
Abstract
Background
Persistent systemic inflammation leads to multidistrectual body dysfunctions. Attenuation of inflammation may improve patients’ functional and life prognoses. We hypothesized that essential amino acids (EAAs) given to elderly patients in rehabilitation after acute diseases may be associated with a reduced inflammatory state. Therefore, this retrospective study investigated whether the supplementation of EAAs – modulators of immune competence – was associated with a reduced inflammation rate in elderly patients.
Methods
The medical records of 282 patients admitted to the rehabilitation (rehab) institute after acute index events (surgery or medical diseases) (age: 81.18 ± 8.58 years; females: 67.9%) were analyzed.
Results
46 patients (16.3% of the entire population) had received EAA supplements (S), whereas the remaining 236 patients had not (N-S). Systemic inflammation (I) (serum C-reactive protein (CRP) > 0.5 mg/dL) was present in 67.4% of the I-S group and 57.2% of the I-N-S group. During rehab, the I-S group (but not the I-N-S group) showed a reduction in CRP levels (p = 0.03) and an increase in circulating lymphocytes (p = 0.035), immune cells of the adaptive immune system. C-reactive protein levels remained virtually unchanged in non-inflamed patients who received supplements but increased in non-inflamed patients who did not receive supplements (p = 0.05). Stratified for developed infections, CRP levels reduced in S patients (p = 0.008) but did not in N-S patients.
Conclusion
EAA supplementation was associated with reduced inflammation in both inflamed and infected patients. In addition, EAA supplementation was associated with increased circulating lymphocytes in inflamed patients.
Keywords
Introduction
Although inflammation is protective in nature as it limits pathogen invasion, when it becomes persistent (chronic inflammation), it results in multidistrectual dysfunctions of tissues and organs.
Low levels of chronic inflammation (inflammaging) 1 characterize important chronic age-associated diseases such as diabetes mellitus, cardiovascular disease and asthma.2–4 Chronic inflammation is also associated with chronic heart failure, 5 chronic kidney disease 6 and chronic obstructive pulmonary disease. 7
The detrimental effects of inflammation have also been documented in rehabilitation (rehab) settings. High serum C-reactive protein (CRP), the marker of systemic inflammation, limits the recovery of sub-acute patients after stroke8–10 and post-surgery hip fracture.11,12 Moreover, high CRP levels predict the development of infection 13 and negative rehab outcomes in sub-acute elderly patients. 14 A recent study has reported that postoperative morbidity is independently associated with inflammation but not with hyperglycemia or markers of insulin resistance. 15
Inflammation is especially problematic in elderly patients as it can be magnified by age-related deteriorations of immune cells (immunosenescence). 16 In turn, immunosenescence greatly contributes to the degree and persistence of systemic inflammation. 17
The reduction of inflammation likely decreases the progression of any disease towards chronic conditions and the incidence/severity of infection. It also improves patient clinical rehabilitative outcomes.
In the present study, we formulated two hypotheses. Firstly, the reduction of persistent inflammation may be achieved by boosting the adaptive immune system given that high levels of inflammation impair the adaptive immune response to antigen stimulation. 18 Secondly, essential amino acids (EAAs) may be able to balance innate–acquired immunity by reducing inflammation and increasing the acquired arm of the immune system.19–21 The rationale behind our second hypothesis was based on the following factors. Under physiological conditions, amino acids (AAs) – primarily EAAs – are essential for the proliferation and differentiation of innate and acquired immune cells.22,23 In particular, EAAs allow lymphocyte protein syntheses to ensure their proliferation and maturation as well as cytokine and antibody production.22,23 Moreover, clinical studies have documented that EAA supplementation has been shown to reduce the rate of inflammation and nosocomial infections in elderly post-acute patients, 13 in patients with severe brain injury, 24 in dysphagic stroke patients 25 and in elderly subjects after surgery following hip fracture. 26
Therefore, the aim of this retrospective study was to document whether supplemented EAAs were associated with a reduced inflammation (CRP) rate in elderly patients admitted to our rehab institute after acute events for any medical or surgical disease. Our ultimate goal was to encourage future investigations into the effects of AA intake/supplementation, in particular EAAs, on disease-induced inflammation and altered immunity. We think effective nutritional interventions that target inflammation could enhance anti-inflammatory drug therapy.
