
Abstract
Management of Crohn’s disease (CD) based on symptom control is a tale of the past as new treatment strategies aim toward a “treat to target” concept and to a patient-tailored approach. Defining treatment goals and assessing therapeutic success have been in the center of IBD research in the past years. Clinical remission and mucosal healing are well-established treatment goals by current recommendations, although prospective data is required to determine whether achieving these targets is enough to alter disease natural course. Furthermore, there is no standard in assessing therapeutic success. Low relapse and hospitalization rates, as well as a low need of surgery are indicators of a successful treatment. Close monitoring is part of the new therapeutic strategy. Monitoring tools are numerous, comprising clinical, biological, endoscopic and imaging scores or parameters but are far from being perfect. The traditional strategy of managing CD patients based on clinical symptoms and response to treatment did not improve the long-term outcomes. Clinical activity scores are frequently used in clinical trials and daily practice, but their use alone is not an accurate measure of inflammation. Endoscopic remission is associated with a lower risk of complications and a better long-term prognostic. Several guidelines include recommendations regarding surveillance endoscopy, but there is an open debate regarding the follow-up intervals. Cross-sectional imaging techniques play a complementary role in assessing transmural inflammation and in identifying extra-intestinal complications of CD and should be used in conjunction with endoscopy. Therapeutic drug monitoring is essential in assessing loss of response and making therapeutic decisions, although firm recommendations are not implemented into daily practice. Extraintestinal manifestations are often disregarded when discussing monitoring protocols. There is no current guideline indication for extraintestinal manifestations monitoring during remission periods.
Keywords
Core tip
Crohn’s disease remains a debilitating disease, far from being controlled in a satisfactory manner. At the present, there is no standard in assessing therapeutic success. Clinical remission and mucosal healing are well established treatment goals, but it’s uncertain if these targets are enough to alter disease course. Monitoring tools are numerous, comprising clinical, biological, endoscopic and imaging scores or parameters but are far from being perfect. The ability to predict the course of disease in any given individual or group of individuals is yet to be achieved. Until then, close monitoring of patients and tailored therapies remain the best approach.
Introduction
Crohn’s disease (CD) is a chronic, relapsing, inflammatory disease that can affect any part of the gastrointestinal tract, with terminal ileum being the most common site of disease localization. CD diagnosis is established on clinical, biochemical, endoscopic, imagistic, and histologic features. 1
Disease natural course often encompasses complications and up to half of patients need surgery within 10 years of diagnosis. 2 Treatment armamentarium widely extended over the past decade but the proportion of patients not entering or not maintaining remission remains high. 3 The ability to predict the course of disease in any given individual or group of individuals is yet to be achieved. Until then, close monitoring of patients and tailored therapies remain the best approach.
Monitoring tools are numerous, comprising clinical, biological, endoscopic, and imaging scores or parameters but are far from being perfect.
A discordance between symptoms and endoscopic findings can be frequently encountered in patients with CD. Patients in clinical remission can have severe endoscopic activity that ultimately leads to complications and altered quality of life. 4 Strategies used to control CD have changed over time from symptom control to inflammation control, mucosal healing (MH) being the new treatment target. MH is correlated with fewer surgical interventions and an improved long-term outcome of CD patients. 5 Although mucosal healing is a well-established treatment goal by current recommendations, prospective data is required to determine whether achieving it is enough to alter disease natural course. Furthermore, there is no validated definition of mucosal healing in CD.
