
Abstract
Background and Aims:
Large headed metal-on-metal total hip arthroplasty may produce more metal ions than hip resurfacing arthroplasty. Increased metal-ion levels may be associated with higher revision rates due to adverse reaction to metal debris. The purpose of our study was to compare the survivorship of three hip resurfacing arthroplasty designs with their analogous cementless large-diameter head metal-on-metal total hip arthroplasties.
Material and Methods:
Based on data obtained from the Finnish Arthroplasty Register, the revision risks of three metal-on-metal hip resurfacing arthroplasty/total hip arthroplasty design couples performed during 2001–2011 were analyzed using the Cox regression model.
Results:
In the Cox regression analysis for compared design pairs adjusted for age, gender, operated side, head size, diagnosis, and implant, there was no statistically significant difference in revision risk between ReCap hip resurfacing arthroplasty and Bimetric/ReCap total hip arthroplasty (risk ratio = 1.43, confidence interval = 0.95–2.14, p = 0.09) or between Birmingham hip resurfacing arthroplasty and Synergy/Birmingham hip resurfacing total hip arthroplasty (risk ratio = 1.35, confidence interval = 0.75–2.43, p = 0.31). However, the revision risk of Corail and Summit/articular surface replacement total hip arthroplasty (ASR HRA) was significantly increased compared to ASR HRA. (risk ratio = 0.73, confidence interval = 0.54–0.98, p = 0.04).
Conclusion:
We conclude that the short-term revision risk of large headed metal-on-metal total hip arthroplasties was not increased compared to analogous hip resurfacing arthroplasties in two out of three devices studied at a nationwide level. There may be implant-related factors having an effect on the success of single manufacturer devices. However, more information on the incidence of adverse soft-tissue reactions in these patient cohorts is needed.
Keywords
Introduction
Hip resurfacing arthroplasty (HRA) and large-diameter head metal-on-metal total hip arthroplasty (LDH MoM THA) have gained popularity during the last decade in hip surgery (1–4). Recently, increased numbers of MoM bearing surface wear complications have been detected (5–7). Concerns exist regarding the consequences of prolonged exposure to increased metal-ion levels, such as adverse reaction to metal debris (ARMD) (8, 9). It has been stated that although HRAs and LDH MoM THAs have the same bearing characteristics, wear and corrosion at the junction between the femoral neck and the adapter sleeve, as well as the open femoral head design, are suspected to be responsible for the additional load of metal-ion release (10). The revision risk of LDH MoM THAs as a group has been increased compared with that of HRAs according to register data (11, 12). The aim of our study was to analyze the early outcome of three HRA designs and compare it with that of analogous LDH MoM THAs from the data of the Finnish Arthroplasty Register.
Material and Methods
The Finnish Arthroplasty Register
Since 1980, the Finnish Arthroplasty Register has been collecting information on total hip replacements (13). Health-care authorities, institutions, and orthopedic units are obliged to provide the National Institute for Health and Welfare with information essential for maintenance of the registry. Since 1995, the data of the registry have been compared with those of hospital discharge registries at regular intervals. Currently, 98% of implantations are recorded. An English translation of the notification form used by the Finnish Arthroplasty Register has been discussed previously (14).
Study Population and Inclusion Criteria
During the study period 2001–2011, 5464 Bimetric/ReCap THAs (Biomet, Warsaw, IN, USA), 698 ReCap HRAs (Biomet), 475 Synergy/Birmingham hip resurfacing (BHR) THAs (Smith & Nephew, Memphis, TN, USA), 1902 BHR HRAs (Smith & Nephew), 632 Corail and Summit/articular surface replacement (ASR) THAs (DePuy, Warsaw, IN, USA), and 979 ASR HRAs (DePuy) were performed in Finland. To reduce the skew in the demographic distribution between patients operated with HRA and those operated with THA, patients older than 85 years of age were excluded (the oldest patient operated with HRA was 85 years old). In addition, those patients with a diagnosis of other reasons (including fractures and avascular necroses of femoral head) or rheumatoid arthritis were excluded. Demographic data are given in Table 1.
