
Abstract
Cholecystitis is a common disease, but the occurrence of gallbladder strangulation is extremely rare. Here, we report a case of an 88-year-old woman with strangulated cholecystitis caused by an intraperitoneal band. Computed tomography (CT) scan revealed a constriction of the gallbladder body and marked wall thickening at the fundus. Additionally, the finding suggested torsion at the constricted area, which we diagnosed as gallbladder torsion. Cholecystectomy was performed immediately, and the diagnosis was strangulated cholecystitis caused by a band. The imaging findings of strangulated cholecystitis are similar to gallbladder torsion, making it difficult to diagnose preoperatively. We will discuss the imaging findings of strangulated cholecystitis and gallbladder torsion.
Introduction
Cholecystitis is generally caused by the impaction of gallstones in the cystic duct. In rare cases, the cystic duct may twist as a consequence of a floating gallbladder, resulting in ischemic inflammation, called gallbladder torsion. Floating gallbladders are classified as type I when the gallbladder and cystic duct are connected to the underside of the liver by the mesentery, and type II when only the cystic duct is connected by the mesentery, and in both cases the gallbladder is not sufficiently fixed to the liver bed. 1 Subsequently, the gallbladder may twist in the cystic duct due to acquired factors (kyphosis, scoliosis, emaciation, postural changes, intestinal peristalsis, trauma, etc.), resulting in gallbladder torsion.
Strangulated cholecystitis is an extremely rare disease caused by blood flow disturbance due to gallbladder strangulation by an intraperitoneal band. It can occur regardless of whether the gallbladder is floating or not, and strangulation causes were a tip of the lesser omentum, a tip of the omentum, a congenital omental band, and a perihepatitis band.2–6
Here, we report a very rare case of strangulated cholecystitis that presented imaging findings similar to those of gallbladder torsion and discuss the imaging findings.
Case report
An 88-year-old woman was diagnosed with cholecystitis at another hospital and was transferred to our hospital. On arrival, she had tenderness in the right hypochondrium, and blood test results showed a mildly increased inflammatory response. She had a history of appendectomy and a medical history of Lemmel syndrome and cholangitis due to endoscopic retrograde cholangiopancreatography.
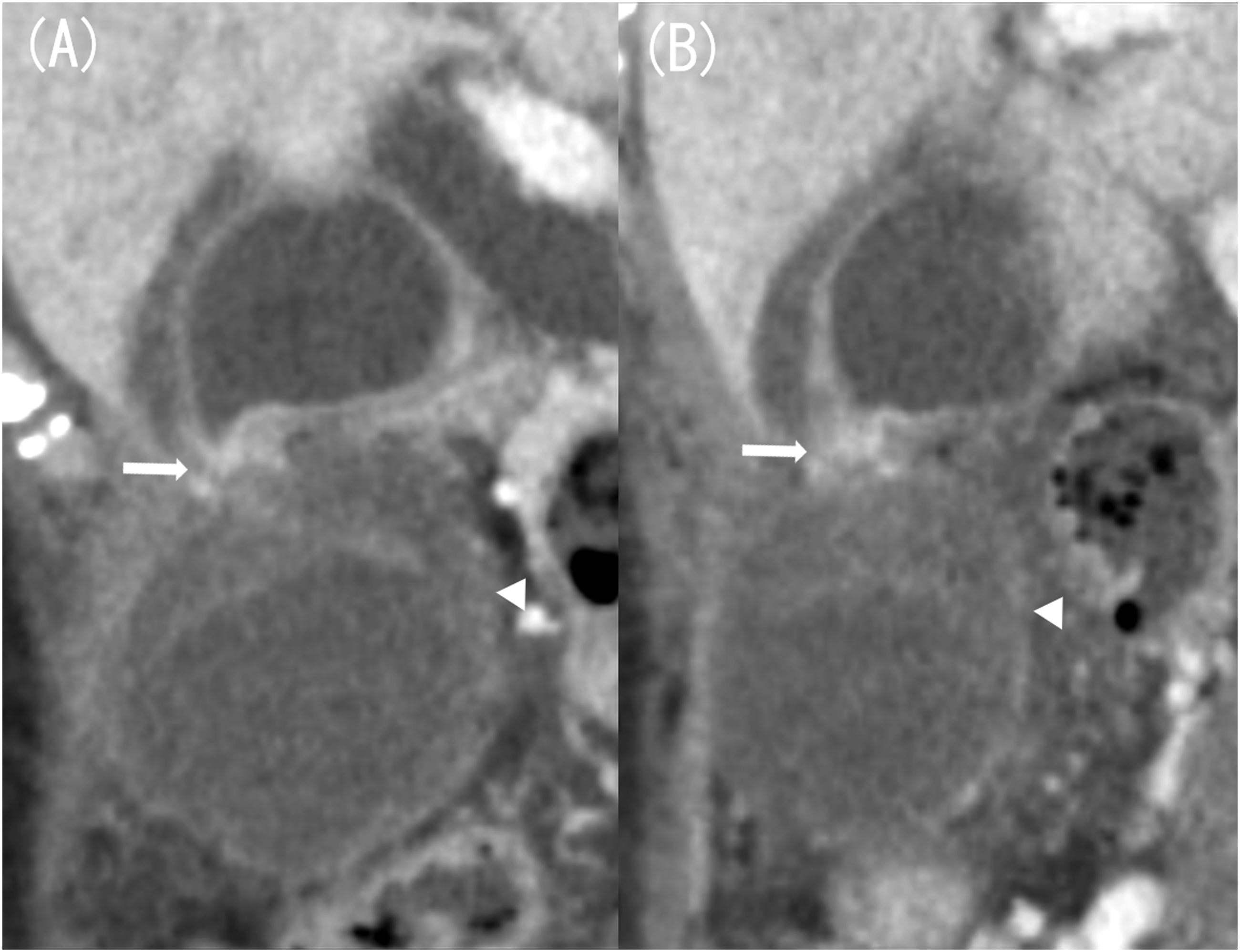
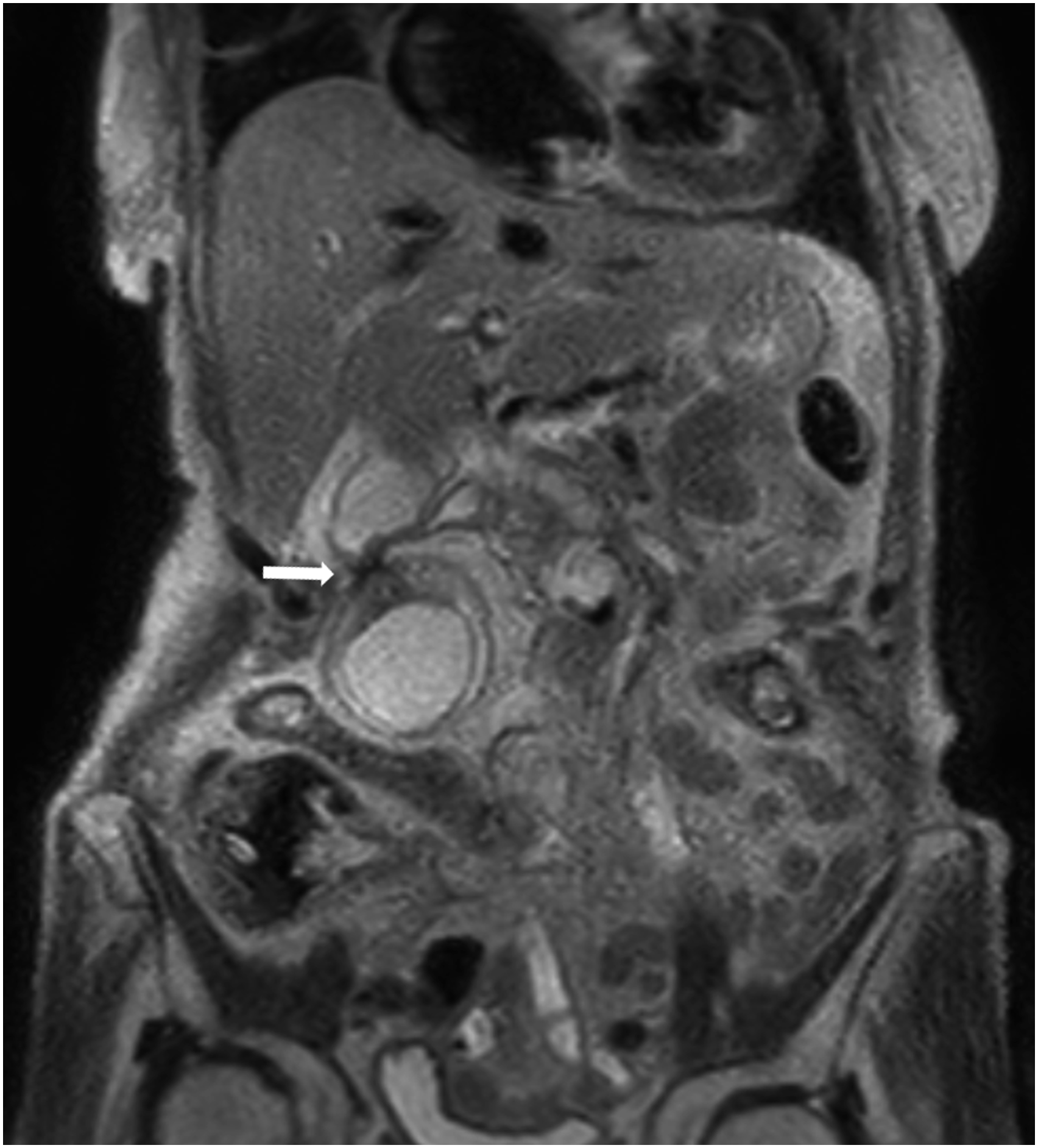
