
Abstract
Among mammals who invest in the production of a relatively small number of offspring, bonding is a critical strategy for survival. Mother–infant bonding among humans is not only linked with the infant’s survival but also with a range of protective psychological, biological, and behavioral responses in both mothers and infants in the post-birth period and across the life span. Anthropological theories suggest that one behavior that may have evolved with the aim of enhancing mother–infant bonding is infant-directed singing. However, to date, despite mother–infant singing being practiced across cultures, there remains little quantitative demonstration of any effects on mothers or their perceived closeness to their infants. This within-subjects study, comparing the effects of mother–infant singing with other mother–infant interactions among 43 mothers and their infants, shows that singing is associated with greater increases in maternal perceptions of emotional closeness in comparison to social interactions. Mother–infant singing is also associated with greater increases in positive affect and greater decreases in negative affect as well as greater decreases in both psychological and biological markers of anxiety. This supports previous findings about the effects of singing on closeness and social bonding in other populations. Furthermore, associations between changes in closeness and both affect and anxiety support previous research suggesting associations between closeness, bonding, and wider mental health.
Introduction
Among mammals, the female reproductive strategy involves investing in the production of a relatively small number of offspring and relying on quality of care and ability to support and enable the infant’s survival. To facilitate this, female mammals form strong social bonds with their infants (Broad, Curley, & Keverne, 2006).
In some mammals, there have been suggestions that a narrow sensitive period exists during which mother–offspring bonding happens very quickly. This is particularly the case when animals are able to walk independently within minutes after birth, providing a higher risk for the accidental confusion of offspring (Lamb & Hwang, 1982). However, researchers have proposed that the motoric limitations faced by human infants (which remove some of the risks of accidental confusion caused by animals being quickly mobile) render a rapid mother–infant bonding process not evolutionarily necessary (Lamb & Hwang, 1982; Myers, 1984). Consequently, while the immediate postpartum period is important for the bonding process and is characterized by a sensitive period of heightened maternal motivation to interact with their infants and receptiveness to the formation of this bond, bonding activities continue to be important over the following weeks and months (Maestripieri, 2001).
Part of the reason that mother–infant bonding in humans is an important focus of research is that poor bonding is associated with adverse effects for infants. Mother–infant attachment is associated with clearer recognition from the mother of her infant’s needs and an appropriate response, whereas insecure attachments are associated with less accurate interpretations or responses to infant signals (de l’Etoile, 2006). Moreover, there are suggestions that bonding between mother and infant can predict longer term relationships between a mother and her child (O’Higgins, Roberts, Glover, & Taylor, 2013). Studies have also linked mother–infant bonding and the related quality of mother–infant interactions in the long term with infants’ cognitive development, social competence, and general intelligence (Ainsworth & Bell, 1972; Feldman & Eidelman, 2004; Forcada-Guex, Pierrehumbert, Borghini, Moessinger, & Muller-Nix, 2006; Licata et al., 2014; Olson, Bates, & Bayles, 1984). And in its extreme, poor bonding is associated with an increased risk of subsequent child abuse or neglect (Brockington, 1998). Longitudinal data suggest that poor early parental bonding may even play a role in the development of psychiatric symptoms in adulthood (Lima, Mello, & Mari, 2010).
Bonding not only has implications for babies but is also associated with psychological and behavioral states in mothers. For example, bonding and anxiety have been linked, with different mother–infant interactions recorded for mothers experiencing anxiety, leading to alterations in infant behavior and coping responses to social challenges (Kaitz, Maytal, Devor, Bergman, & Mankuta, 2010). Bonding during pregnancy and post-birth has been associated with mental health, with mothers categorized as anxious-ambivalent in their bonding styles exhibiting poorer mental health than women with more secure bonding (Mikulincer & Florian, 1999). More specifically, mothers affected by perinatal mental health problems show decreased levels of affective communication with their babies (Kumar, 1997; Milligan, Atkinson, Trehub, Benoit, & Poulton, 2003). For example, mothers with postnatal depression have been shown to exhibit decreased activation in Brodmann’s area of the brain when their infants cry (Leibenluft & Yonkers, 2010). While the direction of causality between bonding and mental health is hard to confirm, psychopharmacologic studies in postnatal depression, while showing effects of medication on postnatal depression itself, have not shown strong effects of medication on mother–infant interactions and bonding, suggesting that enhanced mental health is not enough on its own to increase bonding (Wisner et al., 2006; Yonkers, Lin, Howell, Heath, & Cohen, 2008). Consequently, there is a need to identify interventions that can support mother–infant bonding, not just from a research perspective but also in order to support the wider health and well-being of both mothers and babies.
