
Abstract
In this article we discuss the various options available to musicians wanting to treat their music performance anxiety (MPA), and we recommend that musicians work with a performance psychologist over the other available options. We also discuss the potential for Acceptance and Commitment Therapy (ACT) to serve as both a clinical anxiety treatment and performance enhancement program for musicians, while addressing the state of the research for both applications, as well as the research for a similar, mindfulness and acceptance-based performance enhancement program for athletes, i.e., the Mindfulness–Acceptance–Commitment (MAC) approach. In order for the field of performance psychology to develop into a more credible discipline, we believe practitioners working with musicians should follow an evidence-based practice model of care, in which empirically supported treatments for MPA and performance enhancement are promoted, and information about such treatments is disseminated among practitioners, musicians, and music teachers. Such a practice must become the norm in this field, because it will ultimately result in greater protections for those musicians seeking help for performance-related challenges by ensuring a higher level of professional accountability among practitioners. Lastly, we discuss some issues that may arise when applying ACT or the MAC approach to musicians.
Keywords
Common treatment options for musicians with performance anxiety
When a musician struggles with performance anxiety or with other aspects of their performance, or wants to enhance their overall performance skills, what are the available options for help and how does one find them? This article will attempt to address these essential concerns, and in doing so will promote a newer therapy, Acceptance and Commitment Therapy (ACT), as a possible tool for the musician to use.
Music performance anxiety (MPA) is defined as “the experience of persisting, distressful apprehension about and/or actual impairment of, performance skills in a public context, to a degree unwarranted given the individual’s aptitude, training, and level of preparation” (Salmon, 1990, p. 3). In its more debilitating forms, MPA manifests as a multi-sided clinical problem including cognitive symptoms (worry and apprehension, narrowed attention onto perceived threats) physiological symptoms (shallow breathing, heart palpitations, tachycardia, dry mouth, increased physical tension, shaky hands and feet, tightness in the chest, etc.), behavioral avoidance (avoiding auditions, avoiding soloing, avoiding more challenging repertoire, avoiding drawing attention to one’s self, etc.), and subjective distress and/or occupational or professional impairment related to the MPA (Juncos et al., 2017). Although no standalone diagnosis of MPA exists within the Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5: American Psychiatric Association, 2013), it is included within the Social Anxiety Disorder diagnosis. This diagnosis specifies a person must have either social interaction anxiety or anxiety related to performing in front of others, or both, as its first symptom criteria (American Psychiatric Association, 2013).
When it comes to treatments for music performance anxiety (MPA) many options exist. Most commonly, as many as 30% of professional musicians make use of beta-adrenoceptor blocking medications, or “beta-blockers”, to reduce the physiological sensations associated with MPA such as palpitations, hyperventilation, and shakiness, e.g., Propanolol, Nadolol (Kenny, Driscoll, & Ackermann, 2012). Also common is Cognitive Behavioral Therapy (CBT), a popular form of psychotherapy that has been shown to effectively treat mild to moderate cases of MPA (Clark & Agras, 1991; Braden, Osborne, & Wilson, 2015; Osborne, Kenny, & Cooksey, 2007). Psycho-dynamically oriented therapy has shown promise with more severe forms of MPA with accompanying depression (Kenny, 2016; Kenny, Arthey, & Abbass, 2014, 2016; Kenny & Holmes, 2015). Alternatively, there are numerous other therapies that fall into two basic categories: (1) treatments that promote relaxation and improved physical health, such as biofeedback (Thurber, Bodenhamer-Davis, Johnson, Chesky, & Chandler, 2010), hypnosis (Stanton, 1994), yoga (Khalsa, Shorter, Cope, Wyshak, & Sklar, 2009), meditation (Lin, Chang, Zemon, & Midlarsky, 2008), progressive muscle relaxation (Kim, 2008), and the Alexander Technique (Valentine, Fitzgerald, Gorton, Hudson, & Symonds, 1995); and (2) expressive arts therapies, such as music therapy (Montello, Coons, & Kantor, 1990) and guided imagery (Esplen & Hodnett, 1999). Given these therapies and more, a musician with MPA would likely feel confident in finding help. However, when deciding which option to go with one may discover the numerous hurdles that complicate the process.
To start, musicians with MPA may seek help from a mental-health therapist. However, this option is quite uncommon among professional musicians (Kenny et al., 2012). There are several likely reasons for this. Practical considerations limit the ease with which some MPA treatments are administered. For example, hypnosis, music therapy, biofeedback, and the Alexander Technique each require certification to be properly administered, a condition that inevitably lowers the number of available therapists. Biofeedback also involves the use of costly equipment (Schneider, 1987), and music therapy is limited to settings where its use is appropriate, i.e., places where music can be played at moderate volumes (Bunt, 1994). Furthermore, an online search for psychotherapists specializing in performance anxiety treatment using popular American websites (e.g., www.psychologytoday.com, www.goodtherapy.org) produces few to no results. However, when one broadens the search criteria to include therapists who treat anxiety there are numerous clinicians who do not advertise that they work with musicians. This is undoubtedly frustrating for musicians looking to find an MPA therapist, and it may reinforce any existing hesitation to attend therapy.
A more inquisitive musician may turn to MPA treatment research to seek a practitioner trained in the most effective treatment options, but they may discover the numerous methodological shortcomings found in MPA treatment research. Such limitations not only prevent competent MPA therapists from making informed decisions about which interventions will be most effective, they also prevent information about best practices from being disseminated to musicians in need of help. Examples of these include a lack of studies with well-controlled designs, lack of treatment manuals, lack of objective MPA assessment, lack of a full battery of assessments, and few follow-up assessments (McGinnis & Milling, 2005). For more information on the limitations of MPA treatment research, and for a more comprehensive review of MPA therapies, the reader is directed to Dianna Kenny’s seminal work (Kenny, 2005, 2011).
In order to develop into a more credible resource for musicians seeking help, MPA treatment research (and performance psychology research) must improve its methodology so that it abides by the standards for evidence-based practice set forth by the American Psychological Association’s (APA) Division 12 Task Force, in Clinical Psychology, in particular regarding the promotion and dissemination of empirically supported treatments in psychological research (Chambless & Hollon, 1998). According to these standards, a therapy meets criteria for a “well-established” treatment when research supporting it includes either (1) at least two independently conducted and well-designed experiments showing superiority to pill, placebo, or another treatment, or equivalency to an already established treatment with adequate sample sizes (N ≈ 30), or (2) a large series of well-designed and carefully controlled single-case experiments (N > 9), in which the intervention is compared to another treatment as in the previous condition (Chambless & Hollon, 1998). Treatments that meet this standard are those with the highest level of empirical support. Such standards are not overly difficult to meet, yet only one of the aforementioned treatments meets them: CBT with exposure. For that reason it is considered best practice for MPA treatment (Kenny, 2011). It is important to note that the rest of the aforementioned MPA treatments are not yet well-established and are considered either “probably efficacious”, or “promising interventions”, because they have less empirical support, i.e., they have yet to show efficacy according to the standards listed above. Going in order of decreasing empirical support, a therapy is considered “probably efficacious” when it meets all criteria for a well-established treatment, except that its experiments were not conducted by at least two different investigators, or that its experiments found the therapy to be superior to a wait-list control condition only (Chambless & Hollon, 1998). Lastly, a therapy is considered a “promising intervention” when it is supported by the results of one well-controlled study or by a small (N > 3) series of single-case designs (Chambless & Ollendick, 2001).
