
Abstract
Background
Metal artifact reduction sequence magnetic resonance imaging (MRI) scan is a common method to detect adverse reaction to metal debris in total hip arthroplasty (THA). It might be quicker and cheaper if ultrasonography (US) could screen for the need for an MRI. However, both require trained personnel.
Purpose
We aimed to investigate the sensitivity and specificity of US for detecting pseudotumors (PT) when performed by an orthopedic surgery resident compared to MRI. We also investigated the sensitivity and specificity of US to detect PTs in obese and non-obese patients.
Material and methods
We examined 205 patients with hip resurfacing arthroplasty, metal-on-metal or metal-on-polyethylene THA with both MRI and US. US was performed by an orthopedic surgery resident who was trained according to a standardized training program in musculoskeletal US. Results from MRI were used as gold standard.
Results
US had a sensitivity of 0.92 (95% CI 0.81–0.98) and specificity of 0.94 (95% CI 0.89–0.97) for detecting PT. It had a positive predictive value of 0.84 (95% CI 0.73–0.91) and a negative predictive value of 0.97 (95% CI 0.93–0.99). US performed similarly in obese and non-obese patients.
Conclusions
US had a high sensitivity and specificity for detecting PT when performed by an orthopedic surgery resident. Trained orthopedic surgeons could screen for the need of an MRI scan when searching PTs.
Keywords
Introduction
Total hip arthroplasty (THA) with metal-on-metal (MoM) bearings are almost no longer used as they have high complication and revision rates.1,2 These THA produce metal ion release 3 which may cause adverse reaction to metal debris (ARMD) also called adverse local tissue reaction such as pseudotumors (PT).4–6 PTs also form around metal-on-polyethylene (MoP) THA probably due to trunnion wear.7–9 Some PTs might adversely affect the patients’ health10–12 while others are asymptomatic. 11 The majority of PTs seem to stabilize or regress13–15 and risk of complications after revision for ARMD and PTs is high. 16 However, some countries have introduced lifelong follow-up programs for MoM hip arthroplasties. 3 Therefore, repeated diagnostic imaging might be needed before the surgeon decides to perform surgery.
The gold standard for detecting PTs is a metal artifact reduction sequence (MARS) MRI scan. However, MRI is expensive, time consuming, and in some places the availability of MRI is low. 17 Furthermore, some patients might have absolute or relative contraindications to have an MRI scan performed. Therefore, several studies have suggested the faster and cheaper US as an alternative or supplement to MRI17–20 with sensitivity and specificity ranging from 0.69 to 0.90 and 0.83 to 0.92 when performed by experienced musculoskeletal radiologists. Some even using repeat US to observe PTs. 21 However, experienced musculoskeletal radiologist with special interest in US is not available at every hospital. If other trained clinicians could accurately perform US of the hips, US could be performed to assess the need for MRI, thereby prioritizing the time and skills of musculoskeletal radiologists. However, no study has to our knowledge investigated how a non-radiologist performs when detecting PTs with US. Further, obese patients have a greater distance from the hip to the US probe, 22 but obesity’s effect on sensitivity and specificity for PTs have not been studied. Therefore, we aimed to investigate the sensitivity and specificity when an orthopedic surgery resident after a short training program performed US scans on patients with THA to detect PTs compared with MARS-MRI as a gold standard. Second, we investigated the sensitivity and specificity for US to detect PTs in obese and non-obese patients.