Among discussions on interventions that can improve social bonding in humans generally, there has been particular interest in the role that music can play. There is a wide literature on the potential role of music as an evolutionary adaptation (Freeman, 2000; Huron, 2001; Tarr, Launay, & Dunbar, 2014). This has been supported by research demonstrating the use of music in cultures globally and across history (Fritz et al., 2009; Gregory & Varney, 1996). Weinstein, Launay, Pearce, Dunbar, and Stewart (2016) have briefly reviewed the potential behavioral aspects of music that support bonding, identifying the abilities of music to foster prosocial behavior, a shared sense of success, physical coordination, shared attention, shared motivation, and group identity as key. In further theoretical work, Tarr, Launay, and Dunbar (2014) have proposed that aspects of exertion, synchronization, self–other merging, and endogenous opioids are key components in music-led social bonding. In testing these theories, recent experimental studies have looked at singing specifically as a behavior that can increase both trait social bonding and related perceptions of state and trait emotional closeness and social cohesion. For example, findings have shown the effects of individual singing sessions in both small and large groups on self-perceptions of closeness among individuals, social behaviors, and oxytocin levels (Fancourt et al., 2016; Kreutz, 2014; Weinstein et al., 2016). In addition, longitudinal studies over periods of several months have shown that singing is associated with significantly faster development of perceived closeness than other social activities (Pearce, Launay, & Dunbar, 2015). This has been dubbed the “ice-breaker effect” of singing in promoting fast cohesion. In other longitudinal studies, singing has also been linked to aspects of social behaviors related to social bonding such as social inclusion and integration (Welch, Himonides, Saunders, Papageorgi, & Sarazin, 2014).
Specifically in relation to mothers and infants, singing has been discussed as an evolutionary adaptation designed to support mother–infant bonding. Falk (2004) has proposed that singing developed for this purpose directly out of motherese; a style of infant-directed speech consisting of exaggerations, elevated pitch, slow repetitions, and melodic elaborations of ordinary vocal communication (Dissanayake, 2004; Mahdhaoui et al., 2009; Saint-Georges et al., 2013). Motherese has been found to occur in cultures globally (Gogate, Maganti, & Bahrick, 2015; Grieser & Kuhl, 1988; Papoušek, Papoušek, & Symmes, 1991; Trehub, Unyk, & Trainor, 1993a, 1993b). This has led to suggestions that it evolved as a way of supporting mother–infant interactions and facilitating nurturing while babies are at a relatively early stage of neurological development (Bouissac, 2004), with the simple melodic arches of motherese being cognitively easier to process than words. In support of this, infants have been shown to engage their attention more in response to motherese rather than standard talking (Fernald, 1985; Kitamura, Guellaï, & Kim, 2014; Pegg, Werker, & McLeod, 1992; Santarcangelo & Dyer, 1988), as well as respond with vocalizations (Pelaez, Virués-Ortega, & Gewirtz, 2011), and demonstrate emotional synchronicity with their mothers (Saint-Georges et al., 2013). Indeed, there has been a noted similarity between the musicality of infants’ cries and the musicality of motherese (Wermke & Mende, 2009), which suggests that mother–infant bonding through motherese could be as a direct result of the enhanced communication it facilitates. Like motherese, maternal singing has been shown to achieve many of the same responses, including modulation of infant arousal, more intense engagement, visual attention, and movement reduction (Nakata & Trehub, 2004; Shenfield, Trehub, & Nakata, 2003). These are all behaviors associated with bonding. Further, mother–infant singing has been shown to have wider benefits in terms of stress reduction and affect regulation. For example, singing has been shown to calm heart rate, increase oxygen saturation and caloric intake, and decrease the number of negative critical events in infants in neonatal intensive care units (Desquiotz-Sunnen, 2007; Filippa, Devouche, Arioni, Imberty, & Gratier, 2013; Loewy, Stewart, Dassler, Telsey, & Homel, 2013). Biological studies have also suggested that singing can modulate cortisol levels in infants, reducing their physiological stress (Shenfield et al., 2003).