Alternatively, musicians with MPA may turn to a medical provider for help. Beta-blockers are by far the most common of the aforementioned MPA treatments among orchestral musicians (Kenny et al., 2012). Taken in low doses, they effectively lower physiological MPA symptoms, but unwanted side effects may make them unhelpful for certain musicians. For example, they are not recommended for musicians with heart conditions and asthma due to interference with bronchodilation (Kenny, 2011), and other researchers caution against their use with singers and wind-instrumentalists, due to a loss of effective respiratory exertion (Sataloff, Rosen, & Levy, 2000). Higher doses may create difficulty in connecting emotionally with one’s music or in actual impairment in performance ability (Gates et al., 1985; Nube, 1991). Furthermore, beta-blockers do not directly target cognitive and emotional symptoms of MPA, so musicians whose MPA is expressed mainly by those symptoms cannot expect to benefit much (Kenny, 2011). It is imperative that a medical provider be aware of these shortcomings before prescribing beta-blockers, or other medications, to treat MPA. Lastly, the reader should know that treatment with beta-blockers is only probably efficacious, because the majority of studies investigating their efficacy do not include random assignment (Brugués, 2009), nor do they use adequate sample sizes or provide participants with objective MPA evaluations prior to inclusion (Kenny, 2011).
Musicians may also turn to their professors or to trusted colleagues for help managing their MPA. According to the National Association of Schools of Music, students attending any of the 650+ accredited undergraduate music schools in the United States must be provided with psychological treatment (or be given access to it), which may include therapeutic management of MPA (National Association of Schools of Music, 2017). Additionally, students may turn to a professor with knowledge of MPA treatment for help. Some music schools even invite leading MPA experts to give brief workshops so that treatment information may be disseminated to numerous students at once (Jordan, 2016). However, there are no studies examining the effectiveness of consulting with either one’s professor(s) or with an MPA expert, therefore it is unknown how helpful either practice is. Orchestral musicians sometimes lack access to information on managing MPA and other psychological problems and may rely more on consultation with trusted colleagues or on self-initiated methods. Occasionally, colleagues may recommend the use of beta-blockers without medical supervision, which greatly reduces their effectiveness compared to taking them with medical supervision (Fishbein, Middlestadt, Ottati, Strauss, & Ellis, 1988; Kenny et al., 2012). When considering the limitations of beta-blockers, it is no wonder orchestral musicians frequently turn to self-initiated methods to manage their MPA, such as increased practice, deep breathing, use of positive affirmations, and relaxation techniques (Kenny et al., 2012). Similarly, there is also a lack of well-designed studies that confirm the effectiveness of these methods in managing MPA.
Another option is to work with a psychologist who has a proficiency in sport/performance psychology earned either during or after their doctoral education. This proficiency has been recognized by the APA since 2003, and the APA provides standards for guiding appropriate training for psychologists wanting to practice sport/performance psychology (American Psychological Association, 2017). Sport/performance psychologists are trained to help athletes and performers in a variety of important ways, including diagnosing and treating common psychological problems such as performance anxiety, enhancing performance quality through mental skills training (i.e., goal setting, imagery, self-talk modification, and arousal control), conducting research on issues relevant to performance psychology, and promoting health and well-being (Weinberg & Gould, 2015). Though sport/performance psychologists work primarily with athletes, their specialized knowledge and skills may be transferable to work involving musicians and other performing artists due to the overlap between the domains of sports and performing arts (Clark & Williamon, 2011; Daubney & Daubney, 2017; Hatfield, 2016; Kageyama, 2007; Osborne, Greene, & Immel, 2014; Pecen, Collins, & MacNamara, 2016). For that reason, we believe a sport/performance psychologist would be the most qualified type of MPA practitioner of the options considered heretofore. This is especially possible if the psychologist graduated from a clinical or counseling psychology doctoral program, because they would have been trained to effectively treat anxiety disorders, including those similar to MPA such as Social Anxiety Disorder.
Sport/performance psychologists are also easier to find online than psychotherapists or physicians who treat MPA. The previously named webpages for finding therapists include categories such as “sports performance” and “sport/fitness psychology”, and searches with those terms yield more results than searches for psychotherapists who specialize in MPA treatment. Additionally, the Association for Applied Sport Psychology’s webpage includes an international search engine for sport psychology practitioners and a downloadable guide for selecting the right practitioner (www.appliedsportpsych.org). For the sake of simplicity (and to avoid misleading the reader), sport/performance psychologists will be referred to as “performance psychologists” hereafter. It should be noted, though, while performance psychologists are classified online as sport psychologists, there are important differences between the types of issues confronting athletes and musicians – for examples, see de Paiva e Pona (2015) and Pecen et al. (2016). Therefore, it is recommended that musicians make sure performance psychologists have adequate experience in either MPA treatment or performance enhancement work with musicians, or both.
Towards an evidence-based practice model for the treatment of MPA
What is ACT?
In accordance with the APA’s call for promoting and disseminating information about empirically supported treatments, we now provide information about Acceptance and Commitment Therapy, a newer therapy the performance psychologist should consider investigating further with musicians due to increasing research support for its effectiveness as an anxiety treatment. In doing so we will describe its theoretical underpinnings and objectives while also addressing research supporting it specifically as an MPA treatment.
Acceptance and Commitment Therapy, or “ACT” (pronounced as a word, not individual letters) is part of the “third-wave” of behavioral therapies that have become popular in the past 20 years (Hayes, Strosahl, & Wilson, 1999, 2011). Others in this group include Dialectical Behavioral Therapy (Linehan, 1993), Mindfulness-Based Cognitive Therapy for Depression (Segal, Williams, & Teasdale, 2002), and Metacognitive Therapy (Wells, 2009). Generally speaking, third-wave therapies are considered mindfulness and acceptance-based therapies because they teach clients to view unwanted internal experiences for what they are, i.e., thoughts, emotions, sensations, etc., rather than viewing them as what our minds tell us they are, i.e., problematic experiences to be eliminated or avoided (Hayes, 2004). Thus, rather than teach clients to change the content of their internal experiences, as they learn to do in CBT, third-wave therapies such as ACT teach clients to mindfully observe those internal experiences without changing them. Such a goal is in contrast to one of CBT’s main therapeutic tasks, cognitive restructuring (CR), in which clients are taught to change their thoughts so they are more rational and less distorted, because that will presumably lead to an improved mood (Kahl, Winter, & Schweiger, 2012). However, research examining the effectiveness of cognitive restructuring has shown that disengaging from one’s thoughts while doing CR tasks may actually be more closely related to the improvements in mood (Teasdale et al., 2002). This finding is consistent with the perspective third-wave therapies take in teaching how best to relate to our internal discomfort.