Predictors of treatment response, risk factors for poor disease outcome, surgery and early post-operative recurrence are currently being identified, but disease course remains unpredictable and a challenge for medical management. For example, young age at diagnosis, extensive small-bowel disease, perianal disease, use of corticosteroids, and smoking correlate with poor disease outcome 6 and need for surgery. 7
There is increasing evidence that early treatment with disease-modifying agents, such as biologic agents, may lead to better disease control and prevention of disease progression thus protecting against irreversible damage and restoration of normal quality of life. 8
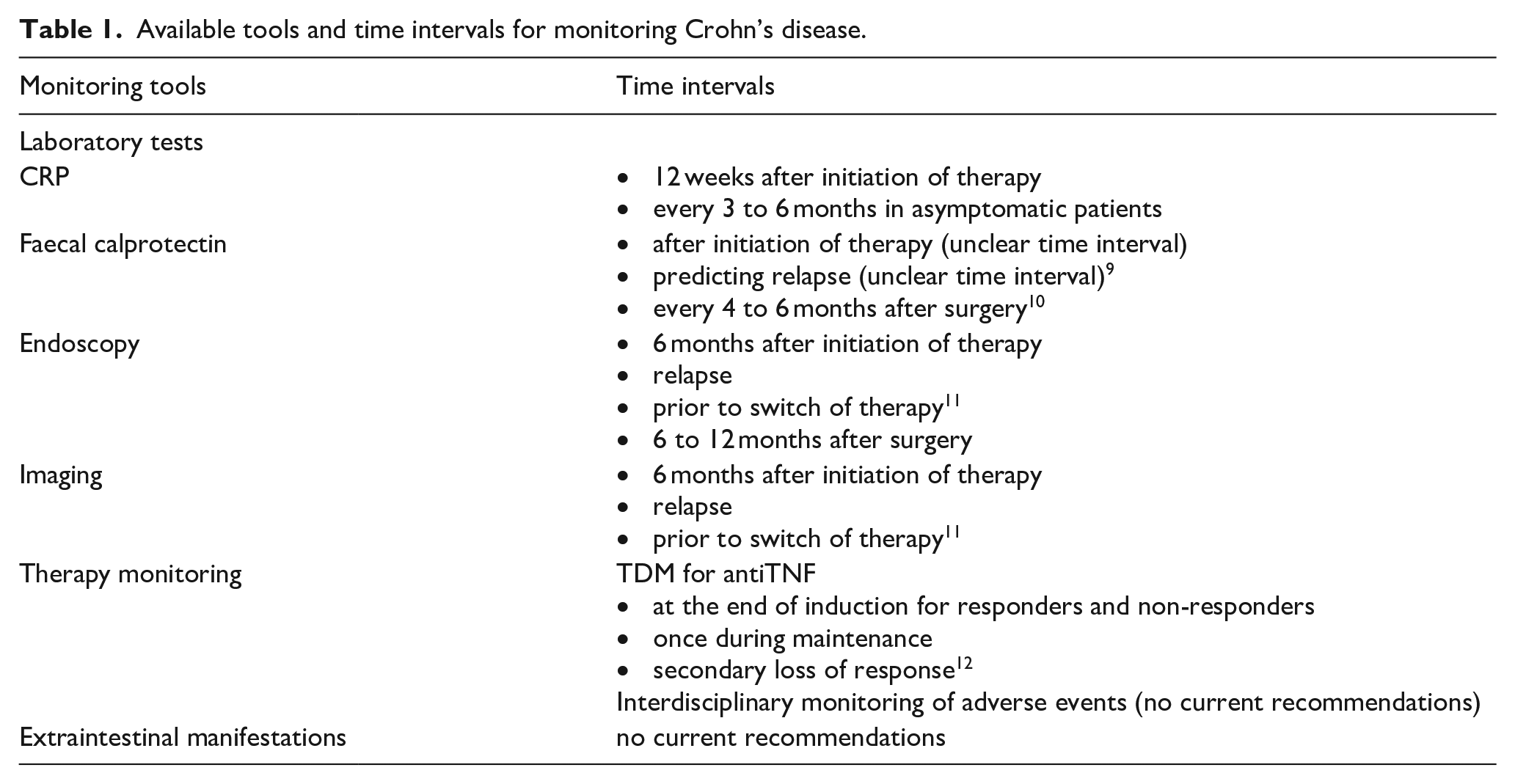
Objective measures of subclinical inflammation could anticipate a clinical relapse and help tailor therapeutic management, but there is a growing need to replace invasive tests by non-invasive markers. Available tools and time intervals for monitoring Crohn’s disease are available in Table 1.
Available tools and time intervals for monitoring Crohn’s disease.
Clinical monitoring
The traditional strategy of managing CD patients based on clinical symptoms and response to treatment did not improve the long-term outcomes. The new concept of “treat to target” highlights the need of objective tools to assess disease activity. The most common scoring systems used to evaluate clinical disease activity are the Crohn’s Disease Activity Index (CDAI), the Harvey-Bradshaw Index (HBI), and the Inflammatory Bowel Disease Questionnaire (IBDQ). The HBI might be easier to use and correlates well, but not perfect with the CDAI results in assessing disease’s activity.13,14 A notable drawback of these scores is the subjectivity of some items, for example “general well-being” or “pain severity” appreciation. Although these scores are frequently used in clinical trials and daily practice, their use alone is not an accurate measure of inflammation. 15
Recurrence after resection in CD is frequent, therefore post-operative monitoring patients should be performed regularly. 16 Although there are studies that suggest that the CDAI score can be used as an assessment tool for recurrence 17 other studies show a poor correlation between CDAI and endoscopic recurrence 1 year after intestinal resection. 18 In a post-operative setting, CDAI might be useful, but ileocolonoscopy remains the gold standard.