Materials and methods
Population
The medical records of 318 elderly patients consecutively admitted to the geriatric rehab institute (GRI) between 1 January 2017 and 31 December 2019 were examined. The patients had been admitted to the GRI 20 ± 7 days after acute medical events (or reacutization of a chronic disease) or surgical intervention following skeletal trauma. We chose not to adopt exclusion criteria for the purposes of our study as our aim was to describe a possible association of supplemented EAAs with a more balanced immune response. However, we excluded 36/318 patients (11.3%) who were subsequently transferred to the emergency department or to an acute hospital setting or who died. Therefore, the medical records of 282 patients were analyzed.
The protocol was approved by the local ethical–technical committee of the GRI (Atti/2018/SM/R002/218 February). All patients gave their written informed consent to the research on admission to the GRI, following the standard protocol.
Patients’ characteristics and variables
Patients’ characteristics and variables (N = 282 patients) registered at time of their admission to the GRI.

Data are reported as mean ± SD for continuous variables and N (%) for categorical variables.
*100 = maximal functional performance.
GRI: geriatric rehab institute; nv: normal values.
Immune variables had been repeated a few days before patients were discharged from the GRI.
Co-morbidities
Disease(s) associated with the primary disease, analyzed using the Charlson Index, 28 was/were also considered.
For more clarity, with the exception of immune activity variables and serum albumin levels, all the other variables were utilized for the sole purpose of describing the clinical presentation of the patients at the time of their admission to the GRI.
Patients stratified for EAA supplementation
Some of the metabolic effects that the EAAs in the study formula exert on the cell immune system.

EAA: essential amino acids; BCAAs: branched chain amino acids (leucine, isoleucine and valine).
The medical records reported that EAA supplementation had been prescribed to increase patients’ inadequate protein intake (<0.8 g protein/kg/day), according to a consolidated protocol adopted in the GRI.
Patients had received EAAs before, after or during the development of an infection.
Objectives of the study
1. The primary objective of the study was to document whether supplemented EAAs were associated with a reduced inflammation (CRP) rate. 2. The secondary objective was to document a possible improvement of peripheral lymphocyte count in patients supplemented with EAAs.
Sample size calculation
We computed the minimum sample size required to detect a medium effect size (Cohens’ d = 0.5) difference in the change (values at T1 − values at T0) of serum CRP between EAA-supplemented and non–EAA-supplemented patients with a power equal to 80%, a two-tailed Type I error equal to 0.05. We anticipated that there would be much fewer supplemented patients than non-supplemented patients (around 1/5). Accordingly, the computed sample size was equal to 228 patients (38 EAA-supplemented and 190 non–EAA-supplemented).
Statistical analysis
The Shapiro–Wilk statistic supported by visual inspection was used to test the normality of the distribution of all variables. Several variables violated the normality assumption. Accordingly, descriptive statistics were reported as mean ±standard deviation (SD), but hypothesis testing was based on non-parametric statistics. Within-group comparisons were carried out by the Wilcoxon signed rank test and between-group comparisons were carried out by the Mann–Whitney U test.
Comparisons of categorical variables were carried out by the chi-square test. The association between couples of variables was assessed by the Spearman correlation coefficient. Multivariable regression analysis was carried out to assess the relationship between changes in serum CRP (values at T1 − values at T0) and EAA supplementation, adjusting for confounding factors such as age, sex and serum albumin levels. All statistical tests were two-tailed and statistical significance was set at p < 0.05. All analyses were carried out using the SAS/STAT statistical package, release 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
When the patients were considered as a whole group, they presented with systemic inflammation, normal weight, mild anaemia and hypoalbuminemia, light cognitive dysfunction, and an important reduction in physical function during their daily life activities.
On admission to rehab (T0), 46 patients (16.3% of the entire population, n = 282) had been supplemented with EAAs (S) and 236 patients had not been supplemented (N-S).