Demographic data relating to HRAs and THAs in 10,150 hips.
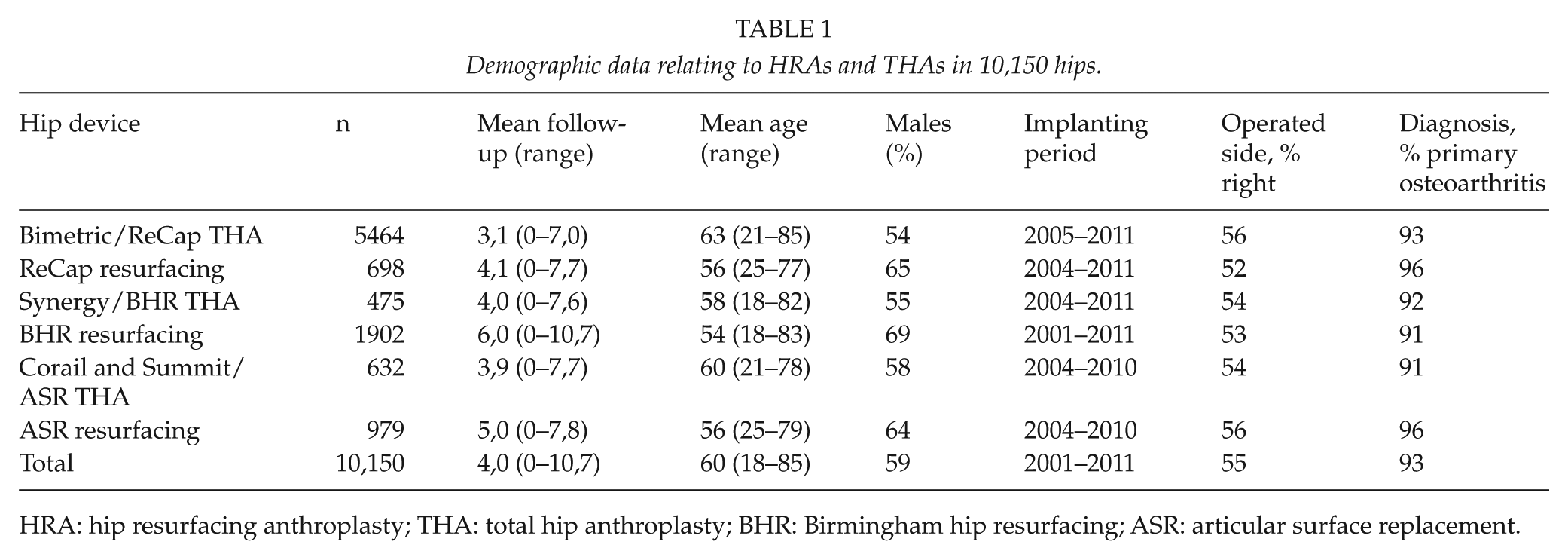
HRA: hip resurfacing anthroplasty; THA: total hip anthroplasty; BHR: Birmingham hip resurfacing; ASR: articular surface replacement.
Hip Resurfacing Versus LDH MoM THA
The revision risk of ReCap HRA was compared with that of Bimetric/ReCap THA, the revision risk of BHR HRA was compared with that of Synergy/BHR THA, and the revision risk of ASR HRA was compared with that of Corail and Summit/ASR THA performed during the same time period with adjustment for age at surgery, gender, operated side, head size <50 or ≥50 mm, and diagnosis, using Cox multiple regression analysis. In addition, stratified analyses were performed for males and females aged <55 or ≥55 years. In these sub-analyses by age and gender, the revision risk of LDH MoM THAs was compared with the revision risk of analogous HRAs performed for similar patients during the same time period.
