
Abstract
The aim of this article is to investigate the effects of intra-abdominal infection on immunological function and high-mobility group box 1 protein (HMGB1)/toll-like receptor 4 (TLR4)/nuclear factor-κB (NF-κB) pathway in patients with severe acute pancreatitis (SAP). Clinical data of SAP patients were retrospectively analyzed. SAP patients were divided into intra-abdominal infection group (103 SAP patients) and control group (115 SAP patients without intra-abdominal infection). All patients were evaluated with the Acute Physiology and Chronic Health Evaluation (APACHE) II score. Enzyme-linked immunosorbent assay (ELISA) assays were used to detect the levels of serum endotoxin,
Introduction
Acute pancreatitis (AP) is an inflammatory disease of the pancreas autodigestion due to the activation of trypsinogen, which is caused by various factors such as gallstone, alcohol abuse, overeating, and hyperlipidemia. Severe acute pancreatitis (SAP), as severe form of AP, is characterized by multiple organ failure and systemic inflammatory response syndrome, with a mortality rate of up to 25% in patients who stay in hospital for more than 2 weeks.1,2 Intra-abdominal infection usually occurs in the late stage of SAP; the incidence of intra-abdominal infection is 40%–70% and the mortality is up to 50%. 3 Therefore, to explore the role of intra-abdominal infection in SAP has important clinical value.
Studies have reported that exogenous microorganisms could stimulate cells to release high-mobility group box 1 protein (HMGB1), which recruited the inflammatory cells such as neutrophil, monocytes, and lymphocytes to the damage sites. HMGB1 can further activate the downstream nuclear factor-κB (NF-κB) signaling pathway through interacting with toll-like receptor 4 (TLR4), which cause inflammatory cells to overwhelmingly release interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF)-α; reduce the contents of IgG, IgM, and IgA; and weaken the immune function of the organism. Thus, the activation of HMGB1/TLR4/NF-κB signaling pathway plays as inflammatory amplifiers in infectious diseases.4,5 In addition, the activation of HMGB1/TLR4/NF-κB signaling pathway is closely related to SAP. For example, Li et al. found high expression of HMGB1, TLR4, and NF-κB in SAP mice. And the targeted injection of recombinant HMGB1 protein into the pancreas activated the TLR4/NF-κB signaling pathway, leading to pancreatic tissue damage, while the effect was absent in the TLR4 knockout mice. 6 However, there is still a lack of clinical evidence on whether the aggravated symptoms in SAP patients caused by intra-abdominal infection are related to the immune disorder mediated by HMGB1/TLR4/NF-κB signaling pathway.
Therefore, 103 SAP patients with intra-abdominal infection were selected as intra-abdominal infection group in this study. And the mechanism of symptom aggravation and immune disorder in SAP patients caused by intra-abdominal infection were investigated in terms of HMGB1/TLR4/NF-κB signaling pathway by comparing with 115 SAP patients in the control group without intra-abdominal infection.
Materials and methods
General information
A total of 103 SAP patients with intra-abdominal infection admitted to the First Affiliated Hospital of Zhengzhou University between February 2016 and February 2018 were selected as intra-abdominal infection group, while 115 SAP patients without intra-abdominal infection admitted in the same period were selected as control group. A retrospective analysis of the clinical data of two groups was performed. The general information of age, sex, body mass index (BMI), and etiology of two groups were compared. The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (No. Speedy trial-2016-13) and informed consents were obtained from all the patients or their families.
Inclusion criteria and exclusion criteria
Inclusion criteria: (1) SAP was diagnosed according to the guidelines for the management of AP in 2014. 7 AP was defined by meeting two of three criteria, such as acute upper abdominal pain radiated to the back, serum amylase or lipase >3X upper limit of normal, imaging of pancreatic necrosis, and effusion. AP combined with one or more organ failure was defined as SAP. (2) The intra-abdominal infection was diagnosed according to the diagnostic criteria for hospital infection in 2001. 8 The standard included positive abdominal computed tomography findings of disappeared bowel sounds and bubbles appeared around the pancreas, white blood cell count >1.2 × 109, temperature >38°C, heart rate >90 times/min, and positive peritoneal cultures. Exclusion criteria: (1) infection occurred in the past 3 months; (2) combined with complications such as liver and kidney dysfunction, cardio-cerebrovascular disease, and autoimmune diseases; and (3) patients with incomplete clinical data.