A state of systemic inflammation (I: serum CRP > 0.5 mg/dL) was present in 166 patients (58.9% of the entire population): 31 in S (I-S: 67.4% of S) and 135 in N-S (I-N-S: 57.2% of N-S). I-S, compared to I-N-S, were older (85.5 ± 7.7 years vs 81.0 ± 8.4 years, p = 0.001), had a lower BMI (21.2 ± 2.5 kg/m2 vs 25.0 ± 2.1 kg/m2, p = 0.0006), had a larger reduction of serum albumin levels (p = 0.037) and had a higher rate of inflammation (p = 0.019) (Supplementary Material Table 1). Among non-inflamed patients (n = 116; CRP < 0.5 mg/dL), S patients (n = 15) had a lower CRP than N-S patients (n = 101) (p = 0.05) (Supplementary Material Table 2).
During the rehab stay, CRP was reduced in I-S but not in I-N-S (p = 0.030), and peripheral blood lymphocytes increased more in I-S than in I-N-S (p = 0.035) (Supplementary Material Table 1). Among non-inflamed patients, baseline CRP was virtually unchanged in S patients, but increased in N-S patients (p = 0.052) (Supplementary Material Table 2). During rehab, changes in total white blood cells, neutrophils, neutrophil–lymphocyte ratio between I-S and I-N-S and between non-inflamed S patients and non-inflamed N-S patients were similar.
Infection episodes (INF) occurred in 21/46 (45.6%) of S patients (INF-S) and 132/236 (55.9%) of N-S patients (INF-N-S) (not significant). As regards the level of inflammation, serum CRP diminished in INF-S but not in INF-N-S (p = 0.008) (Supplementary Material Table 3). In patients who had not developed infections (NO-INF), CRP diminished in S patients (NO-INF-S) and remained unchanged in N-S patients (NO-INF-N-S) (p = 0.046) (Supplementary Material Table 4). No significant differences were found regarding the lymphocyte variations between INF-S and INF-N-S and between NO-INF-S and NO-INF-N-S.
At discharge from rehab (T1) the neutrophil–lymphocyte ratio was higher in I-N-S patients than in I-S. Both I-S and I-N-S had been discharged with a CRP above the range of normal values (Supplementary Material Table 1). Among non-inflamed patients, the S patients had a lower CRP than the N-S patients (Supplementary Material Table 2).
Figures 1 and 2 report the effects of EAA supplementation on the considered variables: EAA supplementation was associated with reduced inflammation in all the patient categories and with improved circulating lymphocytes in the inflamed category only. Moreover, supplemented EAAs improved serum albumin levels. Values at admission (T0) and at discharge (T1) from rehab in supplemented (square) and non-supplemented (diamond) patients. Left panels are for inflamed and right panels for non-inflamed patients. ^: p < 0.05, †: p < 0.01, ‡: p < 0.001 for the comparison T1 versus T0. CRP: serum C reactive protein; TWBC: total white blood cells. Values at admission (T0) and at discharge (T1) from rehab in supplemented (square) and non-supplemented (diamond) patients. Left panels are for infected and right panels for non-infected patients. ^: p < 0.05, †: p < 0.01, ‡: p < 0.001 for the comparison T1 versus T0. CRP: serum C reactive protein; TWBC: total white blood cells.

Correlations between changes in serum CRP and covariates
Multivariable regression analysis, carried out on the whole population, revealed that the changes in serum CRP (values at T1 − values at T0) were significantly associated with EAA supplementation (p = 0.029) and that this association was independent of age, sex or serum albumin levels. None of these adjusting factors was significantly associated with changes in CRP (p = 0.06, p = 0.61 and p = 0.73 for sex, age and albumin, respectively).
Correlations between serum CRP and immune cells
Association (Spearman r) between CRP and total white blood cells (TWBC), neutrophils and lymphocytes, stratified according to AA supplementation at T0 (a) (admission to rehab) and T1 (b) (discharge from rehab).

