
Abstract
Objective
The effectiveness of the combination of steroids and antiviral agents in the treatment of Bell’s palsy remains unclear. This study evaluated the therapeutic effect of combination therapy in severe Bell’s palsy patients and assesses specific conditions under which combination therapy is more effective than steroids alone.
Methods
From January 2005 to December 2019, the records of 1710 Bell’s palsy patients who visited Kyung Hee University Hospital were reviewed retrospectively. Of these, 335 (19.6%) patients were diagnosed with severe Bell’s palsy, with 162 patients treated with steroids alone and 173 patients treated with combinations of steroids and antiviral agents. The outcomes of treatment were assessed using the House–Brackmann (H-B) grade according to age, sex, hypertension, diabetes, and obesity.
Results
The favorable recovery rate was significantly higher in severe Bell’s palsy patients who were treated with combinations of steroids and antiviral agents than with steroids alone (78.0% vs. 66.7%, p = 0.020). Subgroup analysis showed that combination therapy resulted in significantly higher recovery rates than steroids alone in patients aged ≥40 years (77.5% vs. 64.1%, p = 0.023) and in those without hypertension (75.8% vs. 63.3%, p = 0.044) and diabetes (79.7% vs. 65.5%, p = 0.007).
Conclusion
Combination therapy with steroids and antiviral agents resulted in significantly higher favorable recovery rates than steroids alone in severe Bell’s palsy patients. Combination therapy was particularly more effective than steroids alone in patients aged ≥40 years and in patients without hypertension and diabetes.
Introduction
Bell’s palsy is an unilateral peripheral facial nerve palsy of unknown cause that occurs with an annual incidence of 20–30 cases per 100,000 population.1,2 The exact mechanism of occurrence of Bell’s palsy is still unclear, but latent herpes virus reactivation is widely known as one of the causes of Bell’s palsy.3,4 Ischemia is caused by disruption of the microcirculation, followed by neural edema. Inflammation and edematous swelling of the facial nerve within the narrow fallopian canal causes nerve compression, which causes subsequent clinical symptoms.5,6 Based on these mechanisms, steroids, which effectively reduce swelling and inflammation of the facial nerve, have been used in the early stages of treatment of Bell’s palsy patients. The anti-inflammatory activities of steroids minimize nerve damage and improve outcomes.7–9
Despite evidence of viral infection in Bell’s palsy, the use of antiviral agents have shown relatively inconclusive and weak effects in several prospective studies, with the combination therapy with steroids and antiviral agents not achieving better outcomes than steroids alone.7,10,11 Other studies, however, found that combination treatment is more effective than steroids alone treatment, especially in severe Bell’s palsy patients, defined as an initial House–Brackmann (H-B) grade of five or 6.12–14 Recent Canadian Society of Otolaryngology and American Academy of Otolaryngology guidelines recommend treatment of Bell’s palsy with steroids alone, but suggest that combinations of steroids and antiviral agents may be effective in severe Bell’s palsy patients.15,16 Although most Bell’s palsy patients have a good prognosis, approximately 10 to 29% of patients develop persistent dysfunction of facial nerve and experience sequelae, including facial asymmetry, contracture, and synkinesis. In particular, severe palsy patients have a poorer prognosis than patients with milder forms, with up to half of the former failing to achieve favorable prognosis after 12 months despite steroid treatment. 17 Therefore, despite the unclear therapeutic effect of antiviral agents in Bell’s palsy, the combination of steroids and antiviral agents is being increasingly used to treat severe palsy patients. The present study compared the therapeutic effects of combinations of steroids plus antiviral agents with steroids alone in severe Bell’s palsy patients, and investigated the specific patient characteristics for which combination therapy is superior to steroids alone.
Methods
This retrospective cohort study evaluated facial palsy patients who were treated in the outpatient clinic of the Department of Otolaryngology at Kyung Hee University Hospital between January 2005 and December 2019. Three experts reviewed the medical records of these patients, each with more than 10 years of experience in Bell’s palsy. Bell’s palsy was diagnosed as an acute unilateral peripheral facial palsy with no obvious cause. Patients with facial palsy due to other causes, such as Ramsay–Hunt syndrome, facial palsy of central origin, traumatic facial palsy, neoplasms, otitis media, and history of otolaryngology surgery were excluded. Patients’ baseline characteristics, including age, sex, obesity, and comorbidities (hypertension and diabetes) were assessed before initiating medical treatment. Body mass index (BMI) of 25 kg/m2 or more was defined as obesity. 18
Bell’s palsy patients were administered oral steroids alone or in combination with antiviral agents starting within 7 days of facial paralysis. The steroid dosing schedule consisted of 12 days of oral prednisolone, 80 mg/day for the first 4 days and 60, 40, 20, and 10 mg/day every 2 days thereafter. Underweight adults started with 1 mg/kg/day, with the dose being gradually tapered as above. Antiviral therapy consisted of oral acyclovir, at a dose of 1000–2400 mg/day for 5 days, or oral famciclovir, at a dose of 750 mg/day for 7 days.
