
Abstract
The purpose of this report was to evaluate the usefulness of hyperdense whirl sign on unenhanced computed tomography (CT) for diagnosing gallbladder torsion. The CT scans of seven patients with gallbladder torsion were independently reviewed by two board-certified radiologists for locating the high-density core with twisting between the gallbladder neck and liver bed, termed hyperdense whirl sign. The sign was observed in six cases. The detection of a hyperdense whirl sign on unenhanced CT appears useful for diagnosing gallbladder torsion.
Introduction
Gallbladder torsion is a rare entity that occurs most commonly in the elderly and is difficult to diagnose preoperatively. They tend to present with upper abdominal pain, and therefore, one of the most important differential diagnoses is acute cholecystitis. The presence of redundant mesentery is a prerequisite for torsion.
1
Computed tomography (CT) can often provide important diagnostic clues. Through our experience with these cases with torsion, we noticed that a high-density structure in the pedicle with a twisted appearance can be seen between the gallbladder neck and liver bed on the unenhanced CT images (Figure 1). We termed this finding a “hyperdense whirl sign.” Uncontrasted axial computed tomography image of slice thickness 5 mm in a patient with gallbladder torsion. 87-year-old woman with gallbladder torsion presented with an acute onset of abdominal pain in the right lower quadrant area. A close examination revealed that the gallbladder was not fixed in the liver bed and rotated around its pedicle in a 180° counterclockwise direction (incomplete torsion). A central high-density core is observed in the pedicle, which has a twisted appearance (white arrow).
Information on patient informed consent
Informed consent was obtained from all individual participants included in this study.
Patients
We performed a computerized search of the radiology information systems of three affiliated hospitals to identify patients who had undergone abdominal CT and subsequent cholecystectomy with an operative proof of gallbladder torsion between March 2015 and December 2019. The median age of the patients was 86 years (range, 21–92 years).
CT imaging
CT examinations were performed using two different machines: a 320-channel multidetector CT scanner (MDCT; Aquilion One; Canon Medical Systems, Otawara, Japan) in three patients and a 64-channel MDCT scanner (LightSpeed Ultra or LightSpeed VCT; GE Healthcare, Milwaukee, WI) in four patients. All patients underwent both unenhanced and enhanced CT scans of the abdominopelvic regions. Unenhanced CT was obtained with a slice thickness of 5 mm in two of the patients with torsion; unenhanced and enhanced CT scans were obtained with a slice thickness of 1.00 or 1.25 mm in all other patients. In routine scanning, unenhanced and contrast-enhanced images were acquired, starting 100 s after the infusion of 460-mgI/kg nonionic contrast material (Iopamidol 300; Bayer Pharma, Osaka, Japan) or 100-ml nonionic contrast material (Iopaque 300 or 240; Fuji Pharma, Tokyo, Japan) injected after 60 s.
Image evaluation
Two radiologists with 10 and 30 years of experience in abdominal radiology participated in a retrospective review of the density of pedicles and prevalence of the whirl sign on unenhanced CT.
The density of the pedicles was compared with the adjacent portal vein. Hyperdense whirl sign was defined as the presence of a high-density core within the pedicle, with a twisted appearance, between the gallbladder neck and liver bed. Multiplanar reformations (MPRs) were performed if the finding was equivocal on the axial images. In the event of interobserver disagreement, a final decision was reached by consensus. We did not calculate the κ statistic for the interobserver difference because only minor variations in interpretation were noted between the two readers.
Case history
All cases presented to our hospital for acute abdominal pain. Patients typically present with abdominal pain, nausea, and occasional vomiting. The symptoms and laboratory examinations are nonspecific. Emergency CT studies were performed, and we suggested gallbladder torsion. They underwent emergency surgery and were diagnosed with gallbladder torsion.
