
Abstract
Stroke is the major cause of death and disability worldwide and ischemic stroke contributes 80% among them. Although limited number of patients display hemorrhagic stroke (HS), the disability and death rate are higher in HS. Several studies have been reported on identification of suitable markers for diagnosis of stroke, but none of them holds true worldwide. These observations direct toward identification of population-specific biomarker of stroke. In this study, we screened various blood biomarkers in a large cohort of well-characterized Chinese stroke patients and healthy controls. A total of 308 stroke patients including 262 acute ischemic stroke (AIS) patients and 42 HS patients were enrolled in the study and blood samples were collected within 6–24 h of stroke onset. In addition, 46 stroke mimic subjects were included for comparison of blood markers with stroke patients. Furthermore, healthy controls (n = 200) and patient controls (n = 125) from similar ethnic group were enrolled in the study. Biomarkers (S100 calcium-binding protein B (S100B), C-reactive protein (CRP), interleukin 6 (IL-6), plasminogen activator inhibitor-1 (PAI-1), matrix metallopeptidase 9 (MMP-9), P-selectin, intercellular adhesion molecule 1 (ICAM-1), tumor necrosis factor α (TNF-α), low-density lipoprotein (LDL) cholesterol, interleukin 10 (IL-10), nitric oxide (NO), and glial fibrillary acidic protein (GFAP)) were quantified by ELISA. Blood levels of S100B, CRP, IL-6, PAI-1, MMP-9, P-selectin, ICAM-1, and TNF-α were significantly higher in AIS and HS patients compared to healthy controls, patient controls, and stroke mimic patients. Receiver operating characteristic (ROC) curve analysis revealed CRP, IL-6, PAI-1, P-selectin, and TNF-α as possible biomarkers for AIS patients, and HS patients can be diagnosed based on S100B, IL-6, PAI-1, MMP-9, and TNF-α. Interestingly, significant area under ROC curves were observed for plasma S100B and CRP for differentiating AIS from HS. The results of this study validated certain blood parameters used for diagnosis of AIS or HS in Chinese patients. Furthermore, S100B and CRP are promising biomarkers for differentiation of AIS from HS.
Introduction
Stroke is a sudden neurologic dysfunction involving focal area of brain due to interrupted or reduced blood supply. Broadly, stroke can divided into two types. Ischemic stroke due to blockage in artery and bursting or leaking of blood vessel is known as hemorrhagic stroke (HS). Ischemic stroke is most prevalent (80%–85%) compared to hemorrhagic type (20%–15%) worldwide.1–3 In contrast, higher frequency of post-stroke bad prognosis has been reported in HS than ischemic stroke.2–4 A recent report in Chinese population showed prevalence of stroke was 1596 per 100,000 subjects, incidence of 345.1 in 100,000 per year, and majority of stroke patients experienced ischemic stroke (77.8%). 5 As the management and treatment strategies of stroke subtypes are different, lowering of blood pressure is beneficial in treatment of HS as it hampers hematoma growth, 6 minimizes chances of rebleeding, 7 and improves clinical conditions. 8 On the other way, reduced blood pressure increases clinical severity and deleterious in ischemic stroke.9,10 Thus, proper clinical differentiation between subtypes of stroke is essential for management and treatment of patients.
Several investigations have been carried out in different population to identify possible biomarkers for stroke or those who could differentiate efficiently between two clinical subtypes of stroke. 11 Although larger number of biomolecules were reported to be effective markers of stroke subtypes, those could not hold true in all ethnic groups. 12 These observations direct a population-specific identification of biomarkers for stroke. A wide range of biomolecules have been investigated in Chinese population; 11 however, none of the reports was properly designed or included decent sample size.
The aim of this study is to identify possible biomarkers for stroke patients and also those who could differentiate efficiently between subtypes of stroke. In this report, we tested various biomarkers in well-characterized clinical groups including decent sample size, namely, acute ischemic stroke (AIS), HS, healthy controls, patient controls, and stroke mimic patients.