The severity of facial palsy was assessed using the H-B grading system, in which facial function is classified into six categories, going from grade 1(normal function) to grade 6 (complete paralysis). 19 Patients were classified as having mild (H-B grade 2), moderate (H-B grades 3 and 4), or severe (H-B grades 5 and 6) facial palsy, depending on the initial severity of facial palsy. Patients were followed up for a period of at least 6 months or until full recovery was achieved. A favorable recovery was defined as a final H-B grade of one or two, whereas an unfavorable recovery was defined as a final H-B grade ≥ 3.6,20
All patients underwent electroneuronography (ENoG) 5–14 days after the onset of paralysis. The nasalis muscle compound muscle action potential was determined, with the results expressed by dividing the maximum amplitude on the affected side by the maximum amplitude on the unaffected side (%). Amplitude <10% on the affected side was defined as a poor ENoG.14,20
Blood samples were obtained from patients within 5 days after the onset of paralysis. Complete blood counts, differential counts, and glycated hemoglobin concentrations were measured. The absolute neutrophil count divided by the absolute lymphocyte count was defined as the neutrophil to lymphocyte ratio (NLR).
This study protocol was approved by the Institutional Review Board of Kyung Hee University Hospital, which waived the requirement for informed consent due to the retrospective design of this study (IRB No 2017-11-058) (IRB No 2019-07-065).
All results are presented as means ± standard deviations, or as frequencies and percentages. Categorical variables were compared using the Fisher’s exact test and chi-square test, and continuous variables were analyzed using the Mann–Whitney U-test and independent t-test. Univariate analysis was performed to evaluate the factors associated with combination therapy resulting in superior recovery, compared with steroids alone, in severe Bell’s palsy patients. All statistical analyses were performed using IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA), with p-values less than 0.05 indicating statistical significance.