However, to date, although studies have looked at the effects of mother–infant singing on infant behaviors as markers of mother–infant bonding, there are few studies that have explored quantitatively whether mothers feel any differently toward their babies when singing to them. This is despite the fact that research suggests that, while mother–infant bonding is a process that involves input from both mother and infant, the mother’s contribution appears to be the most important (Ainsworth, 1979). Among the few studies that do exist, Mello, Maia, and de Andrada e Silva (2009) found that infant-directed singing as part of an eight-session therapy program enhanced mother–infant behaviors, communication, and maternal anxiety. Cevasco (2008) did not find evidence of greater perceived bonding over 2 weeks of playing recordings of mothers singing to their babies. But, as this did not involve live singing and as the author suggests that uneven numbers of medical complications between experimental and control conditions may have affected results, the results in relation to the effect of singing on mother–infant bonding are inconclusive. A longitudinal study has also found that women who sing to their babies in the 3 months following birth have significantly higher self-reported mother–infant bond as well as lower perceived stress (Persico et al., 2017). Finally, a recent correlation study of 391 new mothers found that singing to babies (but not listening to music) was associated with greater self-reported mother–infant bond with mothers who sang daily being over twice as likely to report high perceived bonding with their infants (Fancourt & Perkins, 2017). However, this study was correlational rather than experimental so, as the authors acknowledge, causality cannot be determined. Consequently, much about the impact of mother–infant singing on mothers remains to be explored, and this study focused on this research gap.
The study was designed in the context of this previous understanding of the impact of maternal singing on mother–infant bonding and looked to explore specifically the effect of a short period of singing on in-the-moment self-perceptions of mothers as to how they felt themselves and in relation to their infants. In recognition of the fact that “bonding” is most frequently defined as an ongoing process between mothers and babies (Bicking Kinsey & Hupcey, 2013), we did not attempt to measure trait bonding between mothers and their infants in this study, but instead chose to focus on mothers’ state perceptions. In this study, we used the popular definition by Klaus and Kennell which states that the bond between mothers and their infants is a biologically based emotional investment in the infant (Klaus & Kennell, 1982). Consequently, we chose a primary outcome measure that has been designed to measure “emotional closeness” and is frequently used in bonding studies. Additionally, we included secondary outcome measures that measured in greater depth emotional responses in the mothers, both psychologically and biologically, to try and gain a broader picture of how singing affected mothers. While it is still recognized that in-the-moment assessments do not necessarily relate to wider affective bonding states among mothers (which are, by nature, an ongoing process), they can give an indication as to whether there are changes in related states that are themselves associated with trait bonding. This was judged to be an important preliminary research question in exploring the links between singing and mother–infant bond. As a result, this exploratory study examined two questions: (i) How does infant-directed singing modulate perceived emotional closeness, affect, and anxiety in mothers with young infants in comparison to a non-musical interactive activity? (ii) How do changes in perceived emotional closeness in response to singing interact with changes in affect and anxiety?
Material and methods
Participants and procedure
This study employed a within-subject crossover design. We recruited mothers living in Greater London over the age of 18 with babies between 3 and 14 months old to attend a 90-min experiment with their babies in groups of 8–10. Mothers were identified through a database held by the researchers of women in the local area who were happy to be approached about involvement in research studies (not specifically those relating to music). Mothers were excluded if they regularly smoked, were taking steroidal medication, or did not have a sufficient level of English to provide informed consent. The study received ethical approval from the Conservatoires UK Research Ethics Committee and all participants provided informed consent prior to taking part.