Results
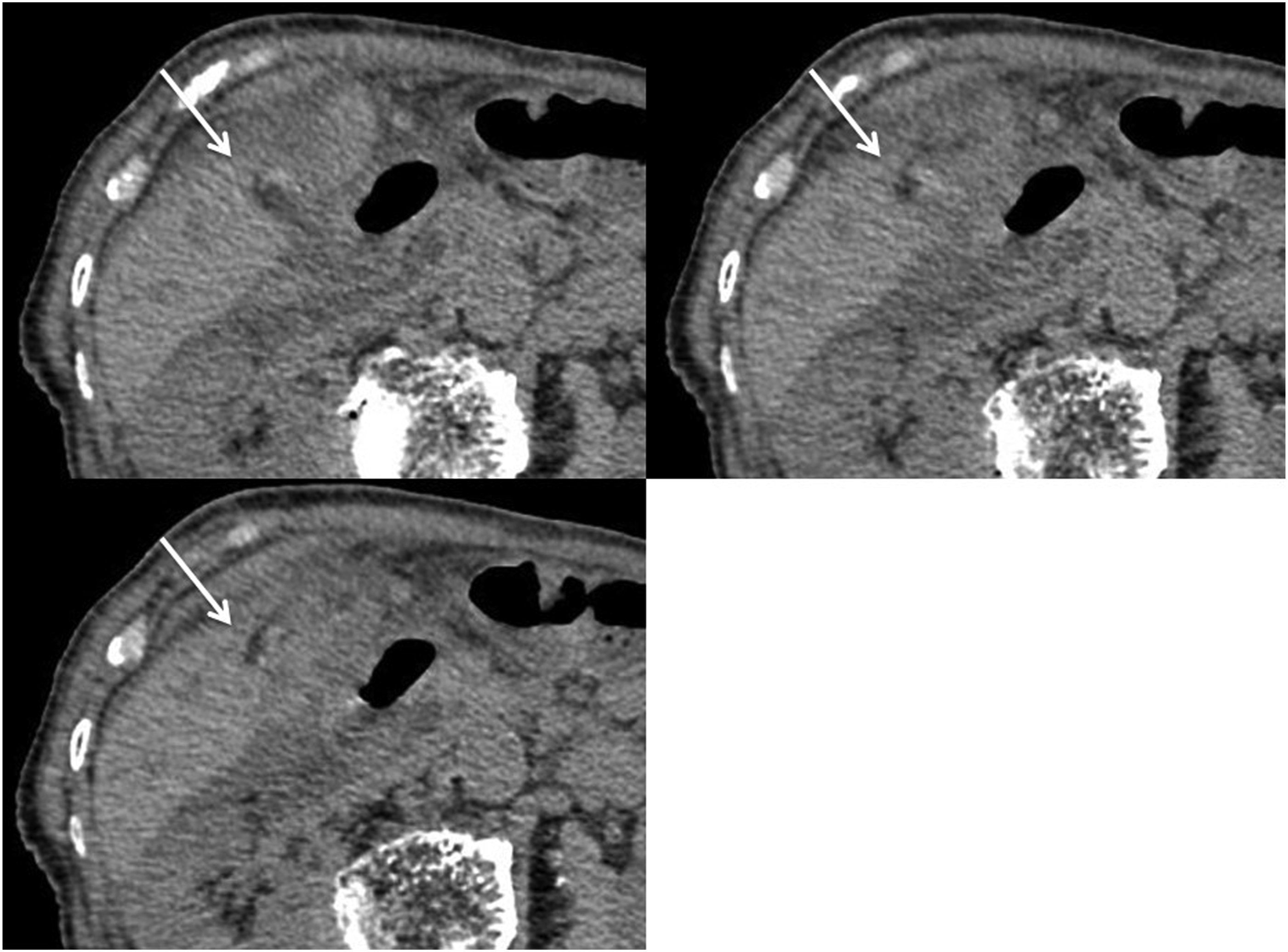
The core had a high density in five cases and slightly high density in two cases (Figures 2 and 3). The whirl sign was clearly seen in five cases and was considered likely in one case. In one case, the whirl sign was most evident on the MPR images. Uncontrasted serial axial computed tomography images of slice thickness 1 mm in a patient with gallbladder torsion. A 71-year-old woman with gallbladder torsion presented to our hospital for right upper quadrant pain of ∼3 days in duration. A close examination revealed that the floating gallbladder rotated around its pedicle in a 720° counterclockwise direction. The central core shows the high density is twisting with the surrounding fat (white arrows). Uncontrasted serial axial computed tomography images of slice thickness 1 mm in a patient with gallbladder torsion. An 86-year-old woman with gallbladder torsion presented to our hospital for right low quadrant pain of 1 day in duration. A close examination revealed that the gallbladder was not fixed in the liver bed and rotated around its pedicle in a 180° clockwise direction (incomplete torsion). Note the fat and soft tissue surrounding the central core (white arrows).
Discussion
Gallbladder torsion is a rare condition that can occur at any age. It is most commonly observed in patients between the sixth and eighth decades of life. It is associated with kyphoscoliosis or a generalized loss of elastic and adipose tissues, and it is also known to be associated with wandering gallbladder. Although this condition is a surgical emergency, the clinical presentation is nonspecific and can mimic other abdominal conditions. The preoperative diagnosis of gallbladder torsion is solely based on the radiological evaluation.
The characteristic CT features of gallbladder torsion include a distended and enlarged gallbladder with mural hemorrhage, a V-shaped distortion of the extrahepatic ducts, and a change in the anatomical position of the gallbladder from vertical to horizontal. The twisting of the pedicle containing the cystic duct and artery has been shown on contrast-enhanced MDCT, as well as poor enhancement of the gallbladder wall.2–6
In this report, there was a central high-density core in the pedicle between the gallbladder and liver bed in many cases. Two of these cases showed only a slight high density.
Previous case studies have reported the whirl sign on contrast-enhanced CT as a direct detection of gallbladder torsion.3,5,7 In this report, however, we could point out this diagnostic CT finding of gallbladder torsion on unenhanced CT. We, thus, consider that the visualization of the hyperdense whirl sign on unenhanced CT is a strong indicator of gallbladder torsion.
In gallbladder torsion, the cystic artery/vein, which lies within the cystic mesentery, twists together with the cystic duct. Layton et al. reported that the torsion of the vascular pedicle and surrounding fat creates a mini “swirl” appearance, 5 and Yokoi et al. demonstrated a twisted cystic artery on 3D-CT angiography. 8 For this reason, we consider that the hyperdense core seen on unenhanced CT indicates a thrombus in the twisted gallbladder mesentery in many cases. However, in some cases, a high density in the central core can indicate twisting of the cystic duct.
In conclusion, a hyperdense whirl sign was found on unenhanced CT in all the cases of gallbladder torsion. This sign could be useful for diagnosing gallbladder torsion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.