Material and methods
We conducted a cross-sectional cohort study where US and MARS-MRI were compared including patients operated at 2 hospitals. The cohort consisted of patients with hip resurfacing arthroplasty (HRA) (ASR, Depuy) and MoM THA (M2a-Magnum, Biomet). In 2011, all patients with these 2 types of hip arthroplasty and operated at the 2 centers during 2005–2010 were invited. Further, we had a matched control group of patients with MoP THA from those 2 centers from the same period, matched with the first 50 from HRA patients at 1 of the centers. The control group was matched on sex, age, and year of surgery. The cohort was part of another study into the prevalence of MARS-MRI detected PT between HRA, MoM, and MoP THA. In total, 205 patients with 121 HRA, 34 MoM, and 50 MoP THA were included in the cohort (Figure 1). Flowchart of inclusion and exclusion of patients. HRA: Hip resurfacing arthroplasty. MoM: Metal-on-metal. THA: Total hip arthroplasty. MoP: Metal-on-polyethylene.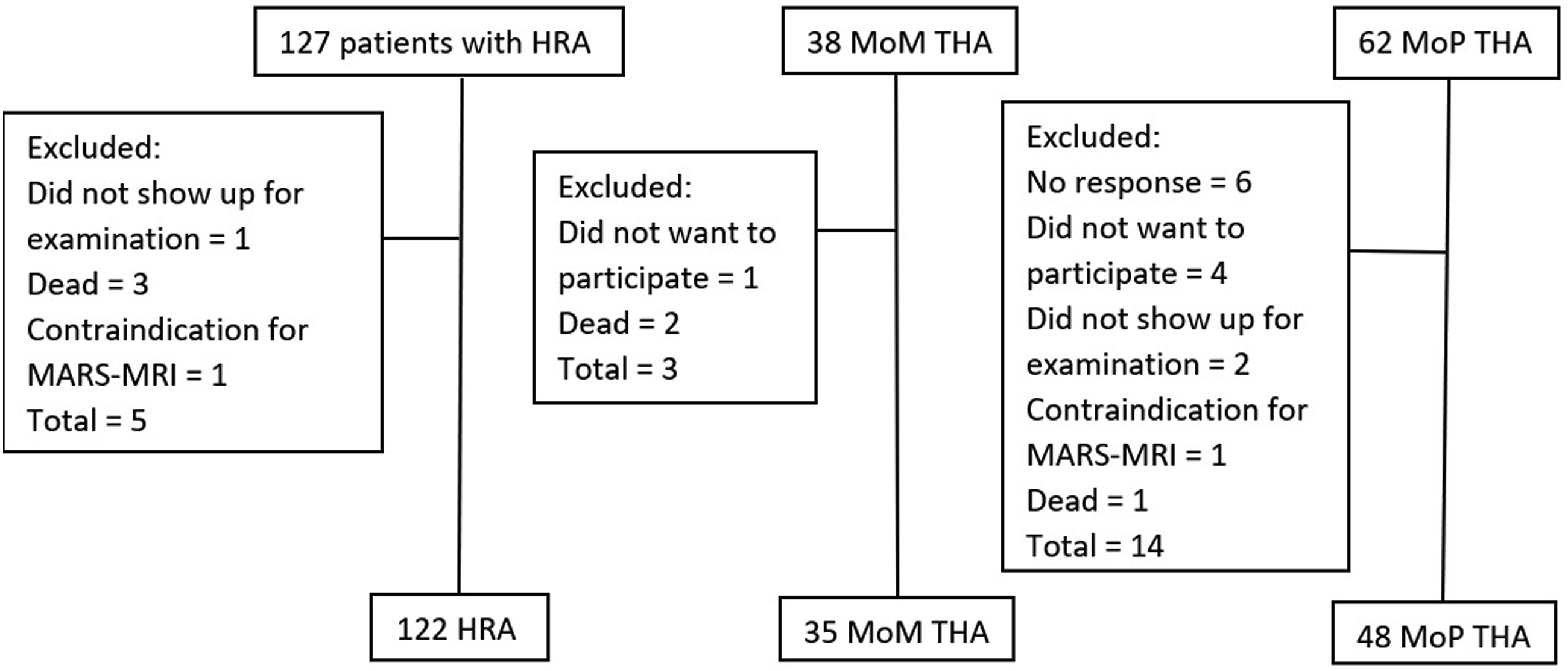
MRI scan
The MRI scans were performed in an open 1 T MRI scanner (Philips Panorama, Best, Nederland) with the following technical MARS-MRI sequences: transversal and coronal T1, coronal T2 and a coronal STIR. For reduction of artifacts resulting from the metal prothesis, the bandwidth was increased and matrix size altered. PT was defined as any mass, solid, cystic, or mixed, in continuity of the joint (Figure 2) according to the Hauptfleisch PT classification.