Materials and methods
Study samples
Patients those were admitted to emergency department of Zhucheng People’s Hospital, Zhucheng, with an acute stroke during 2014–2017, were enrolled in this study. A total of 350 suspected stroke patients were evaluated and out of them, 262 were of AIS, 42 had HS, and 46 patients showed mimicking stroke phenotype. The clinical categorization was performed according to an earlier report. 13 Furthermore, for statistical comparison, we enrolled healthy controls (n = 200) and patient controls (n = 125) from similar population. Healthy controls had no history of stroke, any neurological disorders, or autoimmune diseases. Patient controls were those who were accompanying the patients and preferably next of kin of patients. About 5 mL of blood samples was collected from all individuals in ethylenediaminetetraacetic acid (EDTA) or heparin. The study protocol was approved by Institutional Human Ethical Committee of Zhucheng People’s Hospital, Zhucheng. Written informed consents were obtained from all participants.
Biomarker quantification
Blood samples were centrifuged at 10,000g for 10 min, and plasma was extracted as supernatant and stored at 80°C until used. All plasma samples were quantified for S100 calcium-binding protein B (S100B), C-reactive protein (CRP), interleukin 6 (IL-6), plasminogen activator inhibitor-1 (PAI-1), matrix metallopeptidase 9 (MMP-9), P-selectin, intercellular adhesion molecule 1 (ICAM-1), tumor necrosis factor α (TNF-α), interleukin 10 (IL-10), nitric oxide (NO), and glial fibrillary acidic protein (GFAP) by enzyme-linked immunosorbent assay (ELISA; R&D Systems). Low-density lipoprotein (LDL) cholesterol was also quantified by ELISA (Abcam).
Statistical analysis
All statistical analysis was performed in GraphPad prism software (version 6.01). Baseline characteristics of healthy controls and other clinical categories were compared by Fisher’s exact test or Student’s t test (age comparison). Levels of biomarkers among different groups were compared by one-way analysis of variance (ANOVA) followed by Tukey’s post-test. All molecules were tested for their biomarkers’ properties by receiver operating characteristic (ROC) curve. A P value less than 0.05 was considered to be significant.
Results
Baseline characteristics
A total of 350 subjects with stroke phenotype were enrolled in this study. After detailed clinical and biochemical analysis, patients were further grouped into AIS (n = 262), HS (n = 42), and stroke mimicking patients (n = 46). Baseline data are shown in Table 1. Age and gender distribution among these clinical categories were comparable. Furthermore, patient controls those accompanying patients and healthy controls from similar ethnicity were included in the present investigation. The mean age of patient controls was comparably lower than other clinical categories. History of previous stroke was more frequent in HS patients (24%) compared to AIS (20%) and stroke mimic patients (15%). Clinical phenotypes such as hypertension and diabetic were significantly more prevalent in AIS and HS when compared to healthy controls. In addition, frequency of habit of smoking and consumption alcohol was higher in HS and AIS compared to healthy controls.
Baseline characteristics of patients and controls.