Statistical Analysis
Revisions were linked to the primary operation by using a personal identification number. The end point for survival was defined as revision when either one component (including the femoral head) or the whole implant was removed or exchanged. Revision for any reason, revision for aseptic loosening, revision for dislocation, revision for infection, and revision for periprosthetic fracture each served separately as an end point. In 41 revisions, the recorded indication for revision was “other reason.” Kaplan–Meier survival data were used to construct the survival probabilities of implants. These survival data were compared using the log-rank test. Patients who died or left Finland during the follow-up period were censored at that point. The Cox multiple regression model was used to study differences between groups and to adjust for potential confounding factors. The factors studied with the Cox model were age, gender, diagnosis, and implant design. The effect of age on survivorship was also analyzed by dividing the patients into two age groups: those under 55 years and those 55 years and older. Cox regression analyses provided estimates of survival probabilities and adjusted risk ratios (RRs) for revision. Estimates from the Cox analyses were used to construct adjusted survival curves at mean values of the risk factors. The Wald test was applied to calculate p-values for data obtained from the Cox multiple regression analysis. Differences between groups were considered to be statistically significant if the p-value was less than 0.05 in a two-tailed test.
Results
According to the revision reasons recorded in the register, the most common reason for revision was aseptic loosening of both components. In the Cox regression analysis, there was no statistically significant difference in revision risk between ReCap HRA and Bimetric/ReCap THA (RR = 1.43, confidence interval (CI) = 0.95–2.14, p = 0.09) or between BHR HRA and Synergy/BHR THA (RR = 1.35, CI = 0.75–2.43, p = 0.31). However, the revision risk of Corail and Summit/ASR THA was significantly increased compared with that of ASR HRA (RR = 0.73, CI = 0.54–0.98, p = 0.04) (Table 2, Figs 1 to 3).
Survival of HRA and THA, the reference group. HRAs compared to THAs; adjustment made for age, gender, operated side, head size, diagnosis, and implant.
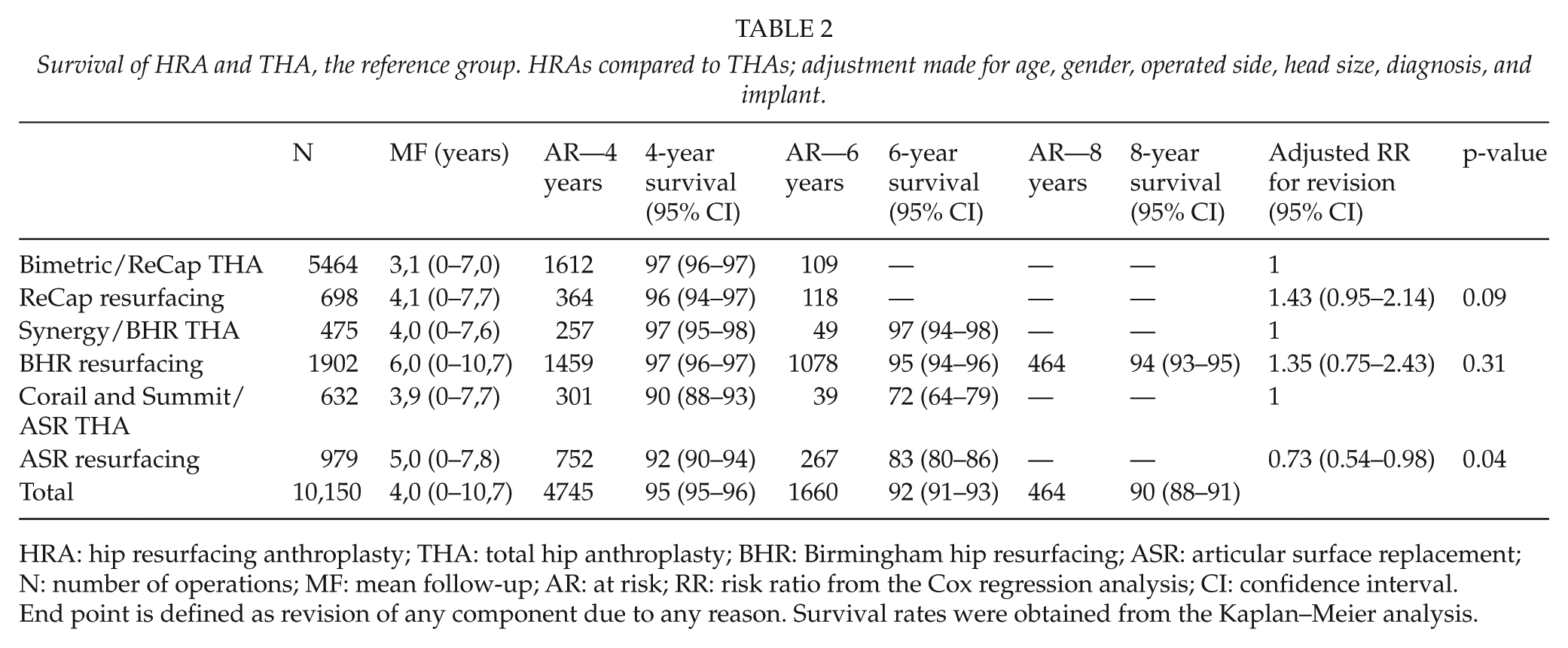
HRA: hip resurfacing anthroplasty; THA: total hip anthroplasty; BHR: Birmingham hip resurfacing; ASR: articular surface replacement; N: number of operations; MF: mean follow-up; AR: at risk; RR: risk ratio from the Cox regression analysis; CI: confidence interval.
End point is defined as revision of any component due to any reason. Survival rates were obtained from the Kaplan–Meier analysis.
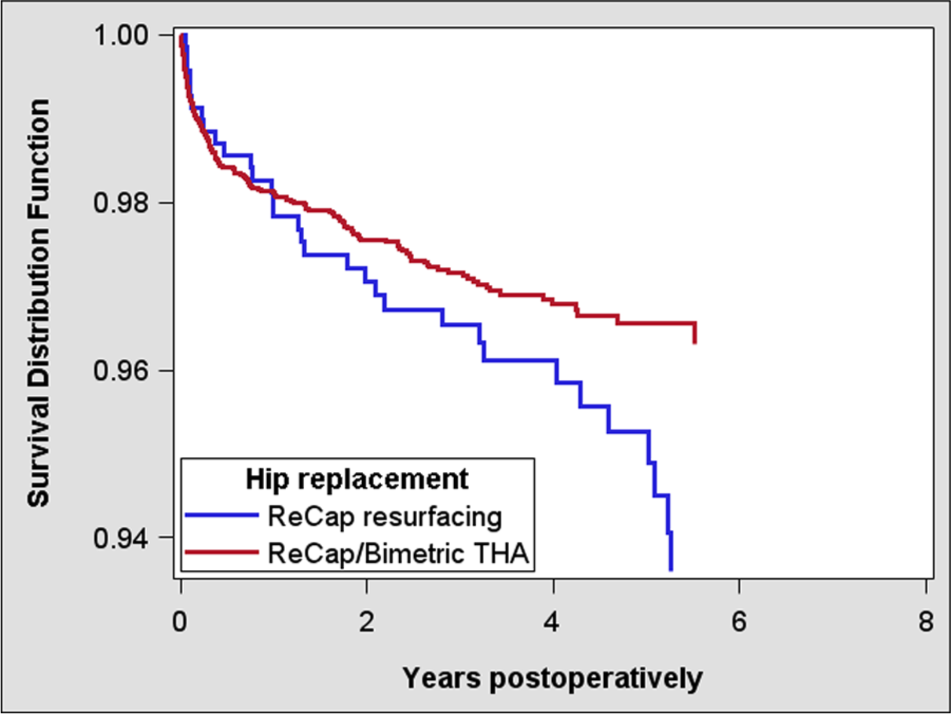
Cox-adjusted survival curves of 698 ReCap resurfacings and 5464 ReCap/Bimetric THAs.