Of 48 women who were screened for eligibility, 44 met the eligibility criteria and participated, although 1 mother had to be excluded from analyses due to significant protocol deviation (leaving the session midway through). The remaining 43 women had an average age of 35.3 years (SD = 4.0, range 28–45), and their babies had an average age of 8.0 months (SD = 2.8, range 3–13.8 months); 76.7% of them were married, 57.1% of them had an undergraduate degree, and 38.1% of them had a postgraduate degree. When asked how confident they felt singing on a scale from 1 (not at all confident) to 10 (very confident), the average response was 6.4/10 (SD = 2.0, range 1–10), with a mixture of scores reported including 32.6% of mothers reporting a score of 5 or lower, 27.9% of mothers reporting a score of 6 or 7/10, 30.2% of mothers reporting a score of 9/10, and only 9.3% of mothers reporting a score of 9 or 10/10.
Following consent, participants completed a background questionnaire and baseline measurements before taking part in the first 35-min workshop. There was then a gap of 5 min during which time they provided their second set of measurements, and they then took part in the second 35-min workshop, after which the third set of measurements were taken. To reduce the impact of carryover effects between the two conditions, the order in which women received the two conditions was counterbalanced and order effects were tested for. Due to the inclusion of salivary biomarkers in the study, we standardized the time of the experiment so that the two conditions took place between 2–4 pm: a time of the day when diurnal cortisol slopes are flatter and have lower variability than in the morning. Data were collected by three researchers and the sessions were run by a workshop leader from the Royal College of Music who had received bespoke training and gained experience both in delivering music and non-music creative classes with mothers and young babies as part of a wider project on music and motherhood. A project assistant was additionally present throughout the sessions to support the study team.
The two workshops were designed to be comparable: both involved mothers sitting on mats on the floor in groups of 8–10 with their babies. Both involved gentle physical movement such as rocking the baby. The same leader led both workshops and tried to maintain the same level of social interaction between mothers. The difference in the groups was the nature of the activity undertaken by mothers. The experimental singing condition involved a short song to start that introduced the mothers and their babies to one another (c. 5 min), followed by mothers engaging in simple melodic vocal patterns as musical games with their babies (c. 5 min), then learning some simple calming songs to sing to their babies with the other mothers in the room accompanied by shakers and handchimes (c. 20 min), followed by a closing song (c. 5 min). The comparison condition involved a short introductory non-music round circle activity that introduced the mothers and their babies to one another (c. 5 min), followed by mothers engaging in simple non-melodic vocal exercises with their babies (c. 5 min), then playing and talking with their babies and with the other mothers in the room assisted by sensory objects selected by the workshop leaders such as scarves and rattles (c. 20 min), followed by a closing round circle goodbye (c. 5 min).
The decision to conduct the experiment in groups rather than in isolation was based on two factors. First, as we were collecting biological data for this study (see “Measures” below), we needed to have periods of time that were long enough for us to see a biological response. It was anticipated that carrying out either the singing or comparison activity with a baby in isolation for 35 min could be challenging. So carrying out the activity in groups would give mothers more support in both activities, such as being allowed to talk with one another between songs or activities. Second, the experiment did not specifically recruit women who sing to their babies on a regular basis but rather looked for women with a mix of singing habits. Consequently, we anticipated that mothers might feel self-conscious about singing for 35 min on their own and potentially not have a large enough repertoire of songs to sustain the activity for this long. So carrying out the activity in groups was felt to be more appropriate. For this reason, we also designed both activities to involve interactions between the mothers as well as with their babies, aiming to balance this across the two conditions. We included a specific measure of perceived mother–mother bonding as well as a measure of perceived mother–infant bonding (see “Measures” below) to quantify the effects of this.