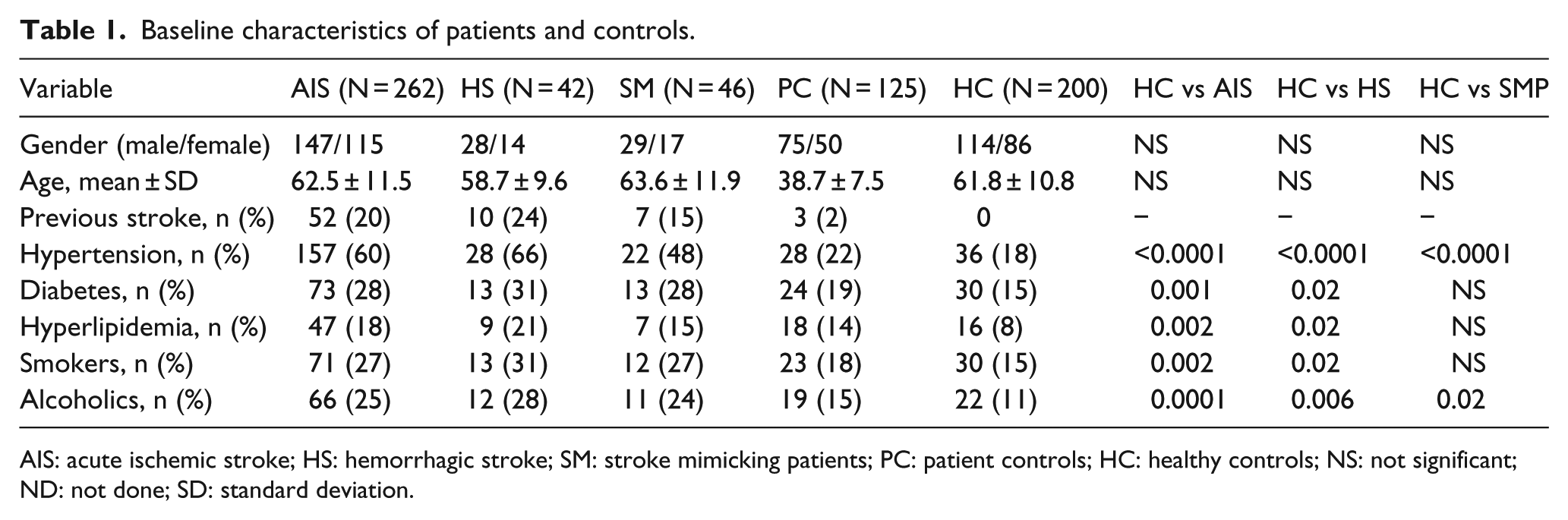
AIS: acute ischemic stroke; HS: hemorrhagic stroke; SM: stroke mimicking patients; PC: patient controls; HC: healthy controls; NS: not significant; ND: not done; SD: standard deviation.
Plasma levels of various biomarkers in different clinical categories
Plasma levels of S100B, CRP, MMP-9, TNF-α, IL-6, PAI-1, ICAM-1, P-selectin, LDL cholesterol, IL-10, NO, and GFAP were quantified by appropriate methods, and results are plotted in Figure 1. The mean levels of biomolecules among different clinical groups were compared by ANOVA followed by Tukey’s post-test. Hemorrhagic shock patients displayed significantly higher levels of S100B compared to AIS (P < 0.0001), stroke mimic case (P < 0.0001), patient controls (P < 0.0001), and healthy controls (P < 0.0001). Similar patterns were also observed in distribution of MMP-9 (Figure 1(c)), TNF-α (Figure 1(d)), PAI-1 (Figure 1(f)), and P-selectin (Figure 1(h)). In contrast, AIS patients had elevated CRP than other clinical categories including HS (stroke mimic: P < 0.0001; patient controls: P < 0.0001, healthy controls: P < 0.0001, and HS: P < 0.0001) (Figure 1(b)).

Plasma levels of different blood parameters in various clinical categories: (a) S100B, (b) CRP, (c) MMP-9, (d) TNF-α, (e) IL-6, (f) PAI-1, (g) ICAM-1, (h) P-selectin, (i) LDL cholesterol, (j) IL-10, (k) NO, and (l) GFAP were quantified in different clinical categories, namely, acute ischemic stroke (AIS: n = 262), hemorrhagic stroke (HS: n = 42), stroke mimicking patients (SM: n = 46), patient controls (PC: n = 125), and healthy controls (HC: n = 200), and compared by analysis of variance followed by Tukey’s post-test. Plots are shown as mean and standard deviation. A P value less than 0.05 was considered as significant.
Mean plasma levels of ICAM-1 and IL-6 in AIS and HS were higher compared to other clinical categories. However, difference between stroke patients, that is, ischemic and hemorrhagic, could not reach significance levels (Figure 1(e) and (g)).
Although several studies have demonstrated possible biomarker properties of other biomolecules such as LDL cholesterol, IL-10, NO, and GFAP, the distribution of those biomarkers was comparable in our present investigations (Figure 1(i)–(l)), indicating that these biomarkers are not valid in studied population.
