mouth opening in combination with the upward-inward preparatory gesture. It seems that the constraining nature of the upward-inward preparatory gesture does even influence the amount of mouth opening in the case of the Abdominal Incongruent condition. The smaller mouth opening might also have caused the slower intake of air as seen in Figure 7.
Onset Time
The hypothesized delay of breathing action and onset in the case of incongruent gesture-task combinations could only be confirmed in the case of the abdominal condition. The incongruent combination of inward-upward preparatory gesture with abdominal breathing caused a delay not only of the breathing action (Figure 7) but also of the onset time, which was significantly delayed by 20 ms. In contrast, the outward gesture did not cause a delay when combined with a clavicular breathing type, and also the onset time did not differ significantly. This lack of delay supports our assumption that the outward gesture does not have a constraining effect on clavicular breathing, while the inward-upward preparatory gesture interferes with abdominal breathing, leading to a delayed reaction of inhalation and onset. The observed delay in incongruent gesture-task combinations could be explained by dual-route models (Heyes, 2011). These models assume that there are two routes through which responses can be activated: an intentional route and an automatic route. If both routes activate the same response, such as in the case of congruent combinations of gesture and task, the execution happens very fast. However, in case of incongruent gesture-task combinations, the automatic route must be inhibited in order to ensure the execution of the correct task, which prolongs the response time.
Sound Pressure Level
Similar to the observed effects on the chest wall kinematics, the outward preparatory gesture turns out to generally elicit a significantly higher sound pressure level than the inward-upward gesture. Although the highest mean and maximum sound pressure levels appeared in the Abdominal Congruent condition, the resulting loudness in the case of the Clavicular Incongruent condition also was significantly higher than the sung tones of the Clavicular Congruent condition. These results support our observation that the outward gesture does indeed influence but not constrain the use of a clavicular breathing type.
Limitations
To provide a stimulus that shows the isolated gesture without mimics and further body language (such as the conductor’s own breathing movement) and to ensure identical stimuli for all participants, we used prerecorded video stimuli for our experiment; thus the presented conducting stimuli did not appear at life size. This non-live presentation on video combined with the size reduction due to the video screen might have reduced rather than amplified the reactions of the participants. A conductor in a live setting would probably have elicited stronger effects, but the comparability would be highly questionable, and masking of mimics and other perturbing aspects of body language would probably have been impossible. Furthermore, the laboratory setting with sensors attached to the participants does not resemble the usual environment in which choral singing takes place and might have had constraining effects on the singers.
Conclusions
To the best of the authors’ knowledge, in the existing conducting literature, preparatory gestures are mostly dependent on the applied beat pattern, and inhalation techniques are – if they are mentioned at all – described separately. Therefore, possible effects of incongruent gesture-task pairings are not discussed. However, our study shows that there is an influence of the used preparatory gesture on the predetermined inhalation type – in particular, the most commonly used inward-upward gesture results in a reduced chest wall expansion and reduced loudness of the resulting tone when combined with an abdominal inhalation. Inhalation and onset are delayed, as well. Of course, greater inhalation and volume are not always desired; in some cases a conductor might for musical reasons even wish to elicit an inhalation with, for example, a higher portion of clavicular breathing. Nevertheless, for choral practice it is essential to generally consider that the selected gesture has an influence on the resulting sound and hence should be chosen with respect to the desired type of inhalation.
As players of wind instruments also depend directly on the type of inhalation used, future studies could explore whether our findings are relevant for orchestral practice as well. Acknowledging that this study deals with only the very first constituent in a long chain of communication between conductor and ensemble, future research should examine whether the presumed general gestural influence on tone production and quality also has consequences for the overall interpretation.
Footnotes
Acknowledgements
We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Action Editor
Youn Kim, The University of Hong Kong, Department of Music.
Peer Review
Steven Morrison, Northwestern University, Center for the Study of Education and the Musical Experience; One Anonymous Reviewer
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the University of Freiburg (No. 250/19).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.