ACT is rooted in philosophical as well as behavioral models. At the foundation of ACT is the philosophy of functional contextualism, which emphasizes the importance of context in determining the function of a behavior (Hayes et al., 2011). Within an unaccepting context, unwanted internal experiences are viewed problematically and function in a manner that interferes with one’s quality of life. However, if a more accepting context is created in which those same experiences are not viewed problematically, but instead as unfortunate parts of life, they no longer function in the same toxic manner. Therefore, ACT clinicians teach clients to adopt a more accepting view of their unwanted internal experiences, so that vital resources such as time and energy can be put towards important pursuits like achieving valued goals (Harris, 2008). ACT was also born out of behavioral models, i.e., Relational Frame Theory (RFT) and Applied Behavioral Analysis (ABA; Hayes et al., 2011). Together, these models help clients untangle themselves from unskillful use of language and cognition and introduce behavioral responses that are more workable and consistent with one’s values, respectively (Harris, 2008).
The goal of an ACT therapy is unique. It does not strive for reduction of unwanted internal experiences, rather, it teaches psychological flexibility in the presence of those experiences. Psychological flexibility refers to the ability to repeatedly persist with valued behavior despite the presence of unwanted internal experiences. Such flexibility is achieved through the promotion of six behavioral processes, collectively known as the “ACT Hexaflex” (Hayes et al., 2011). These are contact with the present moment (mindfulness), acceptance of one’s unwanted internal experiences, cognitive defusion, cultivating a transcendent sense of self, identification of one’s values, and commitment to action consistent with values (see Figure 1). Cognitive defusion refers to the learned ability to become less reactive to one’s unwanted internal experiences, and cultivating a transcendent sense of self refers to viewing one’s self as more contextually defined rather than being defined by the content of one’s internal experiences (Hayes et al., 2011). Every ACT therapy is designed to improve psychological flexibility by identifying and reducing dysfunctional behaviors aimed to control or reduce unwanted symptoms, highlighting the unworkability and limiting nature of those dysfunctional behaviors, creating a more accepting context through which to experience unwanted symptoms, and introducing more skillful, functional responses to unwanted symptoms that are consistent with one’s values.

The ACT hexaflex.
State of the research supporting ACT as an MPA treatment
While CBT with exposure was recently deemed best practice for MPA (Kenny, 2011), ACT has become a well-established treatment for Social Anxiety Disorder more recently (Levin, Herbert, & Forman, in press). The results of two randomized controlled trials (RCTs) have independently shown ACT outperformed control and was equally effective as CBT in treating social anxiety symptoms (Craske et al., 2014; Kocovski, Fleming, Hawley, Huta, & Antony, 2013). Participants who received either 12 weeks of group ACT (N = 53) or CBT (N = 53) scored significantly better than participants in the wait-list control group (N = 31) on measures of social anxiety symptoms, and no significant differences were found between the two treatments (Kocovski et al., 2013), whereas participants who received 12 weeks of individual ACT (N = 34) or CBT (N = 40) also significantly outperformed wait-list control participants (N = 26) on measures of social anxiety, again with no significant differences between the two treatments (Craske et al., 2014). Furthermore, a recent meta-analysis of 39 RCTs involving ACT concluded it is equally effective as established treatments, including CBT, in treating anxiety disorders in general (A-Tjak et al., 2015). In light of this meta-analysis’ findings, and because MPA is technically included in the diagnosis of Social Anxiety Disorder (American Psychiatric Association, 2013), we argue ACT has the potential to meet the criteria for a well-established therapy for MPA. However, further research is obviously needed, because ACT has yet to be compared to CBT as an MPA treatment in two well-designed studies or in a large series of single-case designs. There are key differences between Social Anxiety Disorder and conditions derived from it, like MPA (for examples see Kenny, 2011), which is likely why ACT researchers have begun investigating its efficacy in treating other derivatives of Social Anxiety Disorder, i.e., public speaking anxiety (Block, 2002; England et al., 2012; Glassman et al., 2016), test anxiety (Brown et al., 2011), and sport performance anxiety (Watson, 2008).
Juncos and colleagues have conducted two single-case experiments and a pilot study in which ACT was compared to baseline control as an MPA treatment; the participants were a professional drummer (Juncos et al., 2014), an undergraduate violinist (Juncos & Markman, 2015), and seven vocal students from an elite choir college (Juncos et al., 2017). A similar methodology was used in all studies for recruitment of participants, including a thorough evaluation of MPA symptoms, a clinical interview for anxiety and other disorders using the Structured Clinical Interview for DSM-5 Disorders (First, Williams, Karg, & Spitzer, 2015), and the use of validated self-report measures of MPA and ACT-related processes. Treatment in each study followed an ABA design, which included establishing participants’ baseline functioning with self-report measures, 10–12 individual therapy sessions using an established treatment manual, i.e., ACT for Anxiety Disorders (Eifert & Forsyth, 2005), and follow-up assessment(s). The next section includes more information about specific treatment components.
The results from all studies showed every participant demonstrated clinically significant improvement in at least one Hexaflex process, i.e., defusion, at post treatment and follow up (see Table 1 for scores on the Believability of Anxious Feelings & Thoughts scale, “BAFT”). In other words, all nine participants effectively learned to be less fused with (less reactive to) their MPA-related thoughts while performing. Here, significance is defined according to any one of Kazdin’s (2011) multiple criteria for determining clinically significant change in single-case designs: (1) the client’s post-treatment score on a self-report measure has changed in a healthy direction by at least two standard deviations from the pre-treatment score, (2) the client’s pre-treatment score fell within an unhealthy range but was no longer in that range at post treatment, or (3) the post-treatment score falls below a clinical cutoff score on a validated self-report measure used to aid in the diagnosis of a disorder. The majority of participants also became significantly more accepting of their MPA-related thoughts and physiological sensations at post treatment and at follow up (Table 1, data from the Philadelphia Mindfulness Scale, “PHLMS, Acceptance Subscale”). Furthermore, significant reductions in MPA were found after Hexaflex improvements were observed for the majority of participants (Table 1, data from the revised Kenny Music Performance Anxiety Inventory, “KMPAI”). Such results are significant for two reasons. First, they support current thinking that defusion from and acceptance of unwanted internal experiences are two proposed mechanisms by which ACT treatments increase psychological flexibility (Ciarrochi, Bilich, & Godsell, 2010). They also support a consistent finding in ACT treatment studies: changes in psychological flexibility are likely to precede reductions in clinical symptoms, without being correlated with or a consequence of them (Ciarrochi et al., 2010; Gloster et al., 2017). In other words, it is common for symptom reduction to occur in ACT studies involving both clinical and non-clinical samples, though that is not the explicit goal, and those symptom changes typically occur after improvements in psychological flexibility are noticed (Bach & Moran, 2008; Ciarrochi et al., 2010). A visual inspection of Table 1 shows significant improvements in defusion and acceptance occurred approximately midway through all studies, whereas significant decreases in MPA were observed during the follow-up assessments.
Self-report measures assessing levels of cognitive fusion (via total scores on the Believability of Anxious Feelings & Thoughts [BAFT] scale), acceptance (Philadelphia Mindfulness Scale, [PHLMS, Acceptance Subscale] scores), and music performance anxiety (MPA) (Kenny Music Performance Anxiety Inventory [KMPAI] total scores) taken from nine participants across three studies investigating Acceptance and Commitment Therapy (ACT) as a treatment for MPA.