2.2 Measures
Our primary outcome measure was the Inclusion of Other in Self (IOS) scale, which was developed specifically to measure “emotional closeness.” It has been used in a wide range of studies, including those relating to maternal closeness (Bartz et al., 2010) and those relating to singing and social bonding (Pearce et al., 2015). Further, it is a pictorial scale that depicts seven sets of two circles which move from side by side to almost entirely overlapping, which was felt to be simple and fast to complete and appropriate for the repeated measures involved in this study. However, in order to distinguish perceived general closeness and perceived mother–infant closeness, perceived closeness was measured using two sets of the IOS: one scale where “other” was defined as “your baby” and the other scale where “other” was defined as “other mothers in the room.” This scale is scored from 1 to 7 with higher scores reflecting higher closeness (Aron, Aron, & Smollan, 1992).
Our secondary outcome measures were affect and anxiety. Affect was measured using the positive and negative affect scale; a scale comprising two 10-item subscales (positive affect and negative affect) each scored from 10 to 50 with higher scores indicating higher affect (PANAS; Watson, Clark, & Tellegen, 1988). Anxiety was measured using psychological and biological markers. A visual analog anxiety scale was used ranging from 1 to 10 with higher scores indicating higher anxiety. Saliva samples were collected and analyzed for levels of three hormones: cortisol, cortisone, and dehydroepiandrosterone (DHEA). Cortisol and cortisone are both glucocorticoids released in response to emotional distress (including both stress and anxiety) (Vedhara et al., 2003), while DHEA is a steroid hormone thought to oppose the action of cortisol (Boudarene, Legros, & Timsit-Berthier, 2002). Samples were collected via the passive drool method into 2 mL polypropylene cryovials. Participants were instructed not to eat or drink for 20 min prior to participating in the study, and thereafter were only allowed small sips of water until their participation was complete.
2.3 Analysis
Saliva samples were stored at −20°C for no more than 1 week prior to analysis using high performance liquid chromatography-tandem mass spectrometry with atmospheric pressure chemical ionization coupled with on-line solid-phase extraction, for the steroid hormones cortisol, cortisone, and DHEA.
Data were analyzed using SPSS version 23.0 (IBM, Chicago, Illinois, USA). To explore research question (i) and compare the difference between singing and comparison conditions, the change score was calculated for each condition (post minus pre response) and, given the normal distribution of all data, paired t-tests were carried out. To explore research question (ii) and ascertain if there were correlations between dependent variables, Pearson’s correlations of change scores were carried out. In addition to counterbalancing the two conditions in the study, we also used Pearson correlations to explore the associations between the order the music session was received in and psychological and biological changes, but none was found.
Results
RQ1: How does infant-directed singing modulate perceived emotional closeness, affect, and anxiety in mothers with young infants?
We compared the changes in psychological and biological responses across the session between the two conditions. There was a significantly greater increase in mother–infant closeness in the singing group compared to the comparison group (t = 2.04, p = .048, 95% CI 0.004 to 0.85, d = 0.32). However, for mother–mother closeness, the comparison group had a significantly greater increase than the singing group (t = −2.52, p = .016, 95% CI −0.97 to −0.11, d = −0.39).
In addition, although singing did not alter positive affect in its own right, the small decrease in positive affect in the comparison condition compared to the small increase in positive affect in the singing condition led to an overall significant difference in response between groups, with a greater improvement in positive affect while in the singing condition than the comparison condition (t = 2.64, p = .036, 95% CI 0.18 to 5.11, d = .34). There was also a significantly greater decrease in negative affect in the singing condition than the comparison condition (t = −2.43, p = .019, 95% CI −2.37 to −0.22, d = −.41). However, the difference between groups in anxiety failed to reach significance, with the singing group only showing a marginally greater decrease (t = −1.71, p = .095, 95% CI −1.47 to 0.12, d = −.27).
Regarding endocrine response, the decrease in cortisol was significantly greater in the singing condition than the comparison condition (t = −2.24, p = .031, 95% CI −1.33 to −0.07, d = −.35). However, there was no significant differences between groups in cortisone response (t = −0.40, p = .69, 95% CI −1.11 to0.74, d = −.06) or DHEA (t = −1.43, p = .16, 95% CI −73.18 to 12.72, d = −.24) (see Figure 1). There was also no evidence through correlational analyses of order effects in responses across the two conditions.