The need for more accurate clinical disease activity indices that can provide a good correlation with the endoscopic activity lead to development of a new score, the HBI-PRO score, that incorporates the HBI, C-reactive protein (CRP) and the patient and clinician owns perception of disease activity. 19 This new score better estimates the endoscopic activity of ileocolonic CD.
In our opinion, the superiorirty of a certain monitoring tool is not yet clear, but the use of clinical activity scores and not physician global assessment of symptoms for decision making is mandatory.
Another key point refers to frequency of patient follow-up. Papay et al. proposed an adaptation of monitoring strategies for symptomatic, asymptomatic and post-operative patients. Patients with indolent and stable disease in remission may only be followed up every 12 months, while post-operative patients should be evaluated every 3 months, given the high rates of disease recurrence. 20 This approach could be an acceptable compromise considering symptoms might not correlate well with disease activity. We consider that a proactive routine use of biomarkers every three months even in asymptomatic patients is the best approach.
Laboratory monitoring
Identifying a biomarker that can reflect the presence of active inflammation in IBD patients has been the objective of many studies and remains an unmet need. Data gathered so far support the use of CRP and the heat-stable granulocyte-derived protein, fecal calprotectin (FC).
CRP, although is inexpensive, is not a specific marker of intestinal inflammation and not all patients with active disease have high values of the CRP. 21 Multiple studies have shown a good correlation between the level of CRP and endoscopic activity of the disease.22,23 Also, it was observed that the CRP level rises between 4 and 6 months before clinical relapse, thereby it can be used proactively in order to prevent the relapse. 24 Another advantage would be that it can be used to monitor patients on biologic therapy, as early return to baseline of the CRP level correlates with a sustained long-term response. 25
FC, an inflammatory protein found in the cytosol of human neutrophils, can be used as a marker for monitoring CD. Many studies showed that there is a good correlation between the level of FC and the Crohn’s disease endoscopic index of severity(CDEIS) and the Simple Endoscopic Score for Crohn’s disease(SES-CD),26–28 reflecting intestinal inflammation by non-invasive sampling. FC can also be used to identify patients with higher risk of relapse, as numerous studies reported a good sensitivity and specificity in predicting relapses29,30 and as well as in monitoring response after biologic therapy has been stopped. 31
The main limitations of CRP and stool biomarkers in monitoring CD is that their non-specificity for IBD and the lack of validated thresholds for active disease and remission. 19 A meta-analysis of 19 studies revealed that fecal calprotectin has a higher sensitivity in assessing endoscopic active disease compared to CRP. 17 Regarding postoperative follow-up, it appears that FC is more consistent with recurrence than CRP. 32
The CALM study revealed that treatment management based on both clinical symptoms and biomarkers achieved better endoscopic outcomes compared to decisions guided by symptoms alone. 33 At the same time, the 28 IBD specialist who established the goals of the “treat to target” patient management in the STRIDE program considered the decrease of CRP and calprotectin as an adjunctive target. 34
Very promising biomarkers are peripheral blood miRNAs, recent data suggesting miRNAs can distinguish active IBD subtypes from each other and from healthy controls. Furthermore, miRNAs levels have been shown to vary between active and inactive Crohn’s and UC patients in both colonic tissue and serum samples. 35
Endoscopic monitoring
Endoscopy is the gold standard for diagnosis and evaluation of mucosal inflammation in CD. In order to have an objective tool for assessment of disease extent and severity, two endoscopic scores are being used, CDEIS and SES-CD. The Rutgeerts score is widely used for postoperative recurrence.
The importance of endoscopic monitoring is supported by various studies stating that endoscopic remission is associated with a lower risk of complications and a better long-term outcomes.36,37
At the present, there is no consensus regarding follow-up intervals for endoscopic evaluation. Available data is presented in Table 1. We consider that endoscopy should be performed to all patients at diagnosis, when there is a need for therapy changes or when a suspicion of disease progression exists (based on symptoms or biomarkers). Patients with extensive colonic involvement and long-standing disease have an increased risk ok colorectal cancer 38 compared to general population. Following a screening colonoscopy protocol is necessary in order to detect early dysplasia and cancer, as recommended by current guidelines.