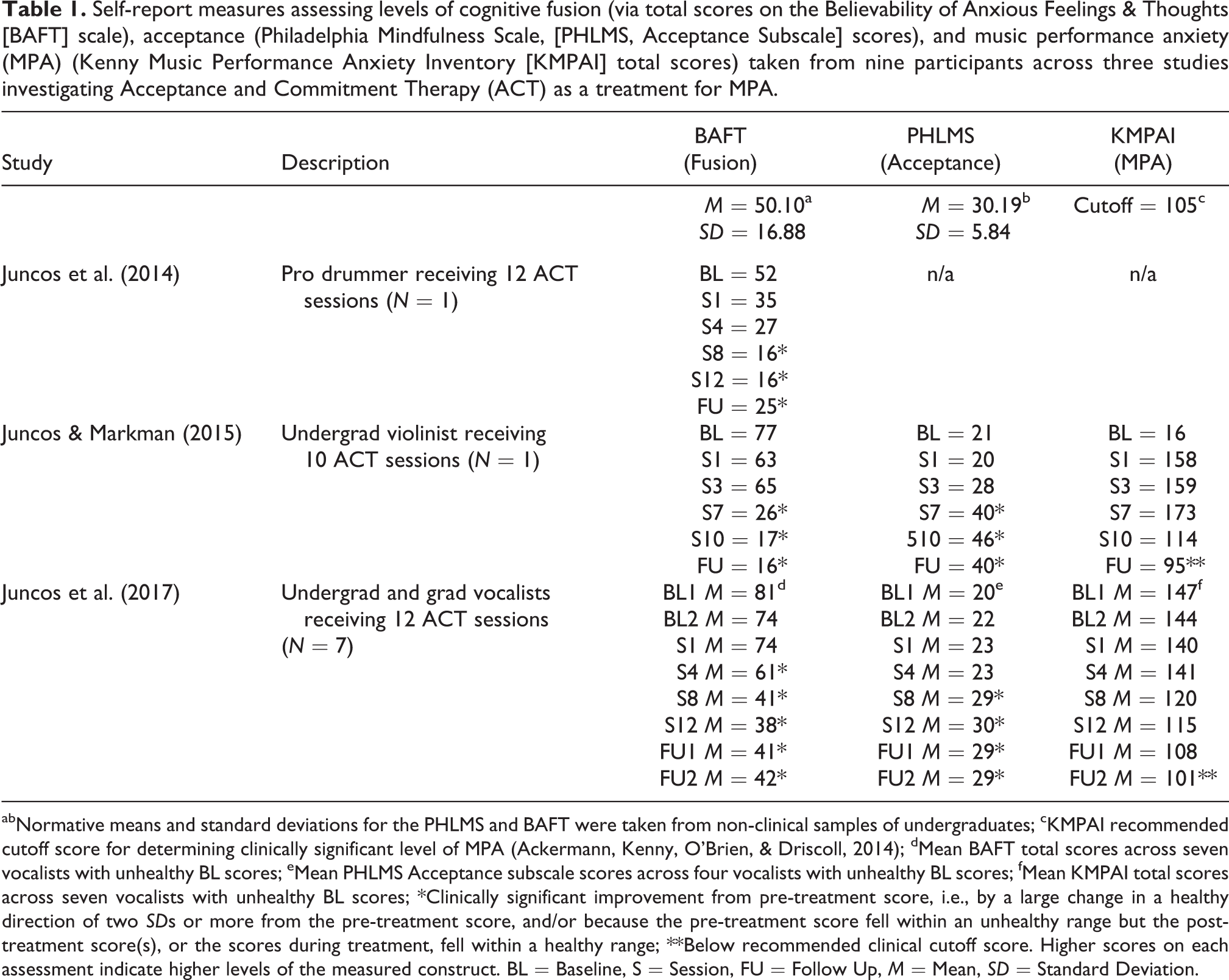
abNormative means and standard deviations for the PHLMS and BAFT were taken from non-clinical samples of undergraduates; cKMPAI recommended cutoff score for determining clinically significant level of MPA (Ackermann, Kenny, O’Brien, & Driscoll, 2014); dMean BAFT total scores across seven vocalists with unhealthy BL scores; eMean PHLMS Acceptance subscale scores across four vocalists with unhealthy BL scores; fMean KMPAI total scores across seven vocalists with unhealthy BL scores; *Clinically significant improvement from pre-treatment score, i.e., by a large change in a healthy direction of two SDs or more from the pre-treatment score, and/or because the pre-treatment score fell within an unhealthy range but the post-treatment score(s), or the scores during treatment, fell within a healthy range; **Below recommended clinical cutoff score. Higher scores on each assessment indicate higher levels of the measured construct. BL = Baseline, S = Session, FU = Follow Up, M = Mean, SD = Standard Deviation.
Potential advantages and disadvantages of ACT as an MPA treatment
Given that the research of Juncos and colleagues currently meets criteria for a promising intervention for MPA with university musicians (Juncos et al., 2017; Juncos & Markman, 2015), and given that ACT has recently become a well-established therapy for Social Anxiety Disorder, we believe ACT has the potential to be best practice in treating mild to moderate cases of MPA, along with CBT. However, both treatments will need to be compared to one another before this claim is confirmed.
ACT may offer some potential advantages over CBT as an MPA treatment. Clients may prefer ACT, because it has shown the potential to improve behavioral performance more than CBT in recent anxiety treatment studies, i.e., with improvements in test performance reported by Brown and colleagues (2011) and improvements in observer-rated public speaking skills reported by both Block (2002) and Glassman and colleagues (2016). In fact, a new study by Herbert and colleagues (2017) showed patients with Social Anxiety Disorder who received 12 individual ACT sessions demonstrated greater improvements in observer-rated social skills than patients receiving 12 individual CBT sessions, despite equal amounts of exposure. In contrast, patients in the CBT group showed greater improvements in clinician-rated and self-reported social anxiety symptoms. Such a finding is consistent with those of the previous studies (Block, 2002; Brown et al., 2011; Glassman et al., 2016) and highlights a possible key difference in outcomes for CBT and ACT treatments: that CBT effectively reduces symptoms and ACT effectively improves behavioral performance (Herbert et al., 2017). This distinction between symptom and behavioral outcomes is potentially very important for musicians with MPA looking for the right treatment – they may prefer a therapy that effectively improves their performance skills (like ACT) over one that effectively reduces anxiety symptoms (like CBT). Moreover, this distinction could also explain why CBT with exposure has not lead to significant improvements in performance quality in some MPA treatment studies, despite significant reductions in MPA symptoms (Braden et al., 2015; Osborne et al., 2007).
Another advantage ACT has over other MPA therapies, including CBT, is that information about it is accessible on the webpage for its affiliated association, the Association for Contextual Behavioral Science (www.contextualscience.org). This webpage includes information about ACT’s theoretical foundations, research supporting it, free self-report assessments, and a directory of ACT therapists. The ACT webpage can be helpful for musicians looking to find a local ACT therapist who may be proficient in performance psychology, while also serving as a resource for clinicians wanting to learn about conditions for which ACT is empirically supported (Association for Contextual Behavioral Science, 2017). We are not aware of another web-based resource that so efficiently disseminates information about other MPA therapies, including CBT.