23
The Hauptfleisch PT classification consists of 3 categories: Type I: Thin-walled cystic mass (cyst wall <3 mm), Type II: Thick-walled cystic mass (cyst wall >3 mm, but less than the diameter of the cystic component) and Type III: A predominantly solid mass. Picture Archiving and Communications System (PACS) (General Electric Healthcare Centricity, Illinois, Ca, USA) was used for all MRI analyses. MRI images were reviewed by a senior consultant in radiology who is specialized in musculoskeletal MRI with more than 25 years of experience. The radiologist also re-evaluated all MRI images a minimum of 2 months after the first review and was blinded to the first review. Hauptfleisch Type II PT as seen on MRI and US (red arrows). The patient has a MoP THA. On the left is a MARS-MRI STIR sequence image in coronal plan showing left-sided Type II PT. On the right is a lateral transversal US showing a cystic Type II PT with little solid mass.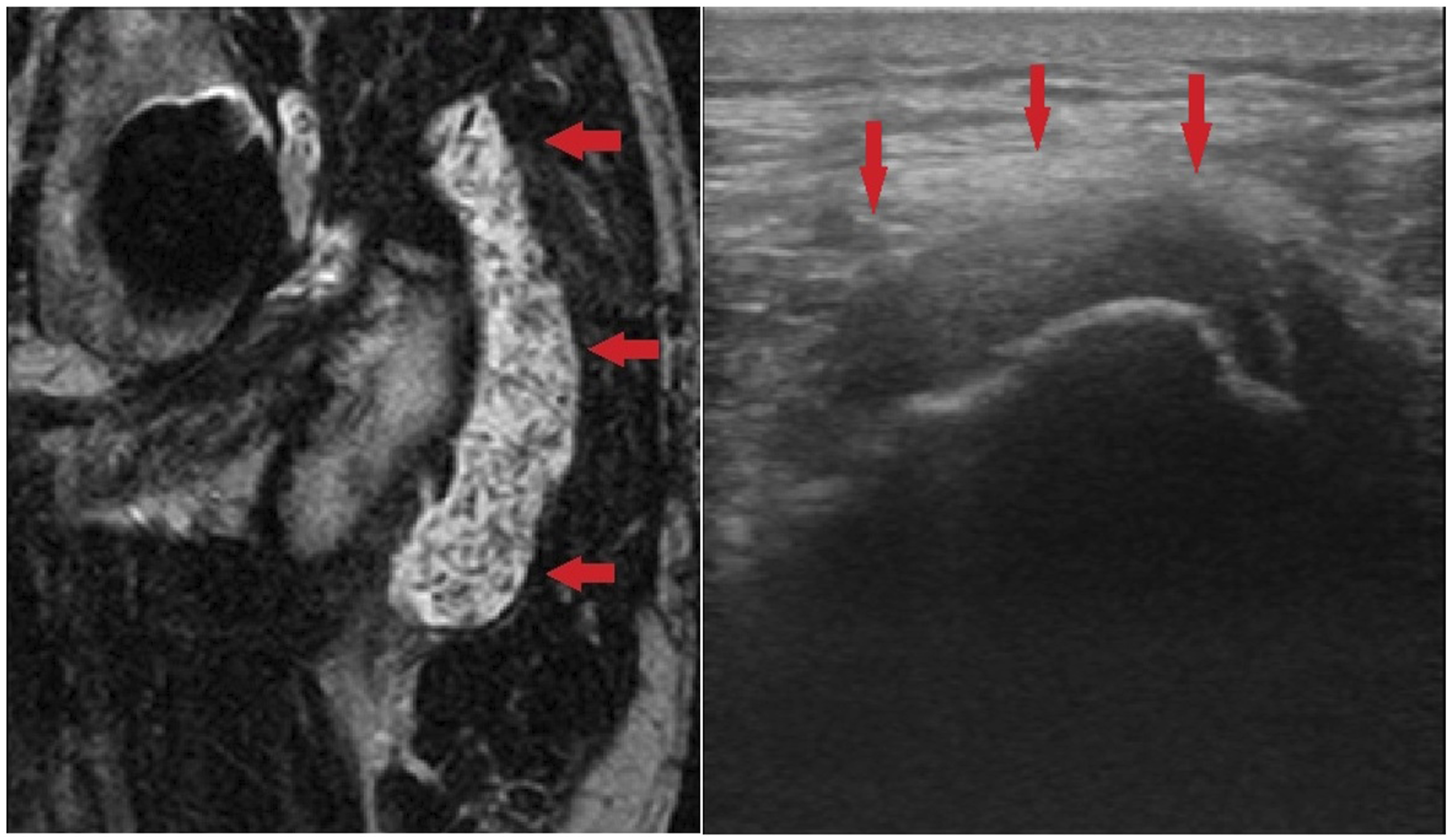
US
The US scans were performed with a 7L4s linear 5–10 MHz transducer (Mindray M7 high powered color doppler laptop, Mahwah, New Jersey, The United States). PT was defined as any cystic or solid mass, solid, cystic or mixed, in continuity of the existing hip joint (Figure 2). If cystic or solid masses were situated both in contact with the implant and in the adjacent tissue, they were assumed to be connected.