Mean changes in (a) social closeness (b) affect and anxiety (c) neuroendocrine markers (with standard error) across 35 min of singing (black) and the comparison condition (gray).
RQ2: How do changes in perceived emotional closeness in response to singing interact with other psychological and biological responses?
When exploring the associations between psychobiological responses to singing (see Table 1), several patterns emerged. First, perceived mother–infant closeness was associated with a medium effect size with positive affect (r = .422, p = .005), negative affect (r = −.410, p = .007), and anxiety (r = −.413, p = .007). However, perceived mother–mother closeness was only associated with anxiety, with a smaller effect size than singing (r = −.313, p = .046). Perceived mother–infant closeness and perceived mother–mother closeness were also correlated (r = .392, p = .009). In addition, anxiety while singing was positively correlated with a large effect size with negative affect (r = .688, p < .001) and negatively correlated with a large effect size with positive affect (r = −.540, p < .001). Positive and negative affect were also negatively correlated, with a small affect size (r = −.378, p = .014). Cortisol and cortisone were strongly positively correlated (r = .696, p < .001) and DHEA was correlated with both (r = .377, p = .02 and r = .366, p = .024). However, they were not correlated with other biological and psychological measures.
Associations between changes in perceived closeness and affect and anxiety when singing.
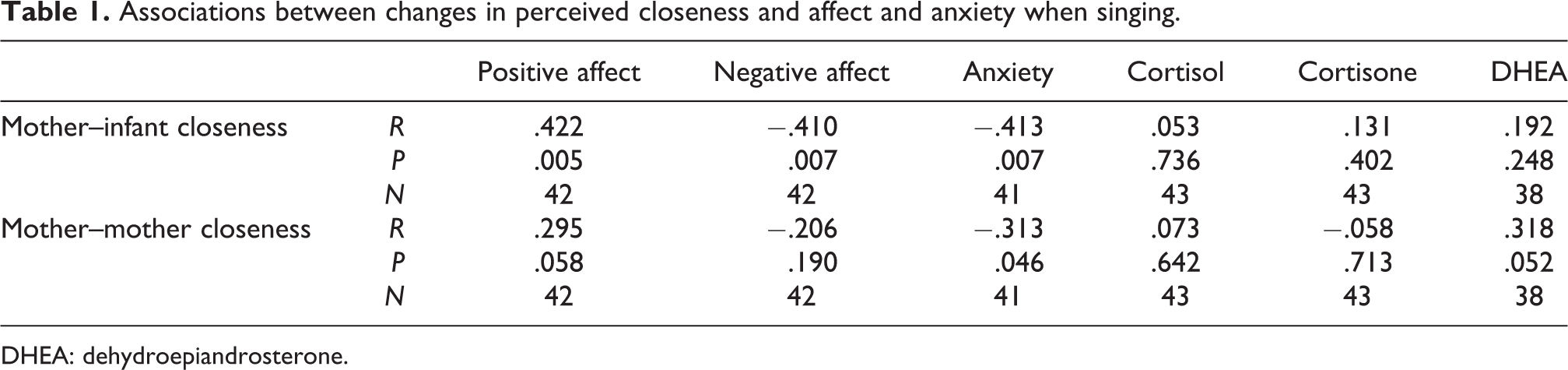
DHEA: dehydroepiandrosterone.
Discussion
We set out to explore whether mother–infant singing increased perceived mother–infant closeness. Using a within-subjects design, we measured the impact of 35 min of singing on maternal perceptions of mother–infant closeness and associated responses including affect and anxiety and compared this with a 35-min comparison condition.