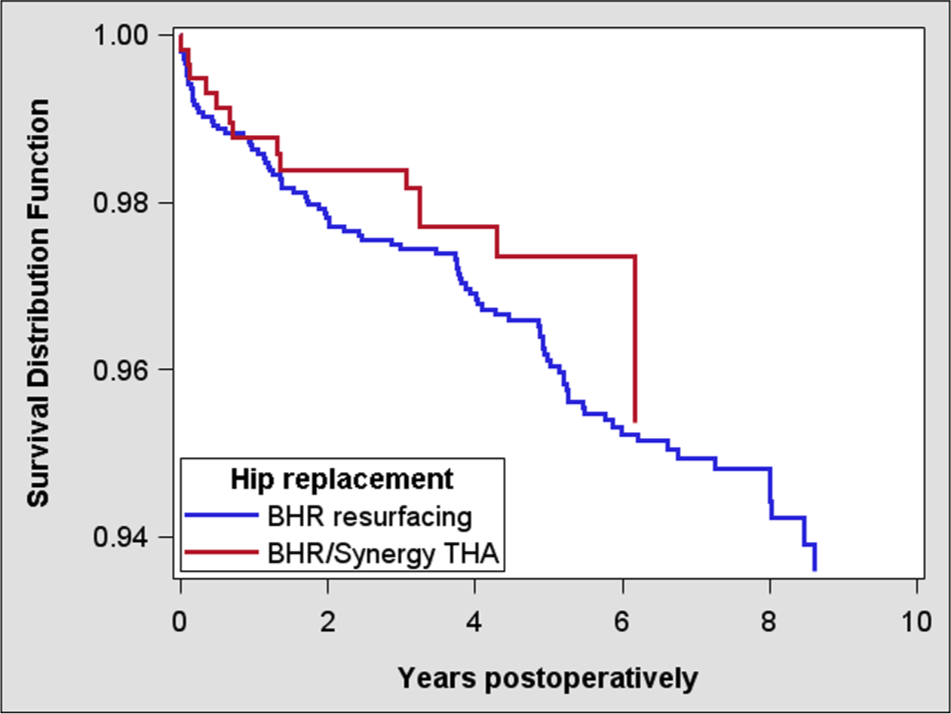
Cox-adjusted survival curves of 1902 BHRs and 475 BHR/Synergy THAs.
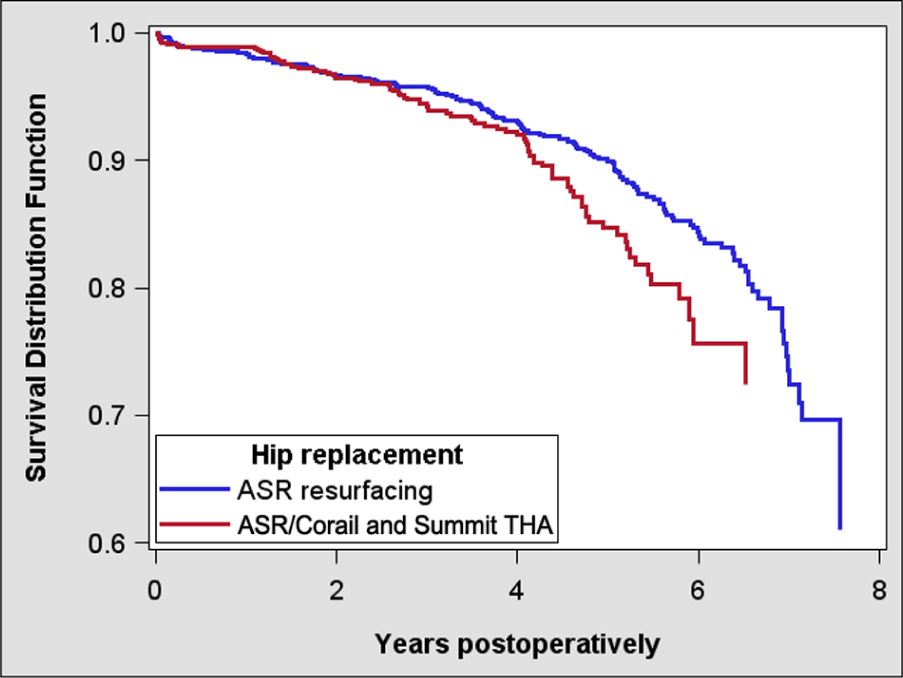
Cox-adjusted survival curves of 979 ASR resurfacings and 632 ASR/Corail and Summit THAs.
