
Abstract
Patients with acute pancreatitis (AP) often suffer tough complications, some of which are fatal. The early diagnosis and definite treatment of central nervous system (CNS) complications have not been fully achieved yet, which seriously affects the mortality of severe acute pancreatitis (SAP). We present a case of infected pancreatic necrosis (IPN) in a 62-year Chinese man who developed acute herpes simplex encephalitis (HSE) caused by herpes simplex virus type 1 (HSV-1) after favorable minimally invasive retroperitoneal approaches (MIRAs). The patient was successfully treated with 115 days stayed in our hospital. The MIRAs included image-guided retroperitoneal percutaneous catheter drainage (PCD), nephroscopic pancreatic necrosectomy (NPN), and ultrasonic pneumatic lithotripsy system (UPLS) assisted non-narcotic sinus track necrosectomy (NSN). HSE is relatively rare and potentially life threatening. We attempt to discuss the probable risk factors and how the relatively rare HSE are related to the patients of SAP with latent HSV.
Introduction
Central nervous system (CNS) infections are potentially life threatening in patients of severe acute pancreatitis (SAP). Bacterial encephalitis is the most common syndrome, however viral encephalitis is relatively rare.1–4 We present a case of herpes simplex encephalitis (HSE) caused by herpes simplex virus (HSV). The patient was diagnosed of infected pancreatic necrosis (IPN), and favorable outcomes was revealed after conducting minimally invasive approaches (MIAs) followed by step-up strategy. Few in articles have reported SAP complicated with HSE. We attempt to discuss the probable risk factors and how the relatively rare HSE are related to the patients of SAP with latent HSV.
Case presentation
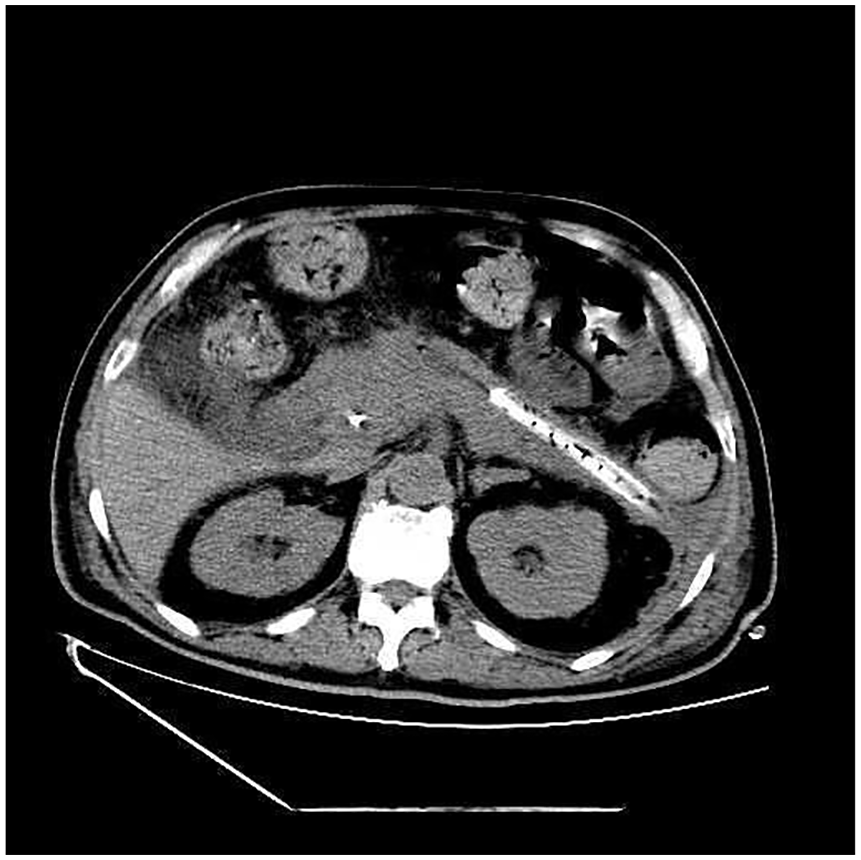
A 62-year Chinese man was hospitalized on March 17, 2019, with a complaint of acute epigastric pain, nausea, bloating, and fever for 3 days, and was gradually worsening. A medical history of biliary stones and diabetes mellitus was revealed. On physical examination, mild-fever, increased heart rate, rapid respiration, abdominal distention, and upper abdominal pain were revealed. Laboratory examination results were as follows: serum amylase 2530 U/L (0–100 U/L), urine amylase 3136 U/L (0–500 U/L), leukocyte count 12.1 × 109/L (3.5–9.5 × 109/L), and hemoglobin 123 g/L (115–150 g/L). Computed tomography (CT) scan showed peripancreatic collections and choledocholithiasis (Figure 1). Biliary cause of acute pancreatitis (AP), acute cholecystitis, choledocholithiasis, and cholangitis were diagnosed. The step-up treatment strategy was decided in the multidisciplinary team (MDT) meeting by pancreas surgeons, digestive specialist, radiologists, interventional ultrasound specialist, anesthesiologist, and intensive care specialist. Urgent peripancreatic percutaneous catheter drainages (PCDs), endoscopic sphincterotomy (EST), and endoscopic nasobiliary drainage (ENBD) were solved on the admitted day followed by guidelines. Five weeks after the first-stage treatment of intensive care, fasting, fluid resuscitation, antibiotics (cefoperazone sodium and sulbactam sodium), enteral tube feeding, symptoms of remittent fever (38.5°C–39.0°C), ongoing gastric outlet obstruction, high leukocyte count (>15.0 × 109/L), and sputum and bile positive culture (Enterococcus faecalis and Citrobacter freundii) were observed. Massive collections and gas sign in walled-off necrosis were showed on CT scan (Figure 2). Infected pancreatic necrosis (IPN) was defined according to the 2012 Atlanta classification. Clinical deterioration positively indicated step-up approaches. Since the distance between main walled-off necrosis cavity and gastric wall was more than 1 cm, we opted for retroperitoneal procedures.