Our results demonstrated that singing can lead to significant increases in perceived mother–infant closeness, over and above a comparison activity involving talking and playing with the baby. This is, to our knowledge, the first quantitative experimental demonstration that a single session of singing can modulate maternal perceptions of mother–infant closeness. While we only focused on state emotional closeness between mother and infant rather than longitudinal bonding, our findings support previous qualitative research on the impact of singing on bonding among new mothers (Creighton, Atherton, Kitamura, & Trondalen, 2013) and the previous correlational study showing higher perceived bonding among mothers who sang on a daily basis (Fancourt & Perkins, 2017). It also ties in with literature that has looked at mother–infant bonding in response to singing from the perspective of infant responses (Nakata & Trehub, 2004; Shenfield et al., 2003). Furthermore, it also echoes findings from studies into singing and both perceived closeness and social bonding in other populations (Fancourt et al., 2016; Kreutz, 2014; Pearce et al., 2015).
A further finding was the effect of singing on the related constructs of affect and anxiety. Regarding affect, this study demonstrated that although both singing and the comparison condition are associated with decreased negative affect, singing leads to significantly greater increases in positive affect and decreases in negative affect than the comparison condition. This study confirmed findings from previous studies that singing can modulate affect (Sanal & Gorsev, 2014; Wendrich, Brauchle, & Staudinger, 2010), although this is the first time it has been shown quantitatively in new mothers. Interestingly, the finding of small (but not significant) increases in positive affect for the singing condition and decreases in positive affect for the comparison condition (yet a significant difference between groups) echoes the same finding in Sanal and Gorsev (2014) and Kreutz, Bongard, Rohrmann, Hodapp, and Grebe (2004). Kreutz et al. interpret this as being an indicator that when there is a singing and comparison group in an experiment, those not singing feel a frustration that translates into a decrease in positive affect. In this study, all participants undertook both conditions, but it is possible that this was still an explanation for the differences in positive affect. Another possibility is that mothers received stronger responses from their infants in response to singing than the comparison activity, which could have led to increases in positive affect in response to singing but again a sense of frustration or lack of positive emotional change in response to the comparison group. This is discussed further in the limitations section later in this article but remains to be explored further. Regarding anxiety, although the singing condition in isolation led to reduced anxiety, this result was not significantly different to the comparison condition. However, singing did lead to a greater decrease in the stress hormone cortisol than the comparison condition. This is in line with previous cortisol studies on singing (Fancourt, Aufegger, & Williamon, 2015; Fancourt et al., 2016; Kreutz et al., 2004). It also ties in with the theories of Carter (1998), who has proposed that social bonding may reduce hypothalamic-pituitary-adrenal (HPA) axis activity, of which cortisol is one of the hormones produced, increasing and decreasing in response to greater or lesser HPA activity. Although there was no correlation between emotional closeness and biological response, this is not entirely surprising given that lag times in hormone production means that the timing of psychological and biological responses do not always coincide, even for measures of the same construct such as psychological and biological measures of stress (Allen, Kennedy, Cryan, Dinan, & Clarke, 2014).
It is also of interest that changes in perceived mother–infant closeness were associated with changes in affect and anxiety, although these associations were not found for mother–mother closeness. This could suggest that there are specific (or specifically strong) pathways linking psychological state and closeness for perceived mother–infant closeness. Indeed, from an evolutionary perspective, it is of note that mother–infant closeness was significantly greater in response to singing than to the comparison condition (which involved talking and playing with babies). This could suggest, similar to the “ice-breaker” effect proposed by Pearce, Launay, and Dunbar (2015), that singing is a fast promoter of social cohesion between mothers and babies. However, it is of note that mother–mother bonding increased more during the non-music comparison condition. This goes against the findings of Pearce et al. (2015) and could suggest that mothers felt more at ease with one another in the talking condition, or it could suggest that they were particularly focused on their babies in the singing condition, to the exclusion of interactions with other mothers in the room. This remains to be explored further.