Biomarkers analysis for AIS
We observed significant elevated S100B, CRP, IL-6, PAI-1, MMP-9, P-selectin, ICAM-1, and TNF-α in AIS when compared to healthy controls and patient controls. Next, we hypothesized possibilities of these molecules as biomarker for diagnosis of AIS. ROC curve analysis was performed for above-mentioned biomolecules, and results are shown in Figure 2. Out of eight tested molecules, CRP (area: 0.99, P < 0.0001), IL-6 (area: 0.96, P < 0.0001), PAI-1 (area: 0.99, P < 0.0001), P-selectin (area: 0.91, P < 0.0001), and TNF-α (area: 0.99, P < 0.0001) showed significant ROC area and could be relevant biomarkers for diagnosis of AIS in Chinese population. Other molecules such as S100B (area: 0.89), MMP-9 (area: 0.62), and ICAM-1 (area: 0.81) failed to show as valid potent biomarkers for diagnosis of AIS.

Receiver operating characteristic (ROC) curve of various plasma parameters with acute ischemic stroke: (a) S100B, (b) CRP, (c) IL-6, (d) PAI-1, (e) MMP-9, (f) P-selectin, (g) ICAM-1, and (h) TNF-α in acute ischemic stroke patients (n = 262) with reference to healthy controls (n = 200). ROC curve was plotted and analyzed in GraphPad prism.
Biomarker analysis for HS
Biomolecule screening in different clinical categories revealed higher plasma parameters such as S100B, CRP, IL-6, PAI-1, MMP-9, P-selectin, ICAM-1, and TNF-α in HS in comparison with healthy controls. Thus, we tested possibility of these molecules to be biomarkers for diagnosis of HS by ROC curve analysis. As shown in Figure 3, various molecules such as S100B (area: 0.98, P < 0.0001), IL-6 (area: 0.97, P < 0.0001), PAI-1 (area: 0.99, P < 0.0001), MMP-9 (area: 0.95, P < 0.0001), and TNF-α (area: 1.0, P < 0.0001) showed significant ROC curve area and qualified for possible potent biomarker for diagnosis of HS. Other plasma parameters were marginally qualified to be a biomarker due to lesser ROC curve area compared to other molecules (CRP: area = 0.88, P-selectin: area = 0.89, and ICAM-1: area = 0.88).

Receiver operating characteristic (ROC) curve of various plasma parameters with hemorrhagic stroke: (a) S100B, (b) CRP, (c) IL-6, (d) PAI-1, (e) MMP-9, (f) P-selectin, (g) ICAM-1, and (h) TNF-α in hemorrhagic stroke patients (n = 42) with reference to healthy controls (n = 200). ROC curve was plotted and analyzed in GraphPad prism.
Biomarkers for differentiation of AIS and HS
We observed elevated plasma levels of S100B, MMP-9, TNF-α, PAI-1, and P-selectin in HS compared to AIS. In contrast, AIS patients displayed high levels of CRP than HS. Furthermore, biomarker analysis revealed CRP and P-selectin as possible markers for AIS, and, on the other hand, S100B and MMP-9 were restricted to HS. To find out a valid biomarker which can differentiate between AIS and HS, we performed ROC curve analysis of S100B, CRP, MMP-9, TNF-α, PAI-1, and P-selectin, and results are shown in Figure 4. Although area under ROC curve was not highly significant, S100B (area: 0.88, P < 0.0001) and CRP (area: 0.85, P < 0.0001) can be possible biomarkers for differentiation of stroke type.