^: p < 0.05; †: p < 0.01; ‡: p < 0.001.
AA: amino acid; CRP: C-reactive protein; N-S: non-supplemented patients; rehab: rehabilitation; S: supplemented patients; TWBC: total white blood cells.
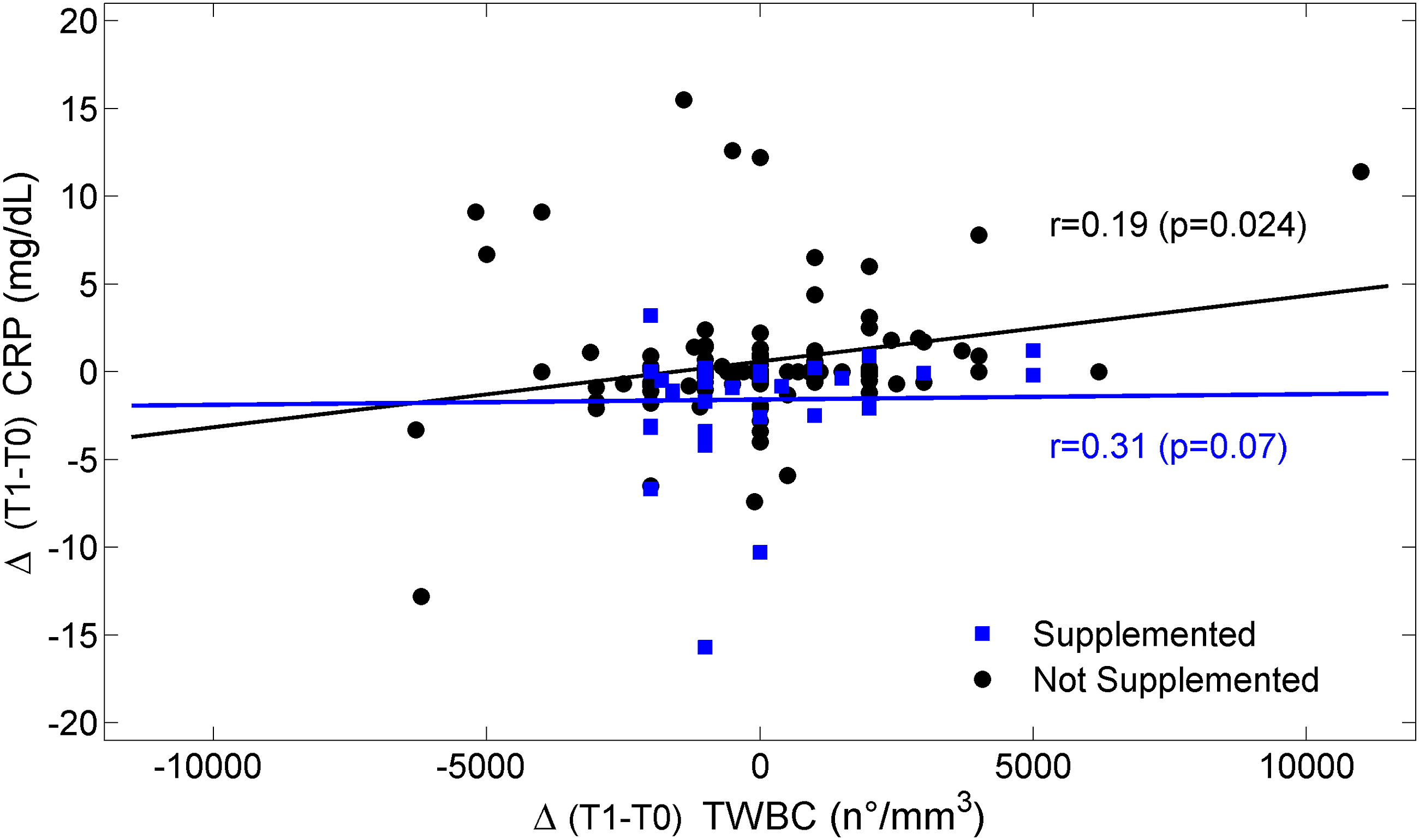
C-reactive protein was positively and significantly linked to total white blood cells and neutrophils in each patient group, both on admission and discharge, with the exception of the absence of a CRP correlation with neutrophils on discharge in S. On the contrary, CRP was not significantly linked to peripheral lymphocyte count in the time points considered. Figure 3 shows that negative correlations occurred between the time courses of lymphocytes and the time courses of CRP in both S and N-S groups. Moreover, the overtime change in total white blood cells significantly correlated with serum CRP in N-S but not in S patients (Figure 4). Furthermore, the study found that the time course of circulating neutrophils was positively linked to the time course of CRP both in S and N-S patients, even though the association was stronger in the latter group (Figure 5). Scatterplot of the relationship between delta (differences T1-T0) C-reactive protein and delta lymphocytes. Squares are for supplemented patients and dots are for non-supplemented patients. The Spearman correlation coefficient r is reported for both groups. Scatterplot of the relationship between delta (differences T1-T0) CRP and delta TWBC. Squares are for supplemented patients and dots are for non-supplemented patients. The Spearman correlation coefficient r is reported for both groups. CRP: C-reactive protein; TWBC: total white blood cells. Scatterplot of the relationship between delta (differences T1-T0) C-reactive protein and delta neutrophils. Squares are for supplemented patients and dots are for non-supplemented patients. The Spearman correlation coefficient r is reported for both groups.

Discussion
This study shows that more than half of the patients had systemic inflammation and that the use of EAAs was shown to be associated with reduced inflammation in I and INF patients. In I patients, EAAs were also associated with improved peripheral adaptive immune response and consequently with a better balance of the immune system from innate to adaptive immune function. Given that in patients with inflammation the association regarded both the innate and adaptive immune cells, the discussion will focus on this patient category.
Essential amino acid–associated reduced inflammation (as also shown in Figure 1) is in line with the results from previous research studies carried out in elderly patients in a rehab programme.12,25 Supplemented EAAs attenuated the interrelationships between inflammatory markers and enhanced the negative effects of adaptive immune response on the inflammatory process (Figure 3).
We are aware that correlation does not necessarily imply causation, yet, based on the above studies and on the knowledge of the physiological importance that AAs have for immune system functions, 22 we postulate that EAA utilization and improved immune balance is more than a simple association, as previous studies have highlighted.13,24,25 To further support this hypothesis, the association occurred in patients with more frailty conditions, that is, with older age, higher rate of inflammation and with more deteriorated metabolic (hypoalbuminemia) and nutritional (body weight loss) conditions.
The link between EAAs and balanced immune response also occurred in the patients who had developed infectious complications.