The revision risk of ASR HRA for aseptic loosening of both components was significantly decreased compared with that of Corail and Summit/ASR THA (p < 0.001). There was no statistically significant difference in revision risk for aseptic loosening between ReCap HRA and Bimetric/ReCap THA (p = 0.8) or between BHR HRA and Synergy/BHR THA (p = 0.2)
No difference was found in dislocation revision risk between the implant pairs compared. (ASR HRA vs ASR THA p = 0.4; BHR HRA vs BHR THA p = 0.5; ReCap HRA vs ReCap THA p = 0.7).
No difference was found in fracture revision risk between the implant pairs compared (ASR HRA vs ASR THA p = 0.2; BHR HRA vs BHR THA p = 0.5; ReCap HRA vs ReCap THA p = 0.2).
There was no difference in infection revision risk between implant pairs compared (ASR HRA vs ASR THA p = 0.2; BHR HRA vs BHR THA p = 0.95; ReCap HRA and ReCap THA p = 0.1).
The subgroup analysis by age and gender is provided in Table 3. Elderly male patients with Corail and Summit/ASR THA had an increased risk of revision compared to those with ASR HRA (RR = 0.48, 95% CI = 0.28–0.84, p = 0.01). Elderly female patients with ReCap HRA had an increased risk of revision compared to those with Bimetric/ReCap THA (RR = 3.52, 95% CI = 1.87–6.60, p < 0.001).
Age- and gender-stratified relative risk of revision. HRAs were compared to analogous LDH MoM THAs during the same period 2001–2011. Data are based on a Cox regression model adjusted for age, operated side, head size, diagnosis, and type of implant.
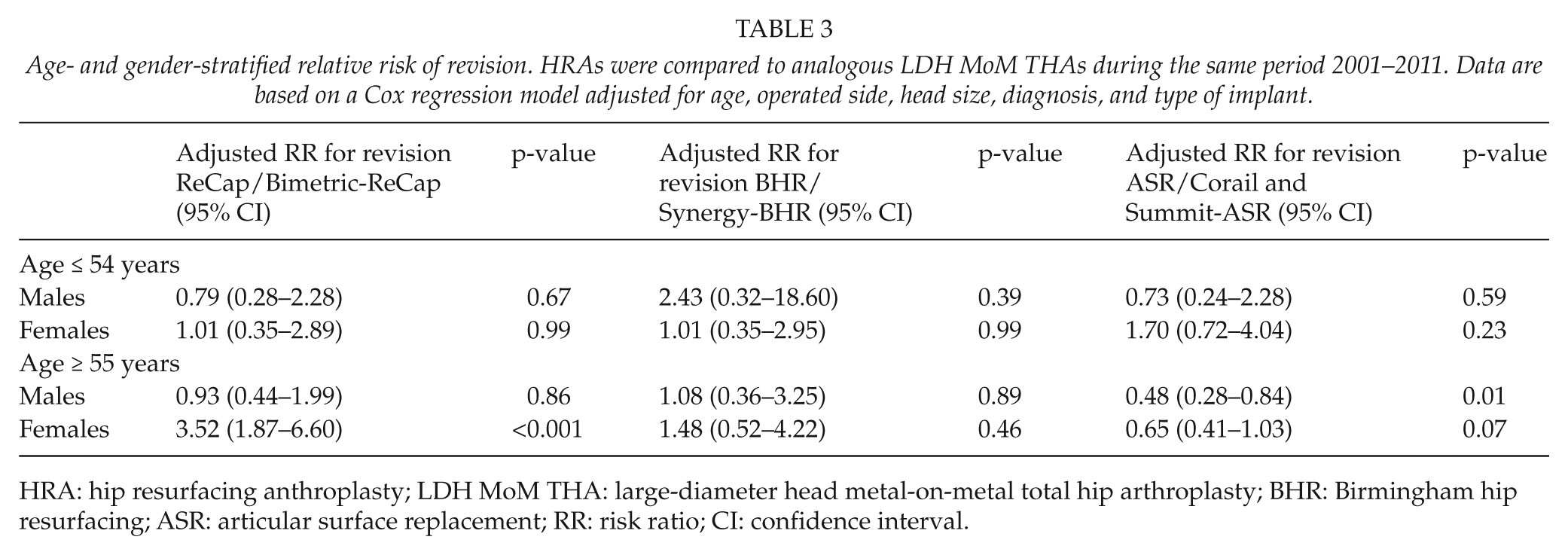
HRA: hip resurfacing anthroplasty; LDH MoM THA: large-diameter head metal-on-metal total hip arthroplasty; BHR: Birmingham hip resurfacing; ASR: articular surface replacement; RR: risk ratio; CI: confidence interval.
Discussion
We found out that the short-term revision risk of LDH MoM THAs was not increased compared to analogous HRAs in two out of three devices studied at a nationwide level. However, the revision risk of ASR THA was significantly increased compared to that of ASR HRA. Longer follow-up and more information on the incidence of adverse soft-tissue reactions in these patient cohorts are needed.