A contrast computed tomography (CT) scan showed a constriction in the gallbladder body and marked edematous wall thickening in the gallbladder fundus (Figure 1(a)). A 2-cm stone was found in the gallbladder neck, but no wall thickening was observed (Figure 1(b)). Findings were suggestive of torsion at the constriction site, as well as of ischemia, such as strong wall thickening of the gallbladder wall and poor contrast effect, so the patient was diagnosed with gallbladder torsion (Figure 2). Preoperatively, magnetic resonance imaging (MRI) showed findings suggestive of torsion in the body (Figure 3). Additionally, a high diffusion-weighted image (DWI) signal was found in the gallbladder wall at the gallbladder fundus and a decrease in the apparent diffusion coefficient (ADC) map, which were suggestive of ischemia (Figure 4). Contrast-enhanced computed tomography (CT) image (axial image, late phase). Marked edematous wall thickening is found at the gallbladder fundus, and the gallbladder wall is poorly enhanced (A, arrow). A stone was found in the gallbladder neck, but the gallbladder wall was not thickened (B, arrow). (a) Contrast-enhanced computed tomography (CT) image (coronal image, late phase). (b) CT image (sagittal image, late phase). Coronal and sagittal images show a constriction in the gallbladder body (arrow). Coronal images also show signs of torsion (A, arrow). Wall thickening with a poor contrast effect is seen in the gallbladder fundus (arrowhead). T2WI of magnetic resonance imaging (MRI) (coronal image). T2WI of MRI shows constriction in the gallbladder body and signs of torsion are also observed (arrow). (a) Diffusion-weighted image (DWI). (b) Apparent diffusion coefficient (ADC) map. DWI shows diffuse high signal intensity in the gallbladder wall (A, arrow). Part of the gallbladder wall shows a decrease in the ADC map, suggesting ischemia (B, arrow).

We decided to perform emergency surgery on the same day. Laparoscopy showed that the gallbladder body was strangulated by a band, and the fundus was dark red, suggesting ischemia (Figure 5). After we incised the band to release the strangulation, we performed a four-port laparoscopic cholecystectomy and placed a C-tube in the cystic duct because common bile duct stones were found preoperatively. The gallbladder torsion was mild, and ischemia was caused by the band; therefore, the patient was diagnosed with strangulated cholecystitis. Intraoperative findings. A band is formed due to adhesions on the gallbladder body, and the fundus is discolored dark red.
Pathological findings showed a clear boundary between ischemic and nonischemic changes in the resected specimen, and histological findings showed chronic cholecystitis with hemorrhage and congestive ischemic areas (Figure 6). The postoperative course was uneventful, and the patient was discharged after 18 days. Resected specimen. The boundary between the ischemic and nonischemic changes in the specimens is clear.