The findings of this study raise the question of whether mild inflammation and its reduction may be clinically important. The authors of the present article believe that this is the case for the following reasons. Firstly, concentrations of CRP > 1 mg/dL are considered clinically significant. 27 Secondly, mild inflammation (CRP concentrations > 1 mg/dL) is found in subjects with type 2 diabetes,29–31 insulin resistance 32 and obesity. Moreover, CRP is not only a marker of inflammation but is itself a pro-inflammatory molecule able to induce insulin resistance. 33 Thirdly, mild inflammation is a negative predictor of both neurocognitive recovery of stroke patients 10 and physical autonomy in post-acute rehab elderly patients.12,14,25 Fourthly, increased CRP levels hide increased interleukine-6 (IL-6) production and activity. IL-6 has pleiotropic actions including the stimulation of muscle protein catabolism, 34 impaired aerobic energy formation 35 and increased activation of catabolic hormones such as cortisol and glucagon. 36 In addition, IL-6 has a cardiodepressant activity. 37
Potential mechanisms underlying the association of EAA supplementation with improved immune response
Given that AAs are essential for the innate and adaptive immune cells,22,38 the use of EAAs likely favoured the patient balance of immune response by influencing both innate and adaptive immune cells. The three BCAAs probably played a key role as they make up 30–45% of the EAAs in the diet of the patients in our GRI and 68.1% of the EAAs contained in the study formula. In addition, BCAA leucine is the most potent stimulator of mTOR signalling for body protein synthesis of body districts including the immune system, in particular lymphocytes.22,39 Furthermore, the BCAAs valine and isoleucine can be used in the tricarboxylic acid cycle for aerobic energy production, which is also essential for lymphocyte function. 39
The similarities in total white blood cells, neutrophils and neutrophil–lymphocyte ratios between I-S and I-N-S, along with a significant positive link between the total white blood cell count, the neutrophil count and serum CRP concentrations led us to suspect that the number/functions of innate immune cells other than neutrophils were influenced by EAAs and that the influence of EAAs was exerted on the activity rather than on the number of immune cells. This is supported by a trial 40 performed in elderly malnourished patients treated with the same EAA formula in the same amount (8 g/d). The study documented improved mitochondrial activity and function in peripheral blood mononuclear cells (PBMCs).40,41
Increased energy availability in the innate immune cells of PBMCs may have boosted both the phagocytosis activity and the capacity for the clearance of debris, with consequent reduction in local pro-inflammatory stimuli. Moreover, adequate energy is essential for protein synthesis and the cells of the immune system are strongly dependent on protein synthesis 38 for producing cytotoxic proteins (by T lymphocytes), antibodies (by B lymphocytes), cytokines, glutathione, nitric oxide and other molecules of enormous biological importance. 38
Likely, the link between EAAs and the immune response was also mediated by EAA-stimulated insulin-like growth factor-1 (IGF-1) production.42–44 Branched-chain amino acids increased the amount, maturation and functions of dendritic cells enhancing their capacity of stimulating both innate and adaptive reactions.45,46