Results
During the study period, a total of 1710 patients were diagnosed with Bell’s palsy. Of these, 242 were excluded because they were aged < 16 years, had recurrent Bell’s palsy, had insufficient medical records (unclear time of onset or follow-up for <6 months after onset), had not received steroid treatment, had undergone surgical treatment for Bell’s palsy, or had uncontrolled hypertension or diabetes. Of the 1468 patients included, 753 (51.3%) were treated with steroids alone and 715 (48.7%) with steroids plus antiviral agents (Figure 1). At the onset of facial paralysis, 203 patients (13.8%) had mild palsy (H-B grade 2), 930 (63.4%) had moderate palsy (H-B grade 3–4), and 335 (22.8%) had severe palsy (H-B grade 5–6). These three groups differed significantly in their initial H-B grade (2.00 ± 0.00 vs 3.51 ± 0.50 vs 5.03 ± 0.16, p <0.001), final H-B grade (1.33 ± 0.47 vs 1.71 ± 0.69 vs., 2.07 ± 1.04, p <0.001), and ENoG score (65.4 ± 17.9 vs 58.3 ± 23.5 vs 39.5 ± 24.5, p <0.001). The severe palsy group had higher white blood cell counts, neutrophil percentage and NLR, and a lower lymphocyte percentage than the other two groups, but there were no significant intergroup differences in age, sex, BMI, comorbidities, and treatment methods (Table 1). Overview of patient enrollment. Mild palsy, initial H-B grade 2; moderate palsy, initial H-B grade 3,4; severe palsy, initial H-B grade 5,6. H-B grade, House–Brackmann grade. Demographic and clinical characteristics of patients with Bell’s palsy. BMI: body mass index; HTN: hypertension; DM: diabetes mellitus; H-B grade: House–Brackmann grade; ENoG: electroneuronography; WBC: white blood cell; NLR: neutrophil to lymphocyte ratio. Results are presented as mean ± standard deviation. *p<0.05. aMild palsy, initial H-B grade 2; moderate palsy, initial H-B grade 3,4; severe palsy, initial H-B grade 5,6.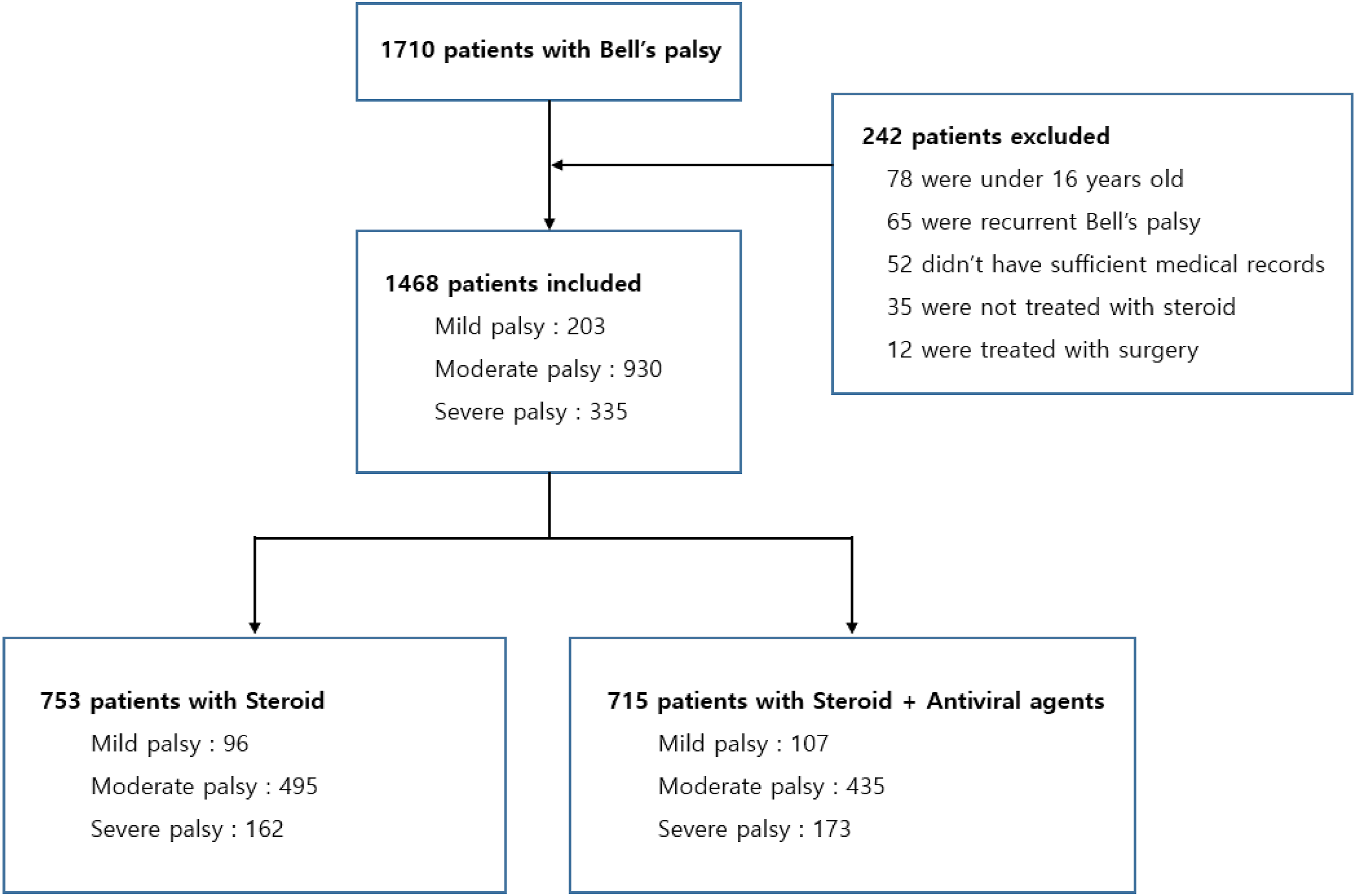

Characteristics and outcome measurements of patients with severe Bell’s palsy.