ASR and BHR cups and analogous HRA femoral components are all made of cast high-carbon-content cobalt–chromium alloy (10, 11). ReCap cup’s inner surface (bearing surface) is made of high-carbon-content cobalt–chromium alloy as well. The outer surface of the shell is covered with titanium alloy. The analogous Biomet HRA femoral component is made of cobalt–chromium alloy (12). The outer surface of BHR cup is covered with hydroxyapatite (10). The radial clearance levels for the cups are 75–150 µm for ReCap, 50 µm for ASR, and 100 µm for BHR. Cup wall thickness at rim is 3.0 mm for ReCap, 3.1 mm for ASR, and 3.6/4.6 mm for BHR depending on component diameter (15). Synergy, ReCap, and Corail and Summit stems used in THA are all made of titanium alloy (16, 17).
LDH MoM THAs may produce more metal ions than HRA due to wear and corrosion at the junction between the femoral neck and the adapter sleeve and open femoral head design. In the study of Lavigne et al. (10), it was concluded that the cobalt–chromium adapter sleeve of the ASR THA system seems to possess better design characteristics than, for example, the Zimmer device. The cumulative 5-year revision rate in Australia for ASR THA was comparable to that of ASR resurfacing (10.3%, 95% CI = 9.0–11.6 and 10.5%, 95% CI = 8.6–12.7, respectively) (18). In England and Wales, the ASR resurfacing had slightly better 5-year survival than the Corail and Summit/ASR THA (9.6%, 95% CI = 8.3–11.2 and 11.3%, 95% CI = 9.1–14.2, respectively) (19). Our data support the view that ASR THA performs worse than ASR HRA.
The main reason for ASR HRA and ASR THA revision in the current data was aseptic loosening of both components. However, there is no specific question for ARMD as a reason for revision in the Finnish Arthroplasty Register data collection form. Therefore, ARMDs may be falsely coded as aseptic loosenings in the register. ARMD is not always coded as “other reason” either, because there were only 12 ASR HRA revision and 4 ASR THA revisions recorded as “other reason.” The Finnish data collection form is currently being updated in collaboration with the Nordic Arthroplasty Register Association (NARA).