Small bowel evaluation using balloon-assisted endoscopy or push enteroscopy has the disadvantage of being invasive and time-consuming methods. An alternative is capsule endoscopy (CE), a non-invasive and well tolerated technique, with a crucial role in three settings: in suspected CD, unclassified IBD (IBDU) and established CD. 39 It can be useful in establishing diagnosis, assessing severity and disease extension.
In suspected CD, when endoscopic and imagistic results are inconclusive, CE resulted to have a higher diagnostic yield compared to computed tomography enterography (CTE) and ileocolonoscopy. 40 In IBDU patients, CE proved to be very useful in reclassification of patients, having a high sensitivity and specificity and a negative predictive value of 94% for the absence of lesions. 41
When it comes to patients with established CD, a discordance between symptoms, endoscopic and imagistic findings make CE evaluation a tool useful in monitoring and management of treatment. 42 In a retrospective study of 128 symptomatic IBD patients evaluated by CE, 61.6% of patients had a medication change and 12.8% suffered a surgical intervention. 43 Another study involving patients with established CD revealed that for more than 50% of patients therapy changes were made based on CE findings. 44
For an objective assessment of CE findings, two scores were validated, the Capsule Endoscopy CD Activity Index (CECDAI) and the Lewis score. 45 There is a correlation between the Lewis score and fecal calprotectin level, when FC is less than 100 µg/g. 46
We see a potential use of iterative capsule examinations especially with the new Crohn capsule in a treat to target approach.
Cross sectional imaging monitoring
Cross-sectional imaging techniques play a complementary role in assessing transmural inflammation and in identifying extra-intestinal complications of CD.
Ultrasound (US), a non-invasive, low-cost and radiation-free imagistic technique, is used in examining mainly the colon and the terminal ileum, evaluating the wall thickness and stiffness, loss of stratification and the presence of complications such as strictures, fistulae or abscesses. 47 Bowel vascularization can be evaluated by using color Doppler US or contrast-enhanced ultrasonography (CEUS). CEUS has a high precision in identifying active disease 48 and correlated well with MRI findings. 49
US can be used in monitoring CD patients as CEUS findings correlate with endoscopic severity 50 and disease activity, having a high sensitivity and specificity in predicting active disease. 51 Also, it has a role in assessing treatment response and efficacy52,53 and has good results in identifying postoperative recurrence. 54
Computed tomography enterography (CTE) is a useful tool in evaluating CD activity and severity, as well as extraluminal complications, with the benefit of distinguishing active inflammation from fibrosis. Even though it has the disadvantage of using ionizing radiation, CTE is widely available, has lower costs compared to magnetic resonance enterography (MRE) and can be used to monitor treatment response, as its results correlate well with disease activity.55,56 Additionally, it’s a very good option in emergency settings.
As CD patients usually need multiple imagistic evaluations during their lives, choosing a radiation free technique becomes relevant, especially in young patients. Considering these aspects, when available, MRE becomes the method of choice.
Both CTE and MRE offer additional information to ileocolonoscopy in evaluating disease activity, with MRE being superior to CTE in identifying intestinal strictures. 57 In a retrospective study of 50 CD patients, MRE findings indicated the need for treatment modification in 24% of patients who had endoscopic remission defined by a SES-CD <5. 58 MRE can be used in diagnosing small bowel inflammation and as well as a prognostic tool for relapses, 59 therefore it has found its place in monitoring CD patients.
The recent VERSIFY reports on MRI activity using the MaRIA score in an exploratory analysis, which proved to be another objective assessment of inflammation in selected CD patients, with a good agreement between the SES-CD and MaRIA scores. We believe that this is a major breakthrough in patient’s approach, that needs to be further evaluated in additional clinical trials. 60 The use of any of the imagistic methods depends on local expertise, availability and costs; for example, a comparison of medical services for IBD patients between Oxford (UK) and Milan (Italy) audited using the National UK audit tool, revealed that CT is more frequently used in Oxford while in Milan ultrasound is preferred. 61
Therapy monitoring
After starting treatment, patients are regularly evaluated. Clinical, biologic, endoscopic and imaging parameters are assessed, in order to monitor treatment efficiency and identify treatment related complications. Guidelines recommendations don’t offer firm follow-up periods. From our experience, in real-life settings, physicians adapt follow-up periods to patients’ needs and maintain a cautious attitude following short interval follow-up protocols.