Of course, there may be disadvantages in choosing ACT over CBT, and musicians should know them prior to participating in an ACT treatment. Two of the most common criticisms are that ACT’s empirical support is smaller and less methodologically rigorous than that of CBT (Öst, 2008, 2014), and ACT may not offer anything new as a behavioral therapy (Herbert, 2005). Regarding the former point, Öst conducted two influential meta-analyses of ACT treatment studies, including 13 RCTs with a total of 677 patients (Öst, 2008) and 60 RCTs with 4,234 patients (Öst, 2014). He concluded that ACT showed only small to moderate effectiveness in treating a variety of disorders, and that ACT studies were not improving methodologically over time, as they were found to be less rigorous than comparable CBT studies on a methodological quality scale he created (Öst, 2008, 2014). For example, he pointed out that ACT studies often compared treatment effects to those of wait-list control groups rather than to other treatments with known efficacy, and that ACT therapists were often not assessed for adherence to treatment manuals (Öst, 2014). However, Öst’s reviews have since been shown to contain numerous factual and interpretive errors by both ACT researchers and independent scholars, leading many to conclude that they are largely biased against ACT (Atkins et al., 2017). For example, A-Tjak and colleagues (2015) used Öst’s same quality rating scale in their meta-analysis and found ACT studies were actually improving methodologically over time, and that ACT was equally effective as CBT in treating anxiety disorders. Furthermore, Öst’s criticisms are becoming outdated, as there are currently over 200 ACT RCTs and many of them have attempted to correct the methodological flaws he reported, i.e., by including evaluations of therapist adherence/competence and by comparing ACT to well-established therapies (Association for Contextual Behavioral Science, 2017). Regardless of which side of the debate one falls on, performance psychologists who use ACT to treat MPA in experimental trials must inform their clients that it is not yet well-established as a treatment for MPA, therefore it may not help them.
In response to the latter criticism, that ACT does not offer anything new as a behavioral therapy, some ACT researchers argue it is usually made by CBT advocates who have been on the receiving end of the allegation by psychoanalytic and other therapists (Herbert, 2005). In fact, ACT’s model of psychological flexibility is indeed a new, and organized way of linking theory and philosophy with clinical practice (Herbert, 2005). This is made clear when considering the different role of exposure therapy in CBT and ACT. Within CBT, exposure therapy is governed by an extinction rationale, in that the patient is repeatedly exposed to a feared stimulus until the fear reaction is extinguished and the patient’s level of distress is reduced (Foa & McLean, 2016). However, there is evidence that a reduction in distress may not be needed for exposure therapy to be effective (Baker et al., 2010). Within ACT, for example, exposure tasks are directly linked to patients’ values and are governed more by a psychological flexibility rationale (Morris, 2017), which is a concept directly linked to functional contextualism (Hayes et al., 2011), as we discussed earlier. In other words, exposure exercises provide patients with the opportunity to experience feared stimuli in the context of valued activities, and the willingness to persist with valued tasks, rather than extinction, is what is prioritized by ACT therapists when doing exposure work (Eifert & Forsyth, 2005; Morris, 2017). Therefore, ACT’s reframing of exposure tasks as opportunities to practice valued behavior may make them more personally meaningful to clients, in comparison to those in CBT (A-Tjak et al., 2015).
How ACT might be used to treat MPA
For performance psychologists who choose to investigate ACT to treat MPA, they should know that the treatment is made easier through the use of valid self-report measures to track improvements in Hexaflex processes, e.g., the Acceptance and Action Questionnaire, or “AAQ-2” (Bond et al., 2011), PHLMS (Cardaciotto, Herbert, Forman, Moitra, & Farrow, 2008), BAFT (Herzberg et al., 2012), and the Valued Living Questionnaire, or “VLQ” (Wilson & Murrell, 2004). The performance psychologist is also encouraged to follow an established treatment manual for treating anxiety (Eifert & Forsyth, 2005), and they should make modifications that apply more to musicians with MPA, when needed. For example, social interaction exercises should be substituted with music performances when conducting in-session exposures. An individualized ACT treatment typically lasts 10–12 therapy sessions, each approximately 60 minutes long (Craske et al., 2014; Eifert & Forsyth, 2005). According to Eifert and Forsyth’s (2005) manual, the first half of treatment focuses on orienting clients to the goal of increased psychological flexibility, identifying dysfunctional behaviors aimed to repeatedly control or eliminate anxiety, enhancing mindful acceptance of MPA symptoms through meditation exercises, and promoting cognitive defusion through language-based exercises (for specific defusion exercises, see Juncos & Markman, 2015). Performance psychologists can use metaphors and in-session exercises to achieve some of these goals. For example, the “Child-in-a-Hole” and “Feeding-the-Anxiety-Tiger” metaphors are designed to illustrate the dysfunctional nature of repeated efforts to control MPA symptoms, whereas the “Chinese Finger Trap” and “Tug of War with Anxiety Monster” exercises are designed to foster acceptance of one’s MPA symptoms (Eifert & Forsyth, 2005).
The second half of an ACT treatment for MPA focuses on strengthening mindfulness and defusion skills through in-session exposure exercises designed to induce the very thoughts and sensations normally feared/avoided by the musician. By mindfully observing MPA symptoms and defusing from what their minds tell them about their symptoms, a musician becomes more accepting of and less reactive to those symptoms. Additionally, the client and performance psychologist may spend several sessions identifying performance-related values that bring vitality back to the performances when expressed. Clients then practice engaging in behavior consistent with those values during in-session music performances. They are encouraged to persist with valued behavior even while experiencing MPA symptoms, so that psychological flexibility is achieved (Eifert & Forsyth, 2005). When a musician relapses into dysfunctional behaviors aimed to control or reduce MPA symptoms, the performance psychologist may encourage them to practice mindfulness and defusion skills while simultaneously redirecting energy towards achieving valued goals in the performances (Eifert & Forsyth, 2005). Examples of musicians’ performance-related values include connecting with the audience, being more emotionally expressive while performing, or, conversely, staying focused on proper technique.
It is important to emphasize that if the performance psychologist can concretize the musician’s performance values into actual behavior to be engaged in during performances, the musician may further benefit from the ACT treatment. For example, while working with an undergraduate violinist with MPA who was studying to be a music teacher, Juncos and Markman (2015) learned she valued being an effective teacher to her students. She elaborated this required having superb knowledge of technique and effective communication skills to explain and demonstrate the techniques to her students. Juncos and Markman (2015) then described how her passion for teaching and her communication skills could help revitalize her performances, and they encouraged her to reframe them as potential teaching opportunities for herself. Specifically, she was encouraged to pretend she was her own student and to silently explain and demonstrate to herself how to perform key aspects of her technique during her own performances, while simultaneously remaining mindful of and defusing from her MPA symptoms. This subtle mental behavior was consistent with her stated value of being an effective teacher, and engaging in it while performing likely helped reinvigorate her performances while also teaching her to be flexible in response to her MPA symptoms (see the “Teaching Technique” section in Juncos & Markman, 2015). It is this component of the therapy, i.e., the collaboration between client and performance psychologist to develop value-consistent behavior(s) to be used during performances, that may also make ACT more personally meaningful for the musician and very rewarding for the performance psychologist. CBT does not typically use such values-guided exposure exercises in anxiety treatments (Morris, 2017). For another example of a values-guided technique created for musicians, see the “Emotional Expression Technique” section in Juncos and colleagues (2017).