The cumulative 5-year revision rate of BHR THA was higher than that of BHR HRA in Australia (4.9%, 95% CI = 3.8–6.3 and 3.5%, 95% CI = 3.1–3.9, respectively). In addition, the cumulative 7-year revision rate of BHR THA was higher than that of BHR resurfacing (6.7%, 95% CI = 4.8–9.4 and 5.0%, 95% CI = 4.4–5.5, respectively) (18). The stem designs used when performing BHR THA were not set out. In England and Wales, the BHR resurfacing had a 5-year revision rate of 3.4% (95% CI = 3.1–3.8). Equivalent figures for BHR THA were not available (19). There was no statistical significant difference in short-term revision rate between BHR resurfacing and BHR THA in our study. However, the total amount of Synergy/BHR combinations was small (430) compared with BHR resurfacings (1636). It is possible that in Australia, the stems used, but not specified in the register, did not manage as well as the Synergy stem seems to manage in Finland. The short-term survival of the BHR resurfacing in Finland is worse than in Australia and in England and Wales. Despite this, the BHR has been one of the best performing resurfacing designs in Finland (20).
The cumulative 3-year revision rate of ReCap HRA was higher than that of ReCap THA in Australia (6.0%, 95% CI = 3.4–10.7 and 1.9%, 95% CI = 1.1–3.1, respectively). The cumulative 5-year revision rate of ReCap THA was 3.4% (95% CI = 2.1–5.5) (18). The cumulative 5-year revision rate of ReCap HRA was 6.4% (95% CI = 4.1–9.8) in England and Wales. Equivalent figures for ReCap THA were not available (19). There was no statistical significant difference in short-term revision rate between ReCap resurfacing and Bimetric/ReCap in our study. The total amount of Bimetric/ReCap combinations was high (5464). The short-term survival of Bimetric/ReCap with Magnum bearing surface has been promising also in previous studies (3, 21, 22). These data support the Australian finding of low short-term revision rate of ReCap THA.
No difference was found in the risk of dislocation revision between the implant pairs compared. Large head size seems to protect against dislocation, whether the prosthesis head is connected to femoral neck or to femoral component. No difference was found in the risk of revision for periprosthetic fracture between the implant pairs compared. At the early stage, the incidence of calcar fractures after cementless THA and femoral neck fractures after resurfacing seems to be similar. There was no difference in infection revision risk between the three LDH MoM THAs and analogous HRAs either. The supposed protecting effect of antibiotic cement of HRA designs was not supported by our data. LDH MoM THAs are probably performed by a higher numbers of surgeons than the resurfacings in Finland. Hip resurfacing has a reputation of being a relatively difficult procedure, and therefore, it has been centralized in the hands of the most experienced surgeons in many hospitals. However, the total amount of ASR THA and BHR THA in this study was low.
Different studies have shown that over 60° abduction angle might be a significant risk factor for increased metal-ion levels and ARMDs (11, 23). However, in a register-based study with a high number of patients, it is not possible to assess the radiographs of the patients.
In this study, elderly female patients had an increased risk of revision using ReCap HRA compared with ReCap THA. This is probably caused by the high number of femoral neck fractures. Elderly male patients had an increased risk of revision using ASR THA compared with ASR HRA. There was also a tendency for elderly female patients to have an increased risk of revision using ASR THA compared with ASR HRA. ASR THA may perform worse than ASR HRA due to wear of adapter sleeve.
In conclusion, there was no difference in risk for revision between BHR HRAs and THAs or between ReCap HRAs and THAs in short- to mid-term follow-up at a nationwide level. The ReCap LDH MoM adapter sleeve is made of titanium, not of chromium cobalt as in the other two models (10), which may have an effect on the development of ARMD. The revision risk of the ASR THAs was, however, significantly higher than that of ASR HRAs. The true prevalence of ARMD among patients with MoM hip replacements is not yet known, and these results need to be updated annually to see whether there are differences between the HRAs and THAs, as well as between designs from different manufacturers.
Footnotes
Declaration of Conflicting Interests
The authors declare that they have no conflicts of interest to disclose.
Funding
This study was supported by Turku University Central Hospital research project and Sigrid Juselius Foundation.