Similarly to the innate immune cells, EAA supplementation influenced the proliferation of the adaptive immune cells (lymphocytes) in the I patients. The influence of EAAs may have also been exerted on lymphocyte metabolic activities. This is suggested by the negative relationship between the time courses of lymphocytes and CRP plasma levels. Indeed, this correlation was not found when the two functions were expressed in absolute values but only when expressed in terms of time courses, both in the entire patient population and mainly in subgroup I. This suggests that the improvement in peripheral lymphocyte activity and reduced inflammation are closely linked. 47 The present study suggests that during EAA supplementation, the lymphocytes conditioned the rate of inflammation. On the other hand, EAAs can stimulate the lymphocytes both directly and indirectly. Directly, EAAs stimulate the lymphocyte mTOR pathway for protein synthesis, which is necessary for the differentiation, activation and function of T and B lymphocytes, as well as of the antigen-presenting cells. 48 Among the essential BCAAs, leucine is particularly active in stimulating the mTOR pathway. Several clinical studies have reported that BCAA supplementation benefited the immune response in cirrhotic patients 45 and in post-surgery allergic subjects. 49 Moreover, EAA supplementation improved immune capacity and reduced nosocomial infection occurrence by 30% in post-acute elderly patients 13 and by 23% in patients with severe traumatic brain injury. 10 On the other hand, it is well known that EAAs/BCAAs can stimulate immune cells, in particular T and B lymphocytes.22,38
Essential amino acids indirectly influence lymphocytes, and in general the immune system, via formation of the amino acid glutamine (Gln), stimulation of IGF-1 production and reduction of cortisol levels following reduced inflammation.
Gln, produced by leucine metabolism within the skeletal muscle, among its numerous pro-immunogenic activities, promotes T cell proliferation, protects T cells against apoptosis, suppresses the cytokine expression of Th1 and Th17 cells, and modulates the homoeostasis between Treg and Th cells. 50
With regard to IGF-1, nearly all immune cells express the receptors for this hormone. 43 IGF-1 regulates T and B lymphocyte functions. 43
Reduced cortisol production following reduced inflammation increases circulating lymphocytes. Lymphocytes, more than granulocytes and monocytes, express cortisol receptors, the stimulation of which is associated with lymphopenia. 51
Anti-inflammatory nutrition as a potentially effective addition to anti-inflammatory drugs. A field for future research
Although anti-inflammatory drugs are the cornerstone therapy for diseases associated with high inflammatory rates, the adoption of a nutritional strategy that is capable of attenuating inflammation might be an effective addition to anti-inflammatory drugs. Indeed, an anti-inflammatory diet, 52 the way in which food is consumed and EAA supplementation might be useful. However, the effect of the association of anti-inflammatory drugs and anti-inflammatory nutrition on the rate of reduction of inflammation should be tested in future research. If this association were found to reduce inflammation, it may have practical implications for the most effective treatment of elderly patients on chronic anti-inflammatory drugs. Indeed, it cannot be excluded that nutritional intervention may lead to the reduction of drugs and their side effects on the central nervous, cardiovascular, gastrointestinal and respiratory systems as well as on circulating blood cells, kidney function and skin integrity.