Towards an evidence-based practice model in performance enhancement
ACT-based performance enhancement program for athletes
We believe ACT can also serve as an effective performance enhancement (PE) program for musicians and other performers (athletes, dancers, actors, comedians, etc.) and should be studied further. In fact, an ACT-consistent PE program has already been used with athletes for more than 10 years and will be discussed in detail here, i.e., the Mindfulness–Acceptance–Commitment approach for enhancing performance, aka the “MAC” (Gardner & Moore, 2007). In order to achieve peak performance, sport psychology practitioners have long believed an optimal state of arousal, focus, and confidence is necessary, and so, they have been applying psychological skills to help athletes enhance performance-related outcomes for more than 30 years (Gardner & Moore, 2012; Moore, 2003). The most common performance enhancement program for athletes is Hardy, Jones, and Gould’s (1996) Psychological Skills Training program, or “PST”, which teaches athletes a number of self-regulatory strategies thought to facilitate performance excellence, i.e., goal-setting, mental imagery, arousal control, and self-talk modification (Gould, Eklund, & Jackson, 1992; Hardy et al., 1996). The MAC approach is quite different to PST, though, because it is a mindfulness-and-acceptance-based program that asserts that unwanted internal experiences such as negative thoughts and high levels of arousal do not necessarily impede performance, therefore, performers need not respond to them (Gardner & Moore, 2007). Rather, the MAC approach promotes acceptance of one’s internal experiences as they are, so that attention is maintained externally on the performance and on eliciting appropriate performance-related responses. It is organized into five phases taught over a seven-session period: educating the client about the MAC protocol, mindfulness and defusion, identification of values and eliciting commitment, acceptance, and skill integration and practice (Gardner & Moore, 2004).
Gardner and Moore (2007) created the MAC program in response to the lack of strong empirical support associated with common techniques found in PST, i.e., goal setting, imagery, self-talk modification, and arousal control, some of which are currently being used with musicians (Clark & Williamon, 2011; Hatfield, 2016; Osborne et al., 2014). In an influential meta-analysis of 97 studies investigating the effectiveness of PST strategies on enhancing performance skills, Moore (2003) applied the same standards set by the APA’s Division 12 Task Force for defining empirically supported treatments in Clinical Psychology (Chambless & Hollon, 1998) and found that none of those aforementioned PST strategies showed efficacy at the well-established level of support when used as singular interventions to enhance athletic performance enhancement. For example, self-talk modification is considered to be an important component of PE work in which athletes are taught to limit their cognitive content to accurate and realistic self-statements, among other modifications (Zinsser, Bunker, & Williams, 1998). However, Moore’s (2003) review showed that of the six studies using it with athletes, only three were methodologically strong enough to be useful in determining self-talk modification’s efficacy, according to Chambless and Hollon’s (1998) criteria (Barling & Breski, 1982; Howard & Reardon, 1986; Rodgers, Hall, & Buckolz, 1991). Of those three studies, though, none showed that a significant improvement in athletic performance had occurred when compared to a control condition (Moore, 2003). Moore (2003) found that only combined PST interventions showed efficacy in significantly improving athletic performance, whether they involved combinations of two PST interventions, i.e., arousal control and imagery (Gravel, Lemieux, & Ladouceur, 1980; Weinberg, Seabourne, & Jackson, 1981; Wrisberg & Anshel, 1989); three interventions, i.e., arousal control, imagery, and self-talk modification (De Witt, 1980); or all four interventions (Beauchamp, Halliwell, Fournier, & Koestner, 1996). Moore (2003) then concluded that PST interventions, when used singularly, were best described as “experimental”, another term to describe a promising intervention with a low level of empirical support (Chambless & Ollendick, 2001), and that only combined interventions with well-established efficacy, e.g., arousal control and imagery, should be used for PE work with athletes. Moore (2003) also noted her review was not intended to discourage sport psychologists from using singular PST interventions with athletes, as they may become well-established in due time. However, in light of the lack of empirical support for PST interventions at the time of her review, the MAC program was thereby developed to better bridge the gap between science and practice within sport psychology (Gardner & Moore, 2004, 2006, 2007). Lastly, we are not aware of any criticisms of the MAC approach, but we assume they exist and are similar to those of ACT, given the similarities between the two interventions.
Since its inception, a number of studies have provided empirical support for the efficacy of the MAC approach with athletes. Three case studies (Gardner & Moore, 2004; Lutkenhouse, 2007; Schwanhausser, 2009), three open trials (Hasker, 2010; Plemmons, 2015; Wolanin, 2005), and one RCT (Lutkenhouse, Gardner, & Moore, 2007) have been published, all of which investigated the MAC approach with athletes of varying ages and skill levels. These studies consistently show competitive and recreational athletes have improved their performance skills after undergoing the MAC protocol, some of whom to a significant degree. For example, in an open trial comparing the effects of the MAC approach on 11 female Division 1 field hockey and volleyball athletes to a no-treatment control with similar athletes, Wolanin (2005) reported that MAC participants earned significantly higher coach ratings of athletic performance than the controls did. Furthermore, in a large RCT (N = 118) comparing the effects of MAC versus PST on the performances of both male and female Division 1 athletes (men’s and women’s soccer, women’s field hockey, men’s and women’s crew, and men’s wrestling), Lutkenhouse and colleagues (2007) reported MAC participants earned significantly higher coach ratings of athletic performance than PST participants. In light of these favorable findings, Gardner and Moore (2012) reported the empirical support for the MAC program has reached the probably efficacious level, and all that is needed for it to reach the well-established level is another well-designed RCT with similarly positive findings, conducted by different researchers. In addition to the MAC approach, researchers have also used a sport-adapted version of ACT in two studies, both of which demonstrated an increase in performance quality. García, Villa, Cepeda, Cueto, and Montes (2004) showed that 16 elite canoeists receiving a sport-modified ACT intervention outperformed a matched control group (receiving hypnotherapy) on a canoeing training apparatus. Similarly, a study by Bernier, Thienot, Codron, and Fournier (2009) showed a group of seven adolescent elite golfers receiving an ACT-based intervention made more improvements in national rankings than a control group receiving traditional PST.
ACT/MAC as a performance enhancement program for musicians
Rather than discuss how an ACT or MAC-based PE program for musicians might progress, we wish now to strengthen the rationale for investigating such programs with musicians by discussing relevant, multi-disciplinary research in support of the underlying mechanisms of those programs. A discussion of how ACT or the MAC program might progress would be redundant, given the inevitable similarities between treating a musician with MPA with ACT and doing ACT or MAC-related PE work with a musician. Moreover, Juncos and colleagues’ ACT for MPA treatments were clearly intended to be PE programs, because in two of their studies they predicted an improvement in juror-rated performance quality would occur at post treatment (Juncos et al., 2017; Juncos & Markman, 2015). Results from both studies indicated the musicians’ performance skills did indeed improve. After 10 ACT sessions, the student violinist improved her performance quality according to a professional musician’s rating (Juncos & Markman, 2015), and after 12 sessions the seven vocalists significantly improved their average performance quality (Juncos et al., 2017) according to two independent judges’ ratings on the Music Performance Quality (MPQ) form (Educational Testing Service, 1998). In light of these positive results, ACT would meet criteria for a promising intervention as a PE program for university musicians with MPA. Furthermore, the results of García and colleagues’ (2004) and Bernier and colleagues’ (2009) pilot studies indicate ACT-consistent interventions are also promising as PE programs for elite adolescent athletes. See Table 2 for a summary of the studies in which ACT was used as a PE program.