This study was not without limitations. First, while every effort was made to create similar conditions between groups, the very nature of the two conditions created some differences. For example, although not explicitly measured as part of the study, levels of crying from babies were noticed by the researchers to be higher in the comparison condition than the singing condition. While this may have been by virtue of the condition (given the research suggesting that singing can help to reduce crying among babies; Keith, Russell, & Weaver, 2009), it may also have affected mother–infant interactions as mothers had to alter their behaviors to cope with the crying (such as feeding or rocking their baby) and thereby altered perceptions of closeness. So, future studies are encouraged to involve audiovisual recordings so that differences in behaviors among babies can be quantified. Secondly, we did not explicitly measure the amount of time that mothers looked at their baby as opposed to focusing on other people in the group. It is notable that during the comparison condition, mothers felt more bonded to other mothers than to their babies. While again this is partly by virtue of the condition (in that singing may be a more focused way of engaging with babies than playing and talking to them and has been shown to help maintain eye contact; Nakata & Trehub, 2004; Shenfield et al. 2003), it remains unknown from this experiment whether the percentage of time that mothers focused exclusively on their infant varied between conditions. This study deliberately focused on the effects of singing to babies when in the company of other mothers and babies for reasons outlined in the methods section, and this is a realistic setting in that many mother–infant music classes are group based. However, a future study could benefit from exploring responses from mothers singing to their babies in isolation, perhaps also involving video recording as discussed above to account for differences in behaviors. This could allow for the controlling of other potential social confounders such as perceived group hierarchies that we were not able to test here. Another limitation is that the crossover design means that there may have been carryover effects between the two conditions. However, counterbalancing was employed to achieve symmetry in these potential carryover effects, and correlational analyses did not reveal significant order effects. Further, the design has been used in previous studies involving both psychological data and cortisol (Bernard & Dozier, 2010; Eatough, Shirtcliff, Hanson, & Pollak, 2009). It is also noteworthy that our population consisted of mothers living in West London; an area of contradictory great wealth and high levels of deprivation. This led to a mixture of “extremes”: both those from relatively high and relatively low levels both of socioeconomic status and educational attainment. While we might not hypothesize that the experiment produces different responses among mothers based on such demographic factors, the sample, especially in educational attainment, cannot be taken as entirely representative of the general population. Also in relation to our demographic factors, although we measured confidence in singing, further details on musical experience and musical values were not assessed but could be of interest in future studies. Finally, we focused on maternal perceptions of mother–infant closeness, rather than objective observational measures. The relationship between perceptions and observations in experiments on emotional closeness is under-researched, so we cannot comment on whether perceptions of greater closeness among the mothers led to different behaviors among the mothers. While the results presented here may be taken as preliminary evidence to support future studies on infant-directed singing to support mother–infant bonding, as discussed in our introduction, it should be recognized that this study looked at single time-points before and after a short intervention, which cannot be taken as a direct proxy for longer term mother–infant bonding. Consequently, future studies that are able to focus more on this longitudinal relationship between mothers and infants in response to singing are encouraged.
Overall, however, this preliminary study demonstrates for the first time the psychobiological impact of infant-directed singing on mothers. Further research remains to be undertaken to confirm this finding in light of the limitations outlined above. In particular, we recommend that future studies explore whether regular singing could lead to longer term effects on mother–infant bond, whether the age of the infant and their behavioral responses to maternal singing affect perceptions of maternal closeness, and what feature of mother–infant singing is responsible for any psychobiological responses to singing, including considering the role that synchrony might play and exploring the effects of different genres of music or different levels of musical valence. Such future research could have implications both for our evolutionary understanding of the role of singing for mothers and their infants and for the development of practical interventions and guidance to support new mothers.
Footnotes
Contributorship
DF designed the study, conducted the analyses and drafted the article. RP designed the study and contributed to the article. Both authors approved the final version of the article.
Acknowledgments
The study was approved by the Conservatoires UK Research Ethics Committee. The authors would like to thank Prof Aaron Williamon, Sarah Yorke, Saoirse Finn, and Sarah Collins for their support in conducting the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Arts Council England Research Grants Fund, grant number 29230014 (Lottery).
Peer review
Manuela Filippa, Università della Valle d’Aosta, Psychology. Fabia Franco, Middlesex University, Department of Psychology. One anonymous reviewer.