The US scans were performed by a single orthopedic surgery resident. The resident was trained according to the European Federation of Societies for Ultrasound in Medicine and Biology Guidelines ‘Minimum Training Requirements for Rheumatologists Performing Musculoskeletal Ultrasound’, 24 which in brief includes 300 US scans of joints, in this case only hips, supervised by an experienced radiologist. The results of the supervised US scans were not included in the results of this study. Each US examination consisted of 30 min of examination in 8 projections as recommended by Hansen et al. 22 The projections used were 1. Anterior, longitudinal/oblique 2. Anterior transversal 3. Medial, longitudinal/oblique 4. Medial, transversal. Projection 1–4 were done with the patient in a supine position. 5. Lateral, longitudinal/oblique 6. Lateral, transversal. Projection 5–6 were done with the patient in a lateral position. 7. Posterior, longitudinal 8. Posterior, transversal. Projection 7–8 were done with the patient in a prone position. For obese patients, the abdominal convex transducer (3.5–5 MHz) was used to create an overview, after that the above-mentioned transducer and method was used. Not all US images were stored, but the orthopedic resident filled out a chart of his findings during the examinations. We consider these charts the raw data.
Obesity
Body mass index (BMI) was obtained for all patients as the distance from the probe to the hip and surrounding tissue might affect the quality of the US scan. It was calculated by dividing the patients’ weight by their height squared as is the international standard. 25 We categorized patients as obese when BMI ≥30.
Statistics
Patient characteristics were given as medians and range. Results of the MRI scans were used as the gold standard, when calculating sensitivity, specificity, positive predictive value and negative predictive value of ultrasonography, and 95% confidence intervals (CI) were calculated. Sensitivity and specificity were calculated for all patients, for obese and non-obese, and for each type of arthroplasty. Data was analyzed in STATA statistical analysis software 16.1.
Ethics
Approval for the study was obtained from the National Committee on Health Research Ethics (reference number SJ-203, application number 27.938). Written and verbal informed consent was given in compliance with the Declaration of Helsinki.
Results
Patient characteristics. Female/male is given in numbers. Age, follow-up, and BMI are given as medians and range.

BMI: Body mass index. HRA: Hip resurfacing arthroplasty. MoM: Metal-on-metal. MoP: Metal-on-polyethylene.
PT distribution between type of hip arthroplasty and Hauptfleisch PT classification as found on MRI.

HRA: Hip resurfacing arthroplasty. MoM: Metal-on-metal. MoP: Metal-on-polyethylene.
Sensitivity, specificity, positive predictive value and negative predictive value with 95% confidence intervals (CI).

MRI: metal artifact reduction sequence magnetic resonance imaging.
We additionally calculated the sensitivity and specificity for non-obese and the obese and found a sensitivity and specificity of 0.89 (CI 0.74–0.97) and 0.92 (CI 0.85–0.97) for non-obese and 0.93 (CI 0.66–1.0) and 0.98 (CI 0.89–1.0) for obese. A subanalysis showed that the sensitivity in the HRA group was 0.94 (CI 0.79–0.99), 0.83 (CI 0.36–0.99) in the MoM group, and 0.80 (CI 0.44–0.97) in the MoP group, respectively. The specificity in the HRA group was 0.96 (CI 0.89–0.99), 0.90 (CI 0.70–0.99) in the MoM group, and 0.95 (CI 0.83–0.99) in the MoP group, respectively.