Summary of ACT-based performance enhancement (PE) studies across sport and music domains.

ACT = Acceptance and Commitment Therapy; MPA = music performance anxiety; PQ = performance quality; PST = Psychological Skills Training; tx = treatment.
After treatment in both studies, the vocalists and violinist reported an increased confidence in their performance skills, which they attributed to being more focused on behaving in ways consistent with their performance values, rather than on attempting to control MPA symptoms (Juncos et al., 2017; Juncos & Markman, 2015). This shift in attention is consistent with outcomes of MAC-related studies, in which athletes learned to decrease self-focused attention and increase task-focused attention on values-consistent behavior (Gardner & Moore, 2004; Lutkenhouse et al., 2007; Wolanin, 2005). It is possible, then, the same mechanisms that led to improvements in performance quality in Juncos and colleagues’ research (Juncos et al., 2017; Juncos & Markman, 2015) were also occurring in the MAC studies, but further research is needed to confirm this.
The results of the aforementioned clinical ACT studies comparing ACT to CBT in treating Social Anxiety Disorder (Herbert et al., 2017) and public speaking anxiety (Glassman et al., 2016) support this possibility and further strengthen the rationale for investigating an ACT-based PE program with musicians, specifically. In both studies, the authors theorized the patients who receive CBT may be taxing their working memory by engaging in CR tasks during social interactions and speeches, whereas patients receiving ACT may use less mental energy by defusing from anxious thoughts and switching focus onto engaging in their chosen, valued behaviors. Glassman and colleagues (2016) also found that when ACT participants were giving a speech there was a decrease in blood volume in the left dorsolateral prefrontal cortex regions of their brains (a part of the prefrontal cortex involved in working memory, task switching, and other executive functions), whereas CBT participants showed an increase in blood volume in that region. Therefore, ACT treatments may free more cognitive resources than CBT, likely due to shifting attention away from monitoring one’s anxiety symptoms to further engagement in task-related behavior, which may result in improvements in observer-rated behavioral performances (Glassman et al., 2016; Herbert et al., 2017).
Additionally, there is compelling data from cognitive neuroscience studies involving experienced meditators and elite athletes that support the proposed mechanisms of change in MAC programs and ACT treatments. Using functional magnetic resonance imaging (fMRI) scans, Brefczynski-Lewis, Lutz, Schaefer, Levinson, and Davidson (2007) studied the brains of 14 experienced Tibetan Buddhist meditators with 10,000 to 54,000 hours of meditation experience and 16 age-matched novices with no meditation experience, and another group of 11 age-matched novices who were promised US$50 for finishing in the top third of activating attention regions of the brain (serving as a control for motivational effects). Their task involved sustaining attention on a dot on a computer screen for three minutes, then resting for 90 seconds, then repeating this cycle of focusing/resting continuously for approximately 20 minutes. The experimenters also inserted distraction sounds of positive, neutral, and negative valence regularly into the task and instructed participants to remain focused during distractions. As predicted, Brefczynski-Lewis and colleagues (2007) found the experienced meditators sustained attention longer than either novice group, but interestingly, the fMRI scans of the most experienced mediators (M = 44,000 hours experience) showed significantly less activation in brain areas devoted to attention than the scans of the meditators with less experience did (M = 19,000 hours). They concluded that the most experienced meditators’ brains were more efficient in allocating mental resources to performing the task, which helped them devote less mental energy to it than the meditators with less experience (Brefczynski-Lewis et al., 2007). This finding highlights how acquiring the meditation-based skill of sustained attention can become automated so that it requires less mental effort to reach such a mindful state over time (Gardner & Moore, 2012). Fortunately, the beneficial effects of meditation on attention can be seen much more quickly than Brefczynski-Lewis and colleagues’ (2007) study would suggest, likely within three months of regular meditation practice (MacLean et al., 2010), or possibly as soon as four days (Zeidan, Johnson, Diamond, & Goolkasian, 2010).
Studies involving elite athletes show a similar trend of mental efficiency, which suggests that elite athletes also require less use of the attention centers located in the left temporal and left prefrontal cortex areas than less experienced athletes do (Gardner & Moore, 2012). For example, Crews and Landers (1993) studied the electroencephalography (EEG) patterns of 34 highly skilled golfers during the moments before putting and found significant decreases in alpha-wave activity in the left temporal region as the moment of putting approached, a brain area typically associated with verbal-linguistic activity. Furthermore, in a review of other EEG studies with athletes, Hatfield, Haufler, Hung, and Spalding (2004) concluded that less experienced athletes generally demonstrated higher levels of left-hemisphere activation when on task, whereas more experienced athletes showed a more balanced activation of left and right hemispheres.
Gardner and Moore (2012) discuss these parallel findings and assert that elite athletes, like experienced meditators, develop the ability to use cognitive resources more efficiently by repeatedly sustaining attention on important performance tasks until it becomes more automated. These findings, and those from the clinical ACT vs. CBT studies (Block, 2002; Brown et al., 2011; Glassman et al., 2016; Herbert et al., 2017), those from Juncos and colleagues (Juncos et al., 2014; Juncos et al., 2017; Juncos & Markman, 2015), and those from the MAC studies (Gardner & Moore, 2004; Hasker, 2010; Lutkenhouse, 2007; Lutkenhouse et al., 2007; Plemmons, 2015; Schwanhausser, 2009; Wolanin, 2005) point to similar, attention-strengthening mechanisms occurring in all treatments that are likely associated with the observed improvements in performance quality. ACT and the MAC approach both aim to improve one’s ability to sustain mindful attention through repeated meditation exercises during the course of treatment, an ability associated with improved task performance with experienced meditators (Brefczynski-Lewis et al., 2007). Furthermore, these studies’ findings also have an obvious implication for musicians looking to enhance their performance skills: an ACT or MAC-based PE program appears more likely to facilitate improvements in performance quality than a CBT or PST-based one, but further research needs to confirm this. Considering that CBT and PST emphasize volitional efforts at both noticing one’s cognitive activity and then changing cognitions deemed to be problematic (Gardner & Moore, 2012), perhaps it is not surprising that CBT-based treatments for anxiety and PST programs for musicians have not led to significant improvements in performance quality as consistently as ACT/MAC interventions have done, whether it is on a public speaking task (Block, 2002; Glassman et al., 2016), a social skills task (Herbert et al., 2017), an academic test (Brown et al., 2011), a sport performance (Lutkenhouse et al., 2007), or a music performance (Clark & Williamon, 2011; Kageyama, 2007). CBT’s use of CR tasks and PST’s use of self-talk modification may prove too costly for one’s cognitive resources, and musicians may never reach the point of full automaticity with these tasks because their focus is obviously needed more on their performances. Even if these CBT/PST-based skills do become automated, they may not be as helpful as has been previously thought. There is debate over the therapeutic relevance of CR tasks within CBT treatments (DeRubeis et al., 1990; Hofmann et al., 2007). For example, Teasdale and colleagues (2002) hypothesize that distancing one’s self from one’s negative thoughts, rather than changing their content, may actually be the mechanism by which CR tasks improve mood in CBT treatments for depression, an idea that is consistent with the perspective ACT and the MAC approach take in teaching how best to relate to unwanted thoughts. Perhaps an acceptance-based program that encourages musicians to simply let go of the struggle with their unwanted thoughts would be more helpful, as suggested by some researchers (de Paiva e Pona, 2015; Juncos et al., 2014; Juncos & Markman, 2015; Juncos et al., 2017).