Computed tomography of the abdomen after hospitalization (axial view), mass peripancreatic collections.

Computed tomography of the abdomen before necrosectomy (axial view), mass infected peripancreatic necrosis.
On May 4, nephroscopic pancreatic necrosectomy (NPN) was performed followed by standard retroperitoneal procedure. Percutaneous accesses to the necrosis were dilated by Seldinger technique. Massive pus and necrosis were extracted and aspirated with the assistance of nephroscopic forceps and ultrasonic pneumatic lithotripsy system (UPLS). Two 24F irrigating tubes for postoperative lavage were placed in the cavity. Continuous irrigation by normal saline solution was started after surgery at a rate of 100–125 mL/h. Postoperative temperature and leukocyte count were rapidly declined to normal level. Non-narcotic sinus track necrosectomy (NSN) performed four times at an interval of 7–10 days to debride the remained necrosis according to repeated CT scans. No intraoperative and postoperative complications were found. Improvement on images (Figure 3) and clinical symptoms showed favorable outcomes as expected.
Computed tomography of the abdomen after necrosectomy (axial view), significant improvement of peripancreatic necrosis.
Outbreak, aphasia, hypotonia, stiff neck, lethargy, and epilepsy (GCS, Glasgow Coma Scale of 8/15) happened to the patient on June 5. No obvious abnormality was detected on routine laboratory examination, emergent head CT scan and magnetic resonance imaging (Figure 4). The critical treatment prescription was set in the MDT meeting by neurologist, infectious disease specialist, radiologists, and intensive care specialist. Low serum leukocyte count, normal serum electrolytes, negative blood culture, normal intracranial pressure (ICP, <160 mmH2O), normal cerebrospinal fluid (CSF) glucose (4.16 mmol/L), high CSF protein (125.2 mg/dL), mild elevation of CSF leukocyte count (8/μL) suspected virus, or autoimmune encephalitis. The patient received a virological diagnosis based on the detection of viral genome in CSF samples. Herpes simplex virus type 1 (HSV-1) was detected by DNA polymerase chain reaction (PCR), HSV-1 caused HSE was diagnosed. Recovery of consciousness occurred 5 days after principal therapy of mechanical ventilation, antiviral agent (acyclovir and sodium phosphonate injection), and antiepileptic agent (sodium valproate injection). CNS dysfunction including aphasia, epilepsy, and consciousness disorder dissolved in 2 weeks. Irrigation was stopped according to the control of symptoms, clear draining fluid, and improved CT scan. The patient was discharged home with drains on July 6 and followed up at 3–4 week intervals with drains being shortened until removal. No neurological sequelae and recurrent infection were found after half a year follow-up. The total days spent in the hospital were 112.