US did not find 4 out of the 50 PT found on the MRI, but US did find 9 PT, that were not found on the MARS-MRI. In 3 of the 4 false negative, the patients’ BMI ≥30 and the PT was situated medial to the implant Figure 3. Three patients had HRA and 1 had a MoP THA. The PTs were described on MRI as minimal in size. In 7 of the 9 false positive, the PT were typically situated close to the implants and measured marginally more than 10 mm. All cases of false negative and false positive were Hauptfleisch Type I.
Discussion
We conducted a cross-sectional cohort study comparing the ability of US to detect PT in patients with 3 types of hip arthroplasties, where the US scans were performed by a trained resident in orthopedic surgery. MRI findings were performed and considered the gold standard. We found overall sensitivity and specificity above 90% and similar sensitivity and specificity for obese and non-obese. This is to our knowledge the only study investigating a non-radiologist’s sensitivity and specificity to detect PTs with US.
The sensitivity and specificity found in our study were similar to that of other studies where the US scans were performed by radiologists.18–20 We had a similar follow-up to that of 2 of those 3 studies,18,19 and a shorter follow-up to that of another study. 20 The prevalence of MRI detected PT in our study was similar to that of Nishii et al. and Muraoka et al.18,20, but much lower than in the study by Siddiqui et al. 19 . Our protocol for MRI was similar to that of other studies, but our US scans also focused on a medial projection of the hip, which Nishii et al. and Siddiqui et al. did not, but Muraoka et al. did. The extra projection might have a better view and therefore better reveal PT.
Contrary to other studies in this field, most of our patients were male. This could have an effect as body fat distribution tend to be deposited on the hips in women and on the stomach in men. 26 Therefore, we might have had a shorter distance from the probe to the implant. This distance might also be affected by the patients’ BMI. In our study, the sensitivity and specificity were similar in the non-obese and obese groups. The trained orthopedic surgeon could reliably detect PTs in both groups. However, this study might be underpowered to detect any difference between the non-obese and obese group, and the BMI of most patients were just below or just above the non-obese/obese cutoff point. BMI was not included in other studies in this field18–20 so we cannot compare our results.
We found slight differences in the sensitivity and specificity for US to detect PTs in different types of arthroplasties. However, this study might be underpowered, and larger studies are needed to investigate the sensitivity and specificity for US to detect PTs between the different designs of hip implants.
There were some false positive and false negative findings of US. The false negative findings were small PTs situated medially to the hip in obese patients. US might have some limitations in these situations. The false positive PTs were marginally larger than 10 mm close to the implants and could have been overlooked on the MRI due to metal artifacts. This is similar to another study where US and MRI findings were compared to intraoperative findings of revised hip resurfacing arthroplasties. 27 However, we consider US and MRI agreement sufficient in our study for US to be used as a screening tool to assess the need for an MRI.
It is difficult to differentiate between postoperative seroma, bursitis, synovitis and pseudotumor. This point has also been made in previous studies in MRI.
28
Ultrasonography has the same limitations. The Hauptfleisch classification defines a PT as any mass solid or cystic in continuity
A limitation of this study is that the US scans were not cross-checked by an experienced musculoskeletal radiologist. However, the point of our study is not that US or orthopedic surgery residents should replace musculoskeletal radiologists, but rather to find a more efficient way to screen patients according to their need for more precise diagnostic imaging by preferably musculoskeletal radiologists. The musculoskeletal radiologist could then focus on describing the PTs in greater detail and precision. Our results show that most of our patients with PT would have been referred to MRI because of a positive US. Those patients that would not have been referred to MRI had small Type I PTs that typically are asymptomatic and stabilize or regress.11,14,29,30
Another limitation of this study is that repeated scans to assess intraobserver variability were not performed. As PT might have changed over time, we cannot redo the US scans to examine intraobserver variability. However, given the high sensitivity and specificity, we still consider the results reliable.
The use of power-Doppler might have improved the US scans by visualizing inflammation. However, we kept the US scans as simple as possible to demonstrate the utility of US in the hands of inexperienced personnel.