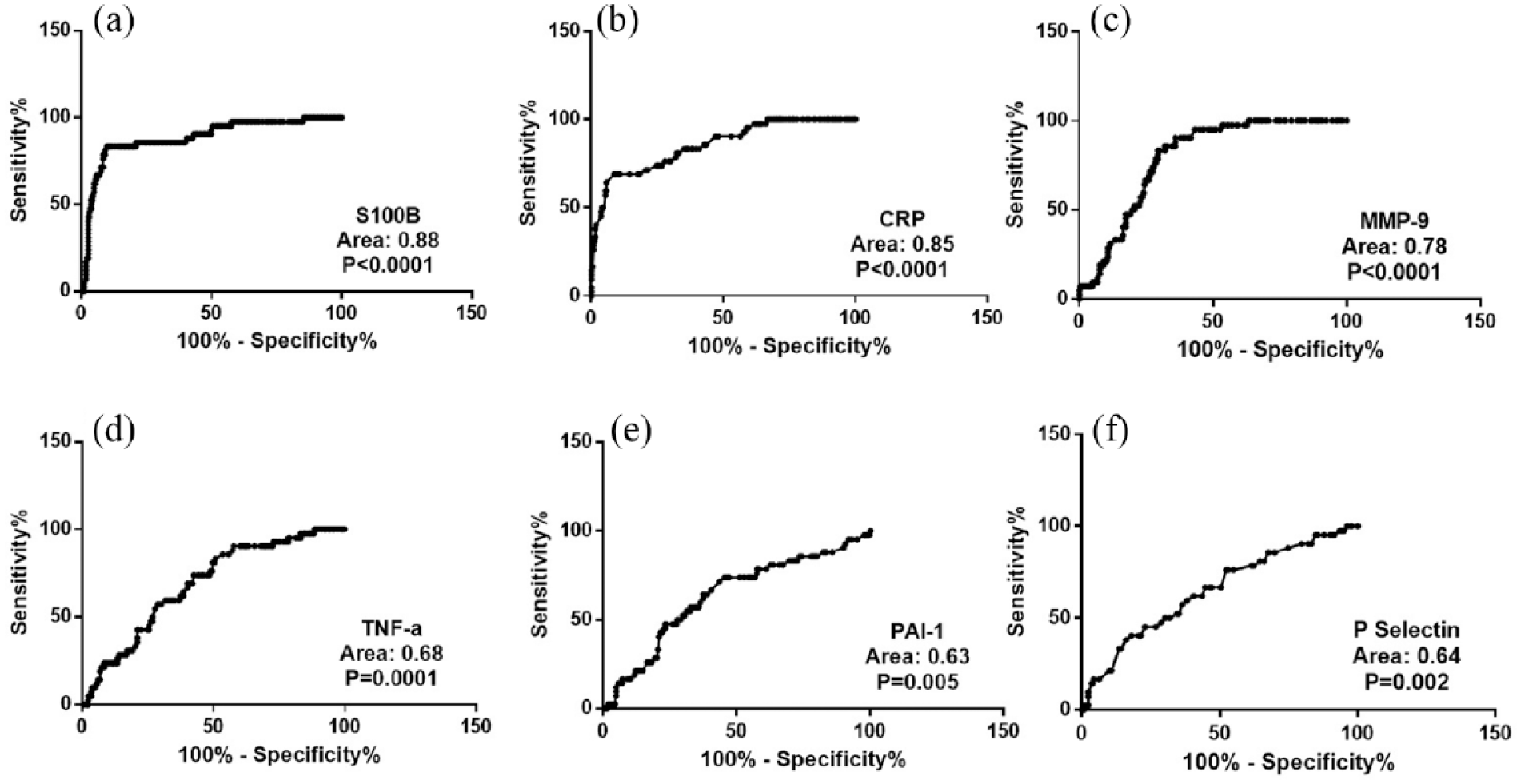
Receiver operating characteristic (ROC) curve of various plasma parameters in acute ischemic stroke with reference to hemorrhagic stroke plotted for (a) S100B, (b) CRP, (c) MMP-9, (d) TNF-α, (e) PAI-1, and (f) P-selectin in acute ischemic stroke patients (n = 262) and hemorrhagic stroke patients (n = 42). ROC curve was plotted and analyzed in GraphPad prism.
Discussion
In this study, we performed a hospital-based case–control investigation to validate biomarkers for stroke in a Chinese cohort. We screened 12 biomarkers those were reported earlier in different population for diagnosis of stroke and revealed CRP, IL-6, PAI-1, P-selectin, and TNF-α as possible biomarkers for AIS. In addition, HS patients can be diagnosed with elevated plasma molecules, namely, S100B, IL-6, PAI-1, MMP-9, and TNF-α. Interestingly, biomolecules such as S100B and CRP are important in differentiation between AIS and HS.