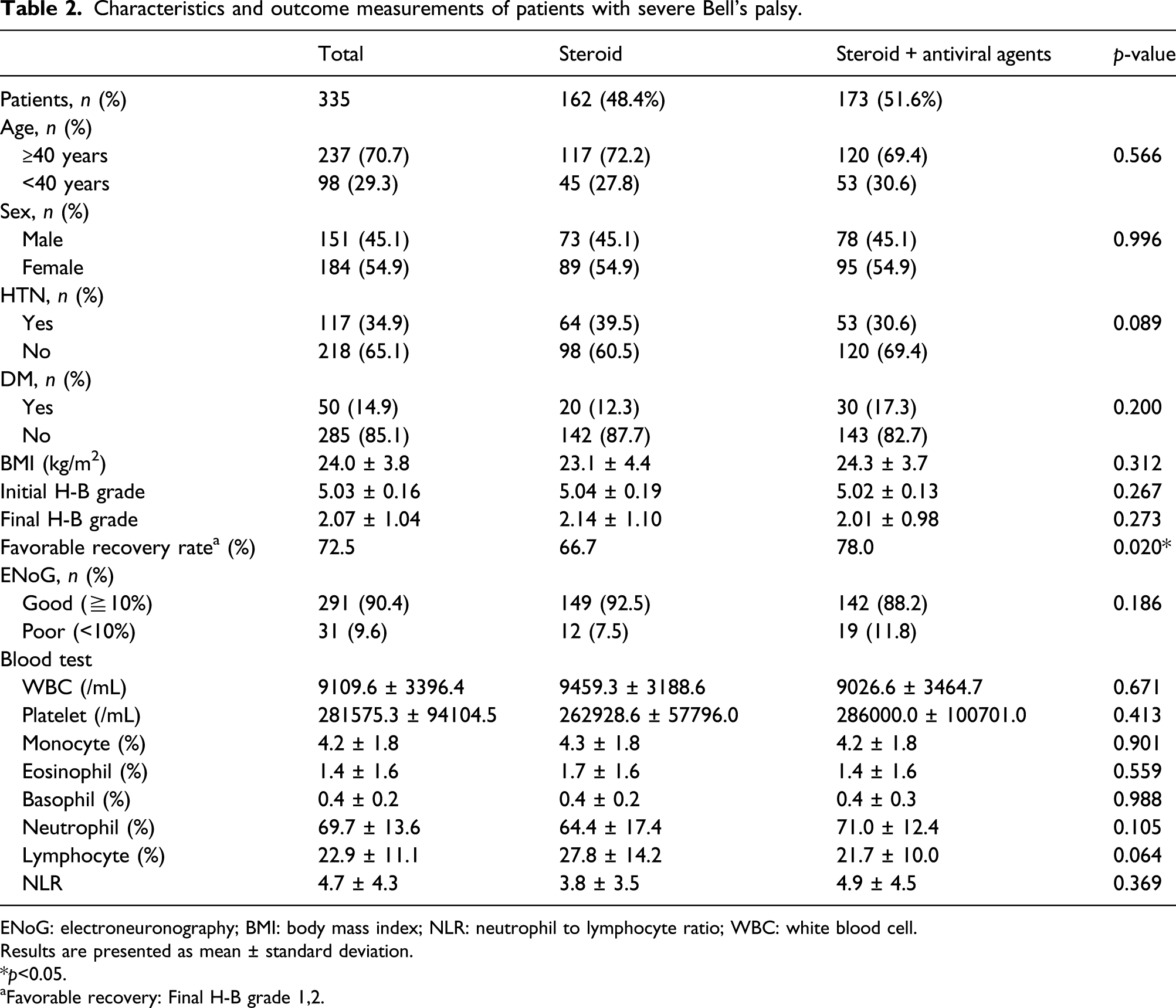
ENoG: electroneuronography; BMI: body mass index; NLR: neutrophil to lymphocyte ratio; WBC: white blood cell.
Results are presented as mean ± standard deviation.
*p<0.05.
aFavorable recovery: Final H-B grade 1,2.
Subgroup analysis to identify factors contributing to a more favorable recovery found that the rate of favorable recovery was significantly higher in patients aged ≥40 years who received combination therapy than in those who received steroids alone (77.5% [93/120] vs. 64.1% [75/117], p = 0.023). Although the favorable recovery rate was higher in patients aged <40 than ≥40 years, the recovery rate in younger patients did not differ significantly between those administered combination therapy and steroids alone. Although the favorable recovery rate in patients with hypertension did not differ significantly between both groups, the recovery rate in patients without hypertension was significantly higher in the combination therapy group than in the steroid alone group (75.8% [91/120] vs. 63.3% [62/98], p = 0.044). Similarly, the recovery rate in patients without diabetes was significantly higher in the combination therapy group than in the steroid alone group (79.7% [114 143] vs, 65.5% [93/142], p = 0.007). However, the favorable recovery rate did not differ significantly in patients with diabetes. Subgroup analysis did not find any significant difference in terms of recovery rates when studying sex and presence or absence of obesity (Figure 2). Therapeutic responses in patients with severe Bell’s palsy: Subgroup analysis. *p<0.05.