In conclusion, we found that an orthopedic surgery resident after a short training program could diagnose PT around hip arthroplasty using US with acceptable sensitivity and specificity compared to MRI scans. US performed similarly in obese and non-obese patients. In perspective, orthopedic surgeons can be trained to reliably screen patients for the need of an MRI when detecting pseudotumors. (See Figure 3) Small medial PTs of less than 10 mm anterior of the femoral neck/implant only visible on US and not MRI.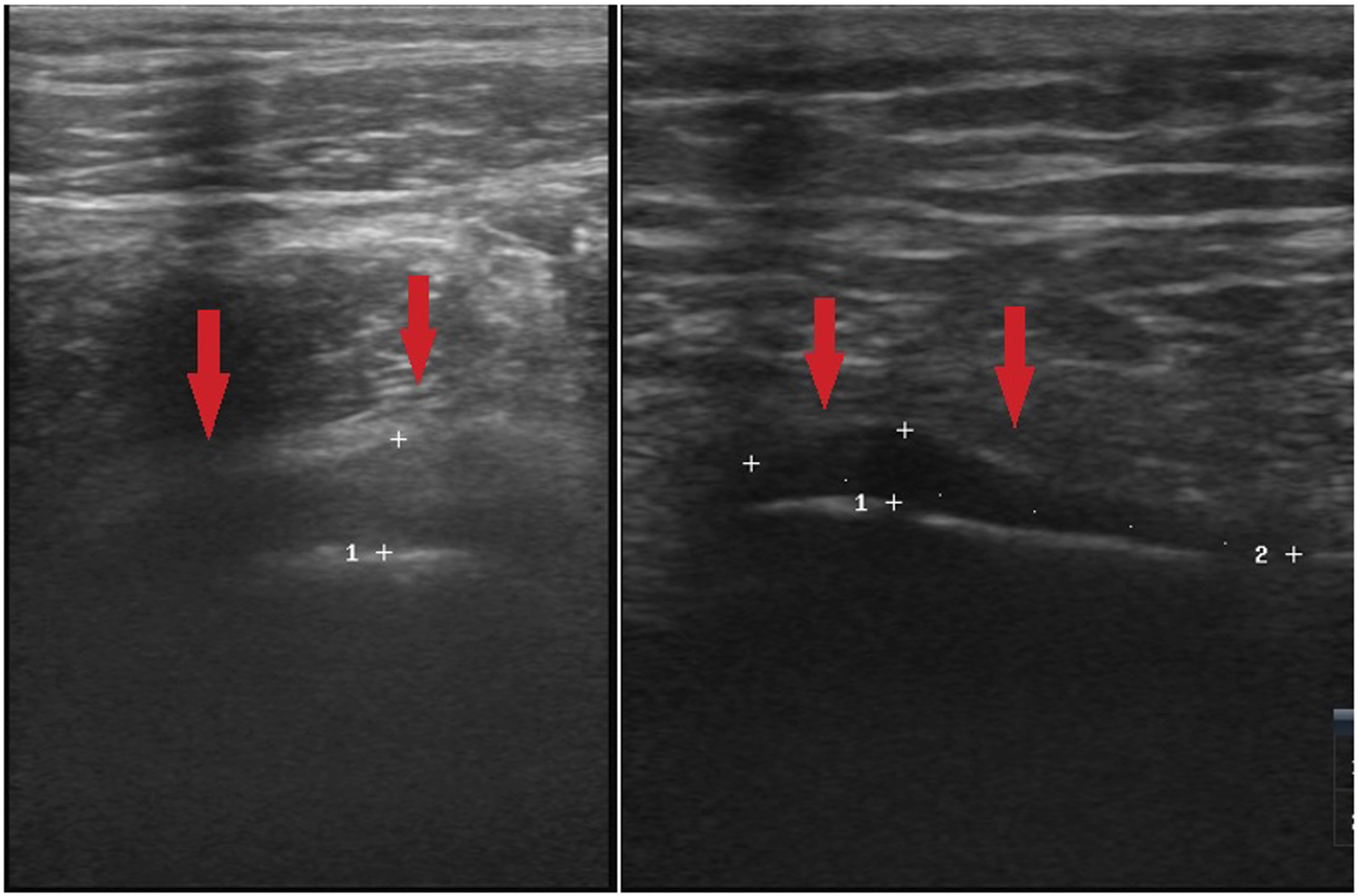
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: One authors received salary via a scholarship of the University of Southern Denmark.