Several biomolecules have been screened in different cohorts to identify relevant markers for diagnosis of stroke. In the present investigation, we observed elevated S100B, CRP, MMP-9, TNF-α, IL-6, PAI-1, ICAM-1, and P-selectin in AIS patients when compared to healthy controls. Earlier reports also showed higher levels of S100B,13–16 CRP,14,17–20 IL-6,6,13,21,22 MMP-9,13–15,23,24 TNF-α,19,25 PAI-1,13,26 ICAM-1,26–28 and P-selectin26,29 in AIS cases than healthy controls or stroke mimic cases and proposed consideration of these molecules as important parameters for diagnosis and discrimination of stroke patients from mimic phenotype. However, in the current investigation, plasma levels of IL-6 were comparable in AIS and stroke mimic cases. We further tested whether these elevated plasma parameters in AIS can be treated as valid biomarkers. To meet this, we performed ROC curve analysis of biomolecules and observed significant area under curve for CRP (0.99), IL-6 (0.96), PAI-1 (0.99), P-selectin (0.91), and TNF-α (0.99) suggesting that these molecules may be important biomolecules for diagnosis of AIS in Chinese population.
HS is characterized by rupture of weakened blood vessel and contributes majority of death compared to ischemic stroke. We observed higher plasma levels of S100B, CRP, MMP-9, TNF-α, PAI-1, ICAM-1, and P-selectin in HS compared to healthy controls or stroke mimic cases suggesting possible biomarkers for diagnosis of HS. Further analysis by ROC curve area validates S100B (0.98), IL-6 (0.97), PAI-1 (0.99), MMP-9 (0.95), and TNF-α (1.0) as promising biomarkers of diagnosis of HS in Chinese. Although limited number of study were performed earlier to decipher probable biomarkers for diagnosis of HS, role of biomolecules such as S180B, 16 MMP-9, 15 and CRP 30 has been demonstrated in some population. Our present study has several advantages over earlier reports: we have tested wide range of biomolecules and in characterized sample categories. To the best of our knowledge, this study is first of its kind including AIS, HS, stroke mimic cases, patient controls, and healthy controls from Chinese population.
As the treatment strategies of stroke patients vary according to types of stroke, diagnosis of stroke type is very much essential for appropriate management and treatment of patients. Limited number of studies were performed earlier and identified possible biomolecules for differentiation of AIS and HS. Biomolecules such as S100B, 16 CRP, 30 and MMP-9 15 have been proposed to distinct hemorrhagic from ischemic stroke. Corroborating with previous reports,15,16,30 our analysis revealed S100B (0.88) and CRP (0.85) as promising biomarkers for differentiation of HS and AIS cases. However, area of ROC curve was not significant for MMP-9 (0.78) and ruled out possibility of marker for stroke categorization.
Contradictory findings have been reported on possibility of IL-10, LDL cholesterol, NO, and GFAP as biomarkers of stroke. Majority of studies in Italian population failed to establish IL-10 as a marker for stroke.21,22,31 High levels of LDL cholesterol has been shown in Taiwanese stroke patients; 19 in contrast, another independent report including Kuwait patients failed to demonstrate such link. 32 While Indian stroke patients displayed higher NO, 20 Venezuelans had lower in patients than controls. 33 Various meta-analyses revealed GFAP as a possible molecule to differentiate HS from ischemic stroke.34,35 However, we failed to observe such associations of IL-10, LDL cholesterol, NO, or GFAP in our studied Chinese cohort. These observations may be population specific and premature to conclude non-importance of IL-10, LDL cholesterol, NO, and GFAP as stroke biomarkers. Furthermore, studies with larger sample size are required in Chinese patients to validate our results.
In conclusion, our data suggest that biomarker panel including CRP, IL-6, PAI-1, P-selectin, and TNF-α may diagnose AIS, and other sets of biomolecules such as S100B, IL-6, PAI-1, MMP-9, and TNF-α may be useful for HS identification. Furthermore, quantification of markers like S100B and CRP can differentiate between ischemic stroke and HS in Chinese population. However, further studies including larger sample size are required for validation of our findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.