Magnetic resonance image of the head (axial apparent diffusion coefficient), no obvious lesions.
Discussion
There have been substantial improvements in the management of AP since the publication of the step-up treatment guidelines.5–9 However it is clear that such a common disease associated with mortality up to 30% in severe cases due to the development of pancreatic necrosis, subsequent infection, and multiple system organ failure (MSOF).10–14 Organ failure (OF) usually develop early within a few days of onset of AP, the commonest of which is respiratory failure. However it may also develop late due to sepsis and prolonged hospitalization. CNS complications are relatively rare and potentially life threatening if not diagnosed and treated early, however, the early diagnosis and definite treatment have not been fully achieved yet, which seriously affects the mortality of SAP. The patient of AP was over early systemic inflammatory response syndrome (SIRS) and developed into infected pancreatic necrosis (IPN) in this case. We followed the step-up strategy and minimally invasive retroperitoneal approach (MIRA), clinical improvement, and postoperative CT scans showed favorable outcomes due to the effective approach.
In this case, the acute onset of characteristic syndromes pointed to suspected CNS complication. We’ve received several CNS complications including pancreatic encephalopathy (PE), subsequent encephalopyosis, cerebral embolism, 14 etc., and their clinical manifestations were different from it. Normal CSF glucose, high protein, leukocyte count 8/μL suggested virus or autoimmune encephalitis. Herpes simplex virus type 1 (HSV-1) was detected from CSF samples, and diagnosis of HSE was confirmed in combination with clinical findings.
HSE is caused by primary HSV infection in 1/3 of cases while the rest are due to reactivation of a latent HSV infection.15–17 It is generally recognized that HSV remains in latent form in sensory ganglia. The virus can extend from an adjacent focus, hematogenous dissemination, or intraneural passage. In this case, both epidemiological characteristics and clinical symptoms point to recurrence of latent infection. CNS is protected by the blood–brain barrier (BBB) but still highly vulnerable to various bacteria, viruses, fungi, or parasites which can migrate into it. The initial clinical manifestation of many CNS infections is nonspecific, consisting of high fever, headache, stiff neck, and consciousness disorder. Early differential diagnosis and antiviral agent administration are critical to the prognosis of HSE. HSE is specifically associated with a series of frontotemporal features such as aphasia, personality changes, and epilepsy. Even after regular treatment, there are still about 10% of the patients, especially the severe illness, will leave different degrees of mental retardation, epilepsy, paralysis, and other sequelae. No CNS symptoms was revealed after treatment in this case.
Although molecular methods are predicted to be widely used in diagnosing CNS infections, clinical findings still need to be considered in combination.18,19 We reviewed literatures about pancreatitis complicated with HSE and found scarce evidence of relevant cases and reviews. The relationship between pancreatic complications and causes of HSE is rarely mentioned.
Conclusions
HSE is relatively rare and potentially life threatening in patients with acute pancreatitis. Systemic inflammatory reaction, pancreatic infection, and insufficient immune function are critical mechanisms of activation of latent herpes virus. Patients with any mild abnormal mental symptoms during treatment of pancreatitis should be vigilant enough and timely. CNS complications can be diagnosed early by pertinent examinations, and can be effectively prevented from worsening or even death by effective treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
Dr. Bei Lu, Dr. Yang Cai, Dr. Junjie Yin, Dr. Jingrui Wang, Dr. Zhong Jia, Dr. Wei Hu, Dr. Jianhua Fang were involved in compilation of the data and drafting of the article. All authors read and approved the final manuscript.
Ethics approval
Ethical approval to report this case was obtained from Ethic Committee of Hangzhou First People’s Hospital (approval number: 2020-009-01).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Consent to publish
The authors certify that they have obtained all appropriate written informed consent forms. In the forms, the patient had given written informed consent to publish in the journal. The patient understood that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Availability of data and materials
All data of this case report is included in this published article.