Regarding treatment management, it was noticed that patients aged 65 or older are mainly treated with corticosteroids and very few are receiving anti-TNF drugs, 62 which in turn can lead to serious adverse effects and complications. Considering these results and the fact that use of corticosteroids is associated with serious infections 63 and low bone mineral density 64 among other side effects, we support the use of steroid sparing agents according to current guidelines, as well as a monitoring bone density every year.
Monitoring anti-drug antibodies is not recommended on routine basis, but it’s a cost-effective strategy 65 and it becomes very useful when patients lose response to treatment. Infliximab dosing based on therapeutic drug monitoring does not increases remission rates but it is associated with fewer flares. 66 IFX discontinuation and intestinal surgery were significantly less frequent with therapeutic drug monitoring (TDM) and investigating loss of response resulted in change in patient management. 67 Therapeutic drug monitoring may be helpful to adjust thiopurine and infliximab therapy, primarily in a reactive setting, in case of inefficacy and of occurrence of adverse event. 68 Additionally, the combination of calprotectin and trough concentration of infliximab can guide dose adjustment and increase the chances for endoscopic response and remission. 69 Recently a consensus has become available regarding the appropriate TDM of antiTNF agents. 12 More data is required to establish clear recommendations regarding other biologic agents.
The proinflammatory state of IBD patients plays a significant role in the microvascular dysfunction noticed in IBD patients. 70 Studies show that there is an increased risk of stroke, myocardial infarction and venous thromboembolism.71,72 TNF-alpha antagonists may reduce the cardiovascular risk, 73 while corticosteroids are associated with a higher risk of cardiac events. 74
Another important aspect is that patients treated with anti-TNF drugs have a higher risk of melanoma 75 and patients treated with thiopurines 76 a higher risk of non-melanoma skin cancer. Anti-TNF therapy is associated with the occurrence of psoriasiform skin lesions, with a higher prevalence in women and sometimes there is a need to withdraw biologic therapy. 77 Considering these aspects, we consider it is important for patients to receive dermatologic counseling, be monitored for skin cancer and use adequate sunscreen.
Monitoring disease in order to adjust treatment in time to prevent progression and complications becomes a requisite when it comes to CD patients. Pallotta and colleagues developed a risk score system that evaluates disease progression and the need for changing treatment, score that needs validation, but might become the objective tool we need in managing CD. 78 They identified 12 risk factors that subdivide in four risk scores predicting the need to use corticosteroids, the need to start azathioprine, anti-TNF drugs and the need of surgery.
Monitoring extraintestinal manifestations (EIM)
Up to 40% of IBD patients experience at least one EIM, which can manifest before IBD is diagnosed and be more debilitating than the intestinal disease itself. 79 More common in CD patients, some EIM can be life-threatening, such as primary sclerosing cholangitis (PSC) or venous thromboembolism. Most EIMs run in parallel with intestinal disease activity, with the exception of ankylosing spondylitis and uveitis and possibly PSC and pyoderma gangrenosum (PG). 80 Therefore, we suggest that EIM should be independently monitored. For example, the presence of PSC is an independent risk factor for the development of colorectal dysplasia and/or cancer in patients with IBD, leading to the recommendation for annual surveillance colonoscopies in affected patients from the time of first diagnosis of IBD. 81
There is no current guideline indication for EIM monitoring in remission periods. In the authors opinion, patients already diagnosed with at least one EIM should be monitored jointly with the rheumatologist/ophthalmologist, independent of intestinal disease activity. Patient awareness of extraintestinal complications related to their disease is still an improving effort, few of them being informed about the life-threatening potential of some EIM. 82 Therefore, it is of utmost importance to monitor EIM and to enhance patient education measures.
Conclusion
Over the past decade, we witnessed numerous breakthroughs in IBD research, but a standard in assessing therapeutic success is yet to be established. Clinical remission and mucosal healing remain for now the pursued treatment targets, and future prospective studies will show if this strategy is enough to alter disease course. The numerous monitoring tools, comprising clinical, biological, endoscopic and imaging scores or parameters provide help in guiding therapy, but are far from being perfect.
Footnotes
Author note
The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Author contributions
All authors contributed to this paper being involved in analysis and review of the literature, writing and editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.