Limitations of the study
The study has several limitations, including the lack of patients’ nutritional intakes, body composition and evaluation of T lymphocyte subpopulations.22,38
Suggestions for clinical practice
Although the present article is retrospective in nature, we think that it provides some useful information for clinical practice: 1. When possible, analyses of body composition, muscle strength and dietary nutrient intakes should be monitored over time – all these aspects should be considered important for immune capacity, besides their nutritional value. 2. It is useful ‘to read’ the distributions of peripheral white blood cells not only for their numeric value but also for the immune processes their changes highlight. In addition to infection, this may be valuable in any other disease. 3. Given the detrimental effects derived from chronic inflammation, it would be useful to recommend an ‘anti-inflammatory diet’ to inflamed patients.
53
Future research studies
The results of this retrospective study should encourage clinical trials aimed to document the efficacy of oral AA supplementation to reduce post-acute and chronic inflammation, improve the immune response and modulate the immune metabolism.13,24
Considering the results of the present study, it may be useful to carry out future research into the level of CRP at which the molecule exerts an anti-inflammatory function rather than a pro-inflammatory activity in sub-acute/chronic patients. 21
Conclusions
This retrospective study found that supplementation of EAAs to sub-acute elderly patients was associated with reduced serum CRP levels under inflammatory and infectious conditions. In inflamed patients, EAA supplementation was also associated with improved circulating lymphocytes.
Supplemental Material
sj-pdf-1-iji-10.1177_20587384211036823 – Supplemental Material for Essential amino acid supplementation is associated with reduced serum C-reactive protein levels and improved circulating lymphocytes in post-acute inflamed elderly patients
Supplemental Material, sj-pdf-1-iji-10.1177_20587384211036823 for Essential amino acid supplementation is associated with reduced serum C-reactive protein levels and improved circulating lymphocytes in post-acute inflamed elderly patients by Roberto Aquilani, Ginetto C Zuccarelli, Roberto Maestri, Mirella Boselli, Maurizia Dossena, Eleonora Baldissarro, Federica Boschi, Daniela Buonocore and Manuela Verri in International Journal of Immunopathology and Pharmacology
Footnotes
Acknowledgements
This research was supported by the Italian Ministry of Education, University and Research (MIUR), Dipartimenti di Eccellenza Program (2018–2022)-Dept. of Biology and Biotechnology “L. Spallanzani”, University of Pavia (to R.A., M.D., D.B., M.V.).
Author contributions
R. Aquilani contributed to the conception and design of the research; R. Maestri, M. Dossena, F. Boschi and D. Buonocore contributed to the acquisition and analysis of the data; R. Aquilani, G. C. Zuccarelli, M. Boselli and E. Baldissarro contributed to the interpretation of the data; R. Aquilani and M. Verri drafted the manuscript. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author Roberto Aquilani is a scientific consultant at Professional Dietetics (Milano, Italy). This company had no role in the design, execution, interpretation or writing of the study. The other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the local Ethical-Technical Committee of the Geriatric Institute P. Redaelli – Vimodrone, Milano, Italy (Atti/2018/SM/R002/218 February).
Informed consent
All patients gave their written informed consent to the research on admission to the Geriatric Rehabilitation Institute, following the standard protocol. Written informed consent was obtained from all subjects before the study.
Supplementray material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.