Factors to consider when applying ACT/MAC approach to musicians
In light of the emerging research supporting ACT/MAC-based interventions, we will briefly discuss some factors that may arise when applying interventions from either program to musicians in experimental trials. Gardner and Moore (2007) originally advertised the MAC approach as a PE program for all performers, including musicians, but thus far no published studies have investigated it specifically with musicians. This may be due to awareness on their part that musicians’ needs are distinct from those of athletes. Be that as it may, we believe performance psychologists who work mainly with athletes are still in a position to help musicians enhance their performance skills, as long as they educate themselves on the important cultural differences between the sport and music performance domains. A recent article in Sport, Exercise, and Performance Psychology recommended that practitioners in this position adopt a positive, culturally sensitive, evidence-based, and holistic approach when applying performance psychology principles to musicians, and that they become aware of systemic challenges likely to be faced when transferring knowledge between sport and music performance domains (Pecen et al., 2016). These recommendations are important and will help guide our discussion.
We agree with Pecen and colleagues (2016) that performance practitioners should take an evidence-based approach towards PE work with musicians. Therefore, we caution performance psychologists using PST interventions to only use those with proven efficacy to improve performance quality, i.e., multi-component interventions, and we caution ACT practitioners to avoid using ACT with musicians in clinical practice until there is more empirical support. We also strongly encourage performance psychologists to further investigate newer PE programs such as ACT or the MAC approach with musicians, given the high likelihood they will have efficacy. In doing do, they should strive to conduct methodologically rigorous experiments in keeping with the standards for defining empirically supported treatments discussed heretofore (Chambless & Hollon, 1998), and they again must inform their clients that neither ACT nor MAC are well-established yet as PE programs for musicians. At some point, the performance psychologist will also need to decide which PE program to investigate further with musicians: ACT or the MAC approach. We believe either approach would be equally helpful given the similarities between them, but it may be more practical to choose ACT over the MAC approach. ACT’s empirical support has more depth and breadth than that of the MAC program – a host of clinical and non-clinical problems have been effectively treated by ACT across several replicated trials, e.g., depression, Social Anxiety Disorder, Obsessive Compulsive Disorder, psychosis, chronic pain, weight management, smoking cessation, substance abuse, work-related stress and burnout, eating disorders, and others (Levin et al., in press). Given how professional musicians are reported to have more incidences of mental health problems than workers in other occupations, most commonly anxiety and depression (Gross & Musgrave, 2016; Kenny et al., 2012), ACT may fare better in treating those musicians with more severe clinical presentations. Furthermore, though the MAC approach already has a treatment manual, existing clinical ACT manuals can be readily adapted for PE work, as shown by Juncos and colleagues (Juncos et al., 2017; Juncos & Markman, 2015) and by other researchers (Bernier et al., 2009; García et al., 2004). Of course, ACT researchers are encouraged to develop a proper treatment manual for PE work with musicians, because it would help organize therapeutic interventions into one resource for future ACT trials.
We also agree with Pecen and colleagues (2016) that performance practitioners who work with musicians should consider potential cultural challenges that may arise in the process. When conducting research within a conservatory or university music department, for example, we believe the performance psychologist must respect the teacher–student bond and avoid giving performance-related instructions that contradict those of their professors and other key personnel. Student musicians will likely defer to their teachers in those situations (Jordan, 2016). For example, when a student vocalist values expressing herself and is then encouraged by the performance psychologist to be more emotionally expressive while performing, she may resist such encouragement if performing a traditional German Lieder song, because her teacher may instruct her to focus mainly on communicating the song’s lyrical beauty. However, this instruction may be more appropriate when working with a student performing the aria “Ah fuggi il traditor” from Act One of Mozart’s Don Giovanni (1787), an aria that is best performed with more emotional expressivity. Pecen and colleagues (2016) rightfully assert that PE work is meant to complement, rather than contradict, the more technical instructions given to students by their teachers. We agree and add that whenever the student’s values conflict with the teacher’s instructions, the performance psychologist should guide the student to make a decision about how best to strike a balance between the two. While they may defer to their teacher on this issue, it should be noted that communication of emotion is an important part of performing music that separates it from sport performance (de Paiva e Pona, 2015), and it should not be overlooked. Therefore, we recommend performance psychologists consult with students’ teachers, whenever possible, so any contradictory or irrelevant instructions regarding the appropriate timing of emotional expression (or of other performance components) may be minimized. We also encourage performance psychologists to further investigate ACT as a PE program that may enhance emotional expressivity, as the student vocalists in Juncos and colleagues’ (2017) study attributed their increased confidence to focusing on valued action during performances, i.e., expressing themselves emotionally.
Finally, due to the success of the MAC and other ACT-based approaches with athletes, we also recommend that performance psychologists consider ACT and/or the MAC approach as having the potential to be best practice as PE programs for musicians. However, an ACT or MAC-based PE program will need to be compared to a more traditional PST program with musicians in two independent studies or a large series of independent single-case designs before this is confirmed.
Conclusion and future directions
The newer field of performance psychology has evolved to a point where practitioners addressing the mental health and/or performance needs of musicians should adopt an evidence-based model of care similar to that found in related disciplines, i.e., Clinical Psychology. Since the APA’s (Division 12) Task Force was implemented (Chambless & Hollon, 1998), it has become standard practice for clinical psychologists to use treatments that have adequate research support and are cost effective, and to disseminate information about such treatments when necessary. This ultimately results in greater protections for the public, because those who are in need of help, i.e., musicians, can learn which treatments are well-established for certain disorders and then seek out practitioners trained in those treatments, i.e., performance psychologists. Such a practice must become the norm for practitioners working with musicians too, especially since they are more prone to mental health problems than the general public (Gross & Musgrave, 2016; Kenny et al., 2012). If such a higher standard is adopted, the field of performance psychology will undoubtedly improve, because the musicians it serves will be helped even further.
Footnotes
Contributorship
DJ primarily wrote the paper. EPP assisted with the conceptualization of the third section and with the organization of the overall paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Peer review
László Stachó, Liszt Ferenc Zenemuveszeti Egyetem, Kodály Institute, Hungary.
Karen Wise, Guildhall School of Music and Drama, UK.
Graham Welch, Institute of Education, University College London, UK.