Measurement indicators
Once diagnosed as SAP patients with intra-abdominal infection, all patients were evaluated with the Acute Physiology and Chronic Health Evaluation (APACHE) II score. It is composed of acute physiology score, age score, and chronic health score, with a total score of 0–71 points. The higher the score, the worse the prognosis. 9
Fasting venous blood (5 mL) was collected. ELISA was used to detect the content of intestinal barrier function indicators, including serum endotoxin (Jingmei, JM-03620H1, China),
Western blotting
Western blotting (WB) was used to determine the levels of TLR4 and NF-κB in peripheral blood lymphocytes of all patients. After blending 2.5 mL of anticoagulant blood with 2.5 mL of saline, the mixture was slowly added to 5 mL of lymphocyte separation liquid (Huayueyang, GH5003, China). Then, the mixed solution was divided into four layers including erythrocyte layer, transparent separation fluid layer, milky lymphocyte layer, and plasma layer from the bottom up after centrifugation for 20 min at 400g. The lymphocyte was namely extracted from lymphocyte layer. A total of 106 cells were added to 100 μL of RIPA lysate (Beyotime, P0013, China) and fully lysed for 5 min. Homogenates were centrifuged at 12,000g for 5 min, and supernatants were taken for bicinchoninic acid (BCA) protein quantification (Beyotime, P0012, China). The 40 μg protein was separated by polyacrylamide gel electrophoresis and transferred to a polyvinylidene difluoride membrane. Membranes were then blocked in 5% skim milk for 2 h. Then, membranes were respectively incubated with the diluted solution of following rabbit anti-human antibodies including anti-TLR4 antibody (1:500, Abcam, ab13556, UK), anti-NF-κB antibody (1:1000, Abcam, ab32360, UK), and anti-GAPDH (glyceraldehyde 3-phosphate dehydrogenase) antibody (1:2,500, Abcam, ab9485, UK) at 4°C overnight. The membranes were then thoroughly washed for three times and incubated with the anti-rabbit horseradish peroxidase-coupled secondary antibody (Boster, BA1056, China) at a dilution of 1:2000. The membranes were impregnated with the enhanced chemiluminescence substrate (Beyotime, P0018, China), and specific protein bands were photographed using gel imager (Bio-Rad, GelDoc 2000, USA). The gray-scale value of each band was measured using GraphPad Prism 6.0 software, and the gray-scale ratio of target protein to GAPDH in the control group was set as 1.0.
Statistical analysis
All statistics were completed by the statistical software SPSS 20.0. The significance of differences in group means for continuous variables expressed as the mean ± standard deviation was determined using the Student’s t test. Differences between group means for nominal variables expressed as case and percentage were assessed by the chi-square test. P < 0.05 is considered statistically significant.
Results
Comparisons of the general characteristics
The results in Table 1 indicated that there were no statistically significant differences in age, sex, BMI, and etiology of the two groups (all P > 0.05).
Comparisons of the baseline characteristics of the two groups.

BMI: body mass index.
Comparisons of APACHE II score and intestinal barrier function
In Figure 1, the results suggested that the levels of APACHE II score, serum endotoxin,
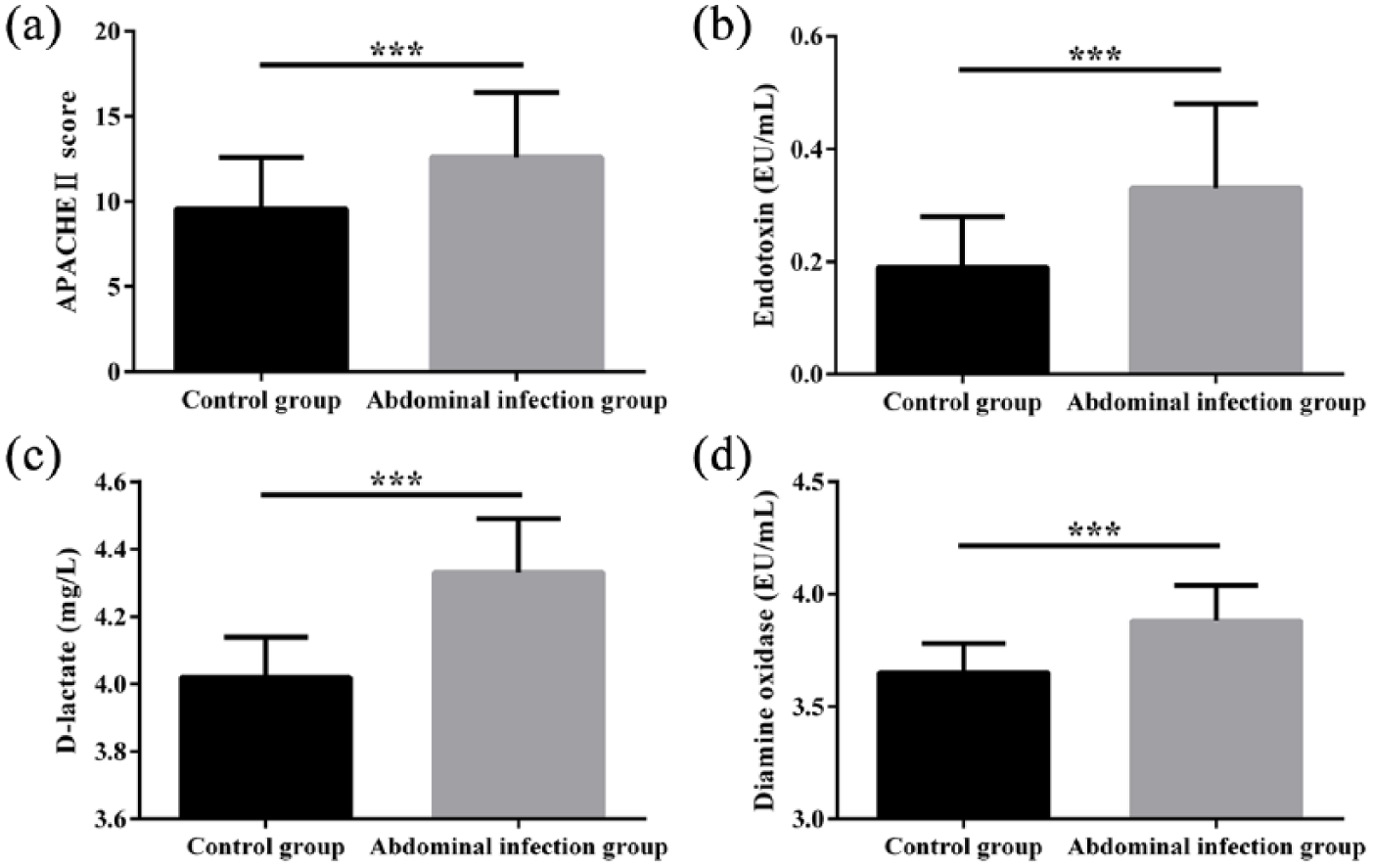
Comparisons of APACHE II score and intestinal barrier function of the two groups: (a) APACHE II score, (b) serum endotoxin, (c)
Comparisons of immune function and HMGB1 expression
The results in Figure 2 showed that the levels of serum IgG, IgM, and IgA in the intra-abdominal infection group were lower than those in the control group, while the levels of serum IL-1β, IL-6, TNF-α, and HMGB1 in the intra-abdominal infection group were higher than those in the control group (all P < 0.05).