Adjusted odds ratios of favorable recovery among subgroups of patients with severe Bell’s palsy.

BMI: body mass index.
*p<0.05.
Discussion
Although Bell’s palsy is a disease with a relatively good prognosis, approximately 10–29% patients develop persistent dysfunction of facial nerve. To reduce the risk of persistent dysfunction and mental distress, it is important to identify and treat patients at high risk of poor long-term outcomes. Many studies have, therefore, evaluated the therapeutic effect of different treatment modalities in Bell’s palsy patients. The present study compared the therapeutic effects of combination treatment with steroids and antiviral agents with those of steroids alone in severe Bell’s palsy patients, as determined by initial H-B grade. In addition, we analyzed the patient factors associated with combination therapy having a better recovery rate than steroids alone.
Medical treatment of Bell’s palsy is based on the hypothesis that reactivation of latent herpes or other viruses within the geniculate ganglia causes neuropathy with cytotoxic edema and nerve inflammation. 3 Majeed et al. detected the human herpes virus 6 (HHV 6) in the saliva of patients with Bells’ palsy and controls, with HHV six levels being significantly higher in patients with Bell’s palsy (p = 0.028). They additionally found a positive correlation between House–Brackmann grade and viral load in patients with Bell’s palsy (p = 0.001). These results suggest that HHV six might play a role in the pathogenesis of Bell’s palsy. 21 Although early use of steroids has been shown to be effective in these patients, the therapeutic benefits of adding antiviral agents to steroids remain unclear. In several randomized placebo-controlled double-blind studies, no evidence was found of additional benefits of adding antiviral drugs.7,11 These studies, however, evaluated patients mild to severe paralysis, which may have masked improvements in particular subgroups of patients. When patients were classified by initial severity, combination therapy with steroids and antiviral agents was found to be more effective than steroids alone in treating severe Bell’s palsy patients.13,14,22 A recent Cochrane review reported that the combination therapy of antiviral agents and steroids may have little or no additional effect on incomplete recovery rates when compared with steroids alone in Bell’s palsy of various degrees of severity. 23 These results were imprecise, as the studies being evaluated utilized different antiviral agents, different grading systems, different definitions of good recovery, and included heterogeneous populations from multicenter studies and small sample sizes, limiting the ability to compare study results. According to a recent systematic review and network meta-analysis that studied the effectiveness of antiviral agents in treatment of Bell’s palsy, patients treated with famciclovir showed significantly better recovery of Bell’s palsy compared to those who received placebo. Also, acyclovir and valacyclovir showed a tendency toward better overall recovery. 24 The present study analyzed a large number of patients at a single center over a period >10 years and evaluated patients’ clinical characteristics and outcomes in relation to the initial severity of Bell’s palsy and treatment methods. To our knowledge, few studies to date have compared the therapeutic effectiveness of combination therapy with steroids alone in about 1400 Bell’s palsy patients treated at a single center.
Our evaluation of the demographic and clinical characteristics of 1468 Bell’s palsy patients found that 335 had severe paralysis (H-B grade 5,6); of these, 162 (48.4%) were treated with steroid alone and 173 (51.6%) with combination treatment. The overall favorable recovery rate was higher in the combination therapy group (78.0%) than in the steroid alone group (66.7%), consistent with the results of our previous prospective, randomized study. 14 In all previous randomized controlled trials reporting that combination treatment had no additional benefit compared with steroids alone, “complete recovery” was defined as a final H-B grade 1 or a Yanagihara score > 36.7,10,11 In other studies, however, “favorable recovery” was defined as a final H-B grade ≤2, based on normal function in daily life.14,20,22 In the present study, “favorable recovery” was defined as a final H-B grade of one or two, and its rate was higher in patients who received combination therapy than steroid alone. Therefore, these findings provide a rationale for the use of additional antiviral agents in the treatment of severe Bell’s palsy.