Discussion
Gallbladder torsion and strangulated cholecystitis are difficult to differentiate preoperatively. In our case, we diagnosed gallbladder torsion based on imaging findings and strangulated cholecystitis postoperatively. However, we believe that the two may be differentiated by knowing the characteristic imaging findings of gallbladder torsion and strangulated cholecystitis.
In gallbladder torsion, CT scans reveal anatomical abnormalities in the gallbladder’s position, a mass-like shadow or whirl sign in the gallbladder neck, and a V-shaped deformation of the extrahepatic bile duct caused by traction of the cystic duct. 7 Magnetic resonance cholangiopancreatography (MRCP) also reveals the displacement of the enlarged gallbladder toward the midline, a tapering or interruption of the cystic duct, differences in signal intensity between the extrahepatic bile duct, cystic duct, and gallbladder, and a V-shaped deformation of the extrahepatic bile duct. 7
Conversely, the gallbladder is slightly deviated in cases of strangulated cholecystitis, and no tapering or interruption of the cystic duct or V-shaped deformation of the extrahepatic bile duct due to traction of the cystic duct is observed. 5
The biggest difference is the location of damage to the gallbladder. In gallbladder torsion, ischemic changes occur throughout the gallbladder, whereas in strangulated cholecystitis, ischemia occurs in the gallbladder fundus with no gallbladder neck damage. Thus, the gallbladder appears in two distinct compartments in the gallbladder body on imaging.3–6 In other words, the gallbladder fundus showed reduced or absent contrast effects on contrast-enhanced CT, and MRI showed high DWI signals and reduced ADC maps, suggesting ischemia. Moreover, the gallbladder neck appears normal on CT and MRI. 5
In our case, CT and MRI showed significant ischemic changes in the fundus, whereas the neck was almost normal. In strangulated cholecystitis, the imaging findings have been reported to show the gallbladder body divided into two compartments.3–6
In conclusion, strangulated cholecystitis is a rare but serious disease that requires surgery. It is difficult to differentiate from gallbladder torsion, but we believe that it is possible to distinguish between the two based on the characteristic imaging findings of both. It is important to know the differences in imaging findings in order to make a correct diagnosis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient and her legal guardian for the publication of case details and images.