Comparisons of immune function and HMGB1 expression of the two groups. (a) IgG, (b) IgM, (c) IgA, (d) IL-1β, (e) IL-6, (f) TNF-α, and (g) HMGB1. Data are expressed as mean ± SD. Compared with control group, *P < 0.05, **P < 0.01, ***P < 0.001.
Comparisons of TLR4 and NF-κB protein expression in peripheral blood lymphocytes
In Figure 3, the results indicated that the relative expression of TLR4 and NF-κB in peripheral blood lymphocytes in the intra-abdominal infection group increased significantly compared with control group (TLR4: 2.35 ± 0.48 vs 1.00 ± 0.24, NF-κB: 2.18 ± 0.40 vs 1.00 ± 0.21, all P < 0.001).

Comparisons of TLR4 and NF-κB protein expression in peripheral blood lymphocytes of two groups. (a) and (b) TLR4 and NF-κB protein expression detected by WB. (c) and (d) Comparison of the relative expression of TLR4 and NF-κB protein. Data are expressed as mean ± SD. Compared with control group, ***P < 0.001.
Discussion
Intra-abdominal infection occurs mainly with SAP and is closely related to the severity of SAP. Lv and Huo
10
reported that the risk factors for intra-abdominal infection included high APACHE II score, high Ranson score, and shock, and the main reasons included severe extent of tissue necrosis and impaired intestinal barrier function. In this study, we found that APACHE II score, serum endotoxin,
HMGB1, a single polypeptide chain, is ubiquitous in the nucleus of mammalian cells, playing an important role in nucleosome stabilization and DNA transcription. Moreover, HMGB1 is a proinflammatory cytokine, regulating the recruitment of inflammatory cells and the release of inflammatory mediators; therefore, the increase in serum HMGB1 occurs in a series of inflammatory diseases, such as sepsis, trauma, and acute myocardial infarction. Yasuda et al. 11 reported that serum HMGB1 was significantly increased by nearly three times higher within 72 h in SAP patients, and elevated levels were associated with organ dysfunction and infection. Our results showed that serum IgG, IgM, and IgA levels were lower than those in the control group, while IL-1β, IL-6, and TNF-α levels were higher than those in the control group. Furthermore, serum HMGB1 significantly increased in the intra-abdominal infection group, indicating that intra-abdominal infection can inhibit the immune function and aggravate the inflammatory reaction in SAP patients, which may be related to enhanced release of HMGB1.
TLR4, the main effector molecule of HMGB1, recruits MyD88 and thus activates the downstream NF-κB. Activated NF-κB is transported from the cytoplasm to the nucleus, which induces the expression of inflammatory factors such as IL-1β, IL-6, and TNF-α. Pan et al. 12 found that the augmenter of liver regeneration can reduce serum amylase and lipase in SAP mice and alleviate pathological damage of pancreatic tissue, which is related to the inhibition of HMGB1/TLR4/NF-κB pathway. Our research showed that the relative expression of TLR4 and NF-κB in peripheral blood lymphocytes in the intra-abdominal infection group was significantly higher than those in the control group, suggesting that intra-abdominal infection can promote the release of HMGB1, and TLR4/NF-κB pathway in lymphocytes can be further activated.
In conclusion, intra-abdominal infection may lead to intestinal barrier dysfunction, aggravated inflammatory reaction, and immune dysfunction in SAP patients. It may be related to the activation of HMGB1/TLR4/NF-κB pathway caused by intra-abdominal infection.
Footnotes
Acknowledgements
The authors thank the reviewers for their useful comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.