Several factors have been reported to affect the prognosis of patients with Bell’s palsy, including age, sex, hypertension, diabetes, obesity, electrophysiological test results, and treatment methods. Electrophysiological tests such as ENoG are valuable for assessing the risk of poor outcome in Bell’s palsy patients, predicting poor outcomes in patients with >90% degeneration on the affected side within 14 days of symptom onset. 25 Because ENoG can determine the degree of Wallerian degeneration about 7–10 days after symptom onset,25,26 these ENoG results are ineffective in predicting prognosis in patients started on treatment soon after symptom onset.
Subgroup analyses were also performed in this study to investigate specific factors prognostic of higher favorable recovery rates in patients with severe Bell’s palsy who received combination therapy. Patients were dichotomized by age (<40 vs. ≥40 years), sex, the presence or absence of hypertension, diabetes, and obesity. Several studies have reported that older age was significantly associated with reduced final recovery rates,27–29 whereas other studies have found no association between age and treatment outcomes.17,30 In the present study, favorable recovery rates in patients of all age groups were higher in those who received combination therapy than steroid alone, with the difference being statistically significant in patients aged ≥40 years. These findings suggested that combination therapy may aid recovery in severe Bell’s palsy patients aged ≥40 years. This may be due to the association between age and the prevalence of latent herpes simplex virus, which was found to increase from 18.2% in subjects aged 0–20 years to 100% in persons aged >60 years. 31 Because increasing age increases the prevalence of latent herpes simplex infection, antiviral agents may have more pronounced additional effects in older than in younger patients with severe palsy.
With regard to sex and obesity, previous studies have reported that sex is not related to the prognosis of patients with Bell’s palsy,30,32 but that obese patients show lower recovery rates than normal weight patients.33,34 Although the present study assessed the therapeutic effect of additional antiviral agents in patients classified by sex and obesity, there were no significant differences in recovery rates between combination therapy and steroid alone in all groups.
Hypertension and diabetes have been reported to be associated with the prognosis of patients with Bell’s palsy. Hypertension has been found to contribute to better outcomes,29,34 whereas diabetes has been found to contribute to poorer outcomes.30,34,35 Other studies, however, have found that hypertension and diabetes are unrelated to patient prognosis. 32 Although previous studies assessed the relationships between underlying diseases and prognosis, this study investigated the therapeutic effects of different treatment methods in subjects with and without hypertension or diabetes. Although combination therapy showed improved recovery rates in both patients with and without hypertension, this difference was statistically significant only in patients without hypertension. Therapeutic responses were similar in diabetes patients who were administered combination therapy and steroid alone, but a higher recovery rate was observed in patients without diabetes who received combination therapy than steroid alone. Logistic regression analysis showed that combination therapy increased the odds ratio of favorable recovery in severe Bell’s palsy patients without diabetes and without hypertension, suggesting that additional antiviral agents were more effective than steroid alone in severe Bell’s palsy patients without hypertension or diabetes. This finding is in agreement with the results of our previous study, although that study analyzed patients with all degrees of severity. 20 Diabetes and hypertension are underlying diseases that may affect the microcirculation, such as the vasa nervosum, causing microangiopathy. Microcirculatory failure of the vasa nervosum in severe Bell’s palsy patients with diabetes or hypertension may undermine the therapeutic effects of antiviral agents. 36
This study has several limitations. First, this study had a retrospective design. Second, we did not perform a genomic study (PCR) for herpes viruses. If these viruses had been detected through a genomic study and the effect of the antiviral agents analyzed, a clearer conclusion could have been drawn about the effect of the antiviral agents. Third, we did not compare the therapeutic effects of different antiviral agents (acyclovir, famciclovir, and valacyclovir). Fourth, the statistical analysis used in this study may have limitations. In particular, we did not perform calculations to justify the sample size selected.
In conclusion, the combination of steroids and antiviral agents resulted in significantly higher favorable recovery rates than steroids alone in severe Bell’s palsy patients. Combination therapy was particularly more effective than steroids alone in patients aged ≥40 years, and in patients without diabetes and hypertension, suggesting that combination therapy be considered in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (NRF-2018R1A6A1A03025124) (NRF-2019R1F1A1049878).
Ethics approval
Ethical approval for this study was obtained from *Kyung Hee University Hospital INSTITUTIONAL REVIEW BOARD (IRB No 2017-11-058/ 2019-07-065.
Informed consent
Informed consent was not sought for the present